
Abstract
BACKGROUND:
The vaccine/autism controversy has caused vast scientific and public confusion, and it has set back research and education into genuine vaccine-induced neurological disorders. The great strawman of autism has been so emphasized by the vaccine industry that it, and it alone, often appears in authoritative discussions of adverse effects of the MMR and other vaccines. By dismissing the chimerical vaccine/autism controversy, vaccine defenders often dismiss all genuinely neurological aftereffects of the MMR (measles, mumps, and rubella) and other vaccines, including well-documented events, such as relatively rare cases of encephalopathy and encephalitis.
OBJECTIVE:
This report explains that autism is not a physical or neurological disorder. It is not caused by injury or disease of the brain. It is a developmental disorder that has no physical origins and no physical symptoms. It is extremely unlikely that vaccines are causing autism; but it is extremely likely that they are causing more neurological damage than currently appreciated, some of it resulting in psychosocial disabilities that can be confused with autism and other psychosocial disorders. This confusion between a developmental, psychosocial disorder and a physical neurological disease has played into the hands of interest groups who want to deny that vaccines have any neurological and associated neuropsychiatric effects.
METHODS:
A review of the scientific literature, textbooks, and related media commentary is integrated with basic clinical knowledge.
RESULTS:
This report shows how scientific sources have used the vaccine/autism controversy to avoid dealing with genuine neurological risks associated with vaccines and summarizes evidence that vaccines, including the MMR, can cause serious neurological disorders. Manufacturers have been allowed by the US Food and Drug Administration (FDA) to gain vaccine approval without placebo-controlled clinical trials.
CONCLUSIONS:
The misleading vaccine autism controversy must be set aside in favor of examining actual neurological harms associated with vaccines, including building on existing research that has been ignored. Manufacturers of vaccines must be required to conduct placebo-controlled clinical studies for existing vaccines and for government approval of new vaccines. Many probable or confirmed neurological adverse events occur within a few days or weeks after immunization and could be detected if the trials were sufficiently large. Contrary to current opinion, large, long-term placebo-controlled trials of existing and new vaccines would be relatively easy and safe to conduct.
Introduction: Origins of the controversy
In 2001 a now-discredited article was published in The Lancet by Wakefield et al. claiming to make a connection between MMR vaccines (the measles component) and autism, initiating an international storm of controversy (described in [1–3]). The study had such an enormous impact because previous reports had appeared in more obscure journals and, overall, there was no body of scientific evidence for the hypothesis. In addition, Wakefield publicized the issue and many parents felt relief at having a physical explanation for their children’s developmental disorders [4]. These events led to an abrupt rise in claims made to the Vaccine Injury Compensation Program with a 2002 spike at more than 12 times the total of all other cases brought [5] (Fig. 1).
Vaccine advocates quickly attacked the article and Wakefield himself. The article was withdrawn by The Lancet and Wakefield lost his license to practice medicine in Great Britain [6]. Meanwhile, the peak of autism complaints began a steep decline from its 2002 peak until in 2006–2007 it no longer exceeded the total of other claims.
Following the attack on Wakefield and the withdrawal of the article, the medical, scientific, and legal community dismissed any claims for