
Abstract
BACKGROUND:
Real-world safety of bevacizumab in cancer patients is limited.
OBJECTIVE:
To review the adverse drug reactions (ADRs) due to bevacizumab in cancer patients, in published case reports.
METHODS:
PubMed was searched; case reports of patients with any type of cancer, administered with bevacizumab (monotherapy/combination) and reported ADRs were included. Causality of ADRs was presented as reported in individual papers. ADRs were classified using the information in the USFDA-approved prescribing information (PI) of bevacizumab as ‘Serious’, ‘Common’, and ‘Post-marketing surveillance’ ADRs; ADRs not mentioned in the bevacizumab PI were termed as ‘Non-label ADRs’.
RESULTS:
A total of 130 published papers comprising 154 cases from 22 different countries were included. Most papers (102/130; 78.46%) had moderate methodological quality. Age range of patients was 9-77 years. Off-label use of bevacizumab was found in 34/154 cases (22.08%). Ninety-six unique ADRs were found among 154 ADRs; most reported ADRs affected circulatory, digestive, and respiratory systems (33, 32, and 26 cases respectively). Most commonly reported ADRs were posterior leukoencephalopathy, fistulae, and gastrointestinal perforation (17, 17, and 16 cases respectively). Twenty-eight unique non-label ADRs (29.17%) were found.
CONCLUSION:
Bevacizumab is associated with more ADRs in the real world among cancer patients than those reported during clinical trials.
Introduction
Bevacizumab is a humanised recombinant monoclonal antibody which binds to, and neutralizes, all known isoforms of vascular endothelial growth factor (VEGF) A. This prevents the association of VEGF with the endothelial VEGF receptors, primarily Flt-1 and KDR, thereby inhibiting angiogenesis [1]. Bevacizumab was first approved in 2004 as a first line treatment for metastatic colorectal cancer. It was subsequently approved for the treatment of five additional cancers [2]. For a brief duration, bevacizumab was also approved for the treatment of HER2-negative breast cancer [3]. As of November 2019, two biosimilar versions of bevacizumab are available, and both are approved for all indications of bevacizumab except ovarian, fallopian tube and primary peritoneal cancers [4]. Bevacizumab has been used off-label for treatment of cancers as well as certain non-cancer conditions [1].
Over the course of the regulatory cycle of bevacizumab approval, some adverse drug reactions (ADRs) which had serious, fatal, or clinically significant consequences (requiring dosage modification/avoidance of bevacizumab) were observed in clinical trials. These ADRs include gastrointestinal (GI) perforation and fistulae, surgery and wound healing complications, hemorrhage, arterial and venous thromboembolic events, hypertension, posterior reversible encephalopathy syndrome (PRES), renal injury and proteinuria, infusion-related reactions, ovarian failure, and congestive heart failure (CHF). All of these have been listed in the USFDA-approved prescribing information (PI) of bevacizumab and its biosimilars [2]. Apart from these clinically significant ADRs, the bevacizumab PI also mentions ‘Common’ ADRs which have been observed in over 10% of bevacizumab recipients, as reported in various clinical trials; these include epistaxis, headache, hypertension, rhinitis, proteinuria, taste alteration, dry skin, rectal hemorrhage, lacrimation disorder, back pain and exfoliative dermatitis. A third category of ADRs that are listed in the PI are those ADRs which are reported from various post-marketing surveillance (PMS) studies, and these include polyserositis, pulmonary hypertension, mesenteric venous occlusion, GI ulcer, intestinal necrosis, anastomotic ulceration, pancytopenia, gallbladder perforation, osteonecrosis of the jaw, renal thrombotic microangiopathy, and nasal septum perforation. Both the biosimilars of bevacizumab carry a similar ADR profile [5,6]. In the latest update of the PI of bevacizumab during June 2019, the USFDA removed the boxed warning for gastrointestinal perforations, surgery and wound healing complications, and severe or fatal pulmonary, gastrointestinal, central nervous system, and vaginal hemorrhage [7].
Although there are several studies that assess safety data of bevacizumab in a randomized controlled trial (RCT) setting, data pertaining to the adverse effect profile of bevacizumab in a real-world setting is limited. In this review, we aim to explore the ADRs due to bevacizumab in cancer patients, in published case reports, which are indicative of a real-world setting.
Materials and methods
All published articles were searched for eligibility using the following approach. “Population” were all case series and case reports which included patients with any cancer who were given bevacizumab either as a monotherapy or in combination of other anticancer drugs or radiotherapy. There was no restriction on age, or gender of the patients, or type of cancer. “Intervention” included bevacizumab given at any dose and duration, either alone or in combination regimens. “Comparator” was excluded, because the types of papers being searched were case reports and case studies. “Outcome” included any adverse drug reaction (ADR) with or without causality assessment. We only included papers published in the English language, since our team of reviewers was proficient in this language. We excluded any type of research papers, apart from case series and case reports, which analysed animal studies, or any patients who were given bevacizumab for non-cancer indications. The study protocol used for the review was not registered in the PROSPERO database.
A systematic literature search was performed in MEDLINE/PubMed from their inception until January 24, 2019, using a combination of search terms and Boolean operators (“Bevacizumab” OR “Mvasi” OR “Bevacizumab-awwb” OR “Bevacizumab awwb” OR “Avastin”) for case reports and case series published in the English language. Using the above eligibility criteria, the titles and abstracts of all retrieved records were independently scanned by two reviewers (JVR and RK). Full texts of the potentially relevant records were assessed for eligibility, and any disagreements were discussed and resolved with the help of a third reviewer (VBN). Additionally, reference lists of the eligible papers were also hand-searched to identify other eligible records.
Once all the eligible records were pooled, two independent authors (JVR and RK) extracted the data from the papers into a predefined data table after reading through the full texts of the individual case reports. Methodological quality of the included studies was assessed using the tool proposed by Murad et al., with suitable modifications for case reports describing ADRs as suggested by the authors, and the overall quality of each paper was assessed as ‘high’, ‘moderate’, or ‘low’ based on their completeness in four domains (selection, ascertainment, causality, and reporting) [8]. Disagreements between the two authors with respect to data extraction and quality assessment were resolved with the help of another author (VBN).
ADRs were classified using the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10), version 2019. For the purpose of this study, when bevacizumab was used for a condition that was mentioned in the PI as an approved indication, it was termed as ‘On label’ use, and other uses were termed as ‘Off-label’ uses. The ADRs were classified using the information in the PI into ‘Serious ADRs’ (clinically significant ADRs listed under section 6 of the PIs), ‘Common ADRs’ (ADRs occurring at a rate of >10%, as listed under section 6.1 of the PIs), and ‘PMS ADRs’ (ADRs identified during post-approval use of bevacizumab, as listed under section 6.3 of the PIs) [2,5,6]. Those ADRs which were not mentioned in the bevacizumab PI were termed as ‘Non-label ADRs’. Causality of ADRs was presented as reported by the physicians in the respective case reports.
All data was entered electronically and analysed in Microsoft Excel. Inter-rater reliability (IRR) and Cohen’s kappa were calculated using SPSS version 20. The cut-offs for kappa statistic were interpreted as ≤0.20 = slight agreement; 0.21–0.40 = fair agreement; 0.41–0.60 = moderate agreement; 0.61–0.80 = substantial agreement; 0.81–0.99 = near-perfect agreement; and 1.00 = perfect agreement [9]. SPSS version 20 was used to apply Chi-square test for comparing ADR distribution under various headings. A p value of ≤0.05 was considered statistically significant for all tests performed.
Results
A total of 130 papers (116 individual case reports and 14 case series) comprising 154 case reports published between 2006 and 2018 were included in this literature review. The study selection process is depicted in Fig. 1. The IRR for selection of papers for review between the two reviewers was substantial, with Cohen’s kappa value being 0.751 and 0.677 for article screening and eligibility assessment respectively. The methodological quality of most of the papers was ‘moderate’ (102/130), with 8 papers having ‘high’ methodological quality, and 20 papers having ‘low’ methodological quality. The IRR for methodological quality assessment was substantial, with the Cohen’s kappa value being 0.69. The 130 included papers came from across the world, representing 22 different countries belonging to all populated continents except Africa, the most numerous being from the USA (42 papers), followed by Japan (22 papers) and France (13 papers). A complete list of all the 130 papers included in this overview is provided in Supplementary Table S1.
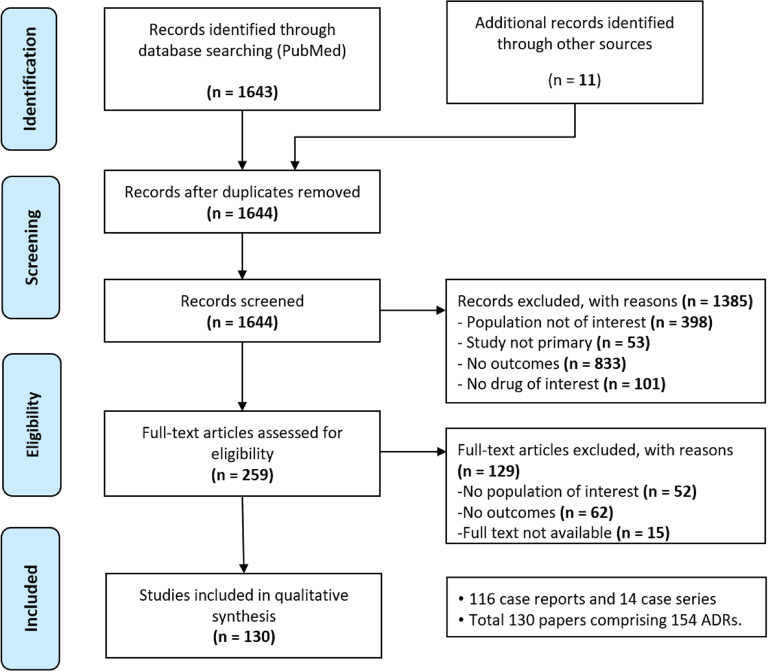
Selection process of the study.
Out of the 154 cases, 81 were females and 73 were males. The mean age was 52.68 ± 14.11 years (range: 9 to 77 years). The median age was 57 years among male patients and 53 years among female patients. Most ADRs were seen in the 61–70 years age group among males (n = 26) and 51–60 years age group among females (n = 28).
Indications and treatment
The most frequent diagnosis was colorectal cancer (n = 61; 39.61%) followed by NSCLC (n = 27; 17.53%) and breast cancer (23; 14.94%). Off-label use of bevacizumab was found in 34/154 cases (22.08%) (Table ). Bevacizumab was used as monotherapy in 21 cases, and as a part of over 40 different combination regimes in the remaining 133 cases. The most common combinations with bevacizumab were the FOLFOX regimen (folinic acid, fluorouracil, oxaliplatin) in 21 cases, and the FOLFRI regime (folinic acid, fluorouracil, irinotecan) in 20 cases, and paclitaxel in 16 cases. A comprehensive list of all combination regimes seen in our study is available in Supplementary Table S2.
Indications for the use of bevacizumab seen in our overview
Indications for the use of bevacizumab seen in our overview
Note: ∗These include Adenocarcinoma of parotid gland, bladder cancer, cholangiocarcinoma, non-melanoma skin cancer, prostate cancer, and ependymoma.
A total of 96 unique ADRs were found among the 154 ADRs. The largest number of ADRs were related to circulatory system (n = 33, 24.03%) followed by digestive (n = 32, 20.78%) and respiratory system (n = 26, 16.88%) respectively (Table 2). The most frequently reported ADRs were PRES (posterior reversible encephalopathy syndrome), fistulae (gastrointestinal, pulmonary, and colovaginal), gastrointestinal perforation, and nasal septal perforation with 17, 17, 16, and 10 cases respectively. A comprehensive list of all ADRs seen in our study is available in Supplementary Table S3. Most of the ADRs were similarly distributed among both male and female patients (Table 2).
Details of ADRs classified per system/organ affected
Details of ADRs classified per system/organ affected
Note: P value by Pearson Chi square test. MT = Monotherapy; CT = Combination therapy; PI = Prescribing information. ∗ = significant difference (p <0.05).
Out of the 34 times where bevacizumab was used for an off-label indication, GI perforation (n = 5) and perforation of the nasal septum (n = 4) were the most frequently occurring ADRs; there were 3 cases each of PRES and wound healing-related ADRs. Thirteen of these 34 ADR were not mentioned in the USFDA label; notably, there were three cases each of osteonecrosis and vocal hoarseness among these. The cause of the ADR was reasonably proven to be bevacizumab (by means of demonstrating improvement after bevacizumab withdrawal) in 14/34 cases.
The list of ADRs classified based on occurring with bevacizumab monotherapy and combination therapy is provided in Table 3. The causality of the ADR was reasonably established as bevacizumab in 53/154 (34.42%) cases, including the 21 cases where bevacizumab was used as monotherapy, and in 32/133 (24.06%) cases of combination therapy where improvement in the ADR was demonstrated with withdrawal of bevacizumab.
ADRs seen with bevacizumab monotherapy and combination therapy
Note: FOLFRI: Irinotecan + folinic acid + fluorouracil; FOLFOX: Folinic acid + fluorouracil + oxaliplatin; PRES: Posterior reversible leukoencephalopathy syndrome; GI: gastrointestinal.
A total of 52/154 ADRs (33.77%) comprising 28/96 unique ADRs (29.17%) were not mentioned in the USFDA-approved PI of bevacizumab (Table 2). Among these 52 ADRs, the most frequently reported ADRs were osteonecrosis not involving the jaw (six cases) and neurotoxicity (six cases), followed by vocal hoarseness (four cases) and radiation pneumonitis (four cases). However, the cause of the ADR was reasonably proven to be bevacizumab (by means of demonstrating improvement after bevacizumab withdrawal) in only 20 of these 52 cases (38.46%) comprising 10 different ADRs, which included all six cases of osteonecrosis, neurotoxicity, and vocal hoarseness, skin rash/ulcers, and interstitial nephritis among others (Fig. 2). Out of the 102 ADRs mentioned in the bevacizumab PI, 79 were ‘Serious ADRs’, and 23 were ‘PMS ADRs’; no ‘Common ADR’ was retrieved from the included case reports.
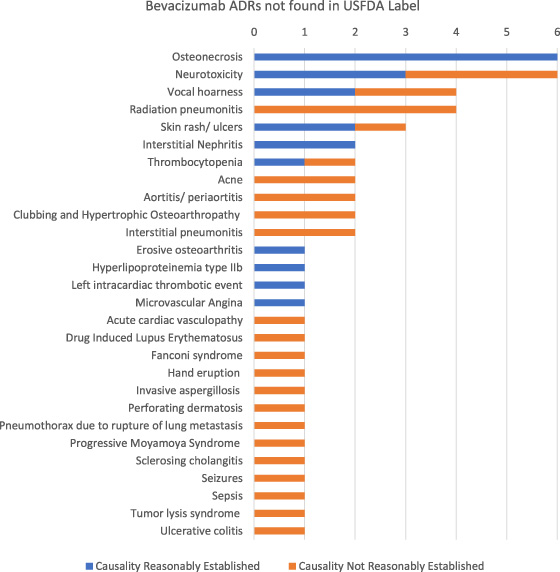
Bevacizumab ADRs were not found in the USFDA label.
Bevacizumab has been in use for close to 15 years, and its efficacy and safety data are emerging on a real time basis. By blocking the working of VEGF receptors located throughout the body, bevacizumab inhibits microvascular growth, thereby retarding the growth of all tissues, including cancerous tissues [1]. This property of retarding the angiogenesis and growth of all tissues in the body is both advantageous (can be used to treat multiple disorders) and disadvantageous (can cause varied ADRs). This fact also makes it necessary to regularly update the safety and efficacy profiles of bevacizumab, for effectively understanding the treatment implications and management of patients.
The recent revision of bevacizumab PI was done in June 2019 wherein the boxed warnings for some serious ADRs were removed [2,5–7]. However, new ADRs were not added in the updated PI. Our study included papers published up to January 2019, and around one-third of the ADRs that we observed in these case reports were not found in the recently updated PI. Out of these non-label ADRs, the causality with bevacizumab was reasonably proven for ADRs such as osteonecrosis not involving the jaw, neurotoxicity, vocal hoarseness, skin rash/ulcers, and interstitial nephritis. These ADRs might not have been reported with an increased incidence in the RCT settings to merit an inclusion into the PI, but the fact that these are increasingly observed in the real world setting suggests that the PI would be more comprehensive if real-world studies (such as case series and case reports, in addition to the regulatory updates from the pharmaceutical companies) are also considered. The possibility of these ADRs being already communicated to the USFDA as a part of the regulatory requirements cannot be ruled out.
It is interesting to observe that while the bevacizumab PI lists osteonecrosis of the jaw as a PMS ADR, in our review we found six cases each of osteonecrosis of jaw and osteonecrosis affecting another bone. Further, none of the seven dermatological ADRs and vocal hoarseness that we observed in our review was mentioned in the PI. We also observed that bevacizumab resulted in unique ADRs when it was used in 34 cases of off-label indications, in a real-world scenario. These observations highlight the importance of including the information from real-world studies.
Real-world studies have their own advantages, which makes it necessary to consider them in addition to the RCTs. Real world data includes all the data that are used for decision-making that are collected in studies apart from RCTs. These include non-randomized trials, case series and case reports, observational studies, and physician experience surveys where randomization has not been done. The real-world data is considered to complement the data from RCTs, and while there is discordance, the data from RCTs is given a higher value [10].
Case reports and case series typically occupy the lowest rung in the ladder of evidence, whereas RCTs, systematic reviews and meta-analyses of RCTs are at the top. Case series and case reports however do serve as an important starting point for hypothesis generation [11]. Systematic reviews of case series and case reports have not been done as frequently as the systematic reviews of RCTs. Synthesizing data from case reports is not comprehensive because of inherent selection bias: only interesting cases with unique ADRs are reported and published, and the common ADRs that are well-known in literature or in regulatory listings are not published [11]. However, observing a pattern in such unique ADRs may help to identify trends that are rare but serious.
The most important strength of our study is the high IRR observed between the reviewers, which indirectly suggests that the data synthesis has been done with a low risk of bias. Perhaps the greatest limitation of our study is that of publication bias as explained previously. Second, we focussed only on case series and case reports to highlight their importance in literature as sources of real-world evidence; however, by doing so we might have missed out on other sources of information on ADRs, including observational studies and pharmacovigilance reports. Third, we restricted to searching only the MEDLINE/PubMed database; inclusion of other databases might have provided a larger number of eligible case reports. Fourth, we did not register our review protocol with any database such as PROSPERO. Next, we did not asses the correlation of ADRs with indications, nor did we analyse the dose-response relationship between bevacizumab and the ADRs. Finally, we did not include the list of ADRs associated with bevacizumab as maintained by the WHO program for international drug monitoring or in any national database, since we were interested to identify the ADRs published in case reports and case series.
Conclusions
Our overview of case reports for ADRs of bevacizumab in the real world suggests that bevacizumab is associated with more ADRs in the real world among cancer patients than those reported during clinical trials. We also found 28 ADRs which are not presently listed in the PI of bevacizumab, the most important of which include osteonecrosis not involving the jaw, neurotoxicity, and vocal hoarseness, skin rash/ulcers, and interstitial nephritis. Randomized studies and targeted data collection are essential to confirm the findings of our overview. Inclusion of real-world studies while preparing regulatory documents such as PIs should be given a serious consideration for the benefit of all recipients, and a framework for this should be developed.
Footnotes
Author contributions
AD: study design, and reviewing the manuscript. JVR: study design, literature search, screening and curation, data extraction, and reviewing the manuscript. RK: literature search, screening and curation, and data extraction. VBN: statistical analysis, resolution of disagreements during data curation, and preparing, revising and editing the manuscript.
Conflict of interest
All authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Funding
This study was self-funded by the authors.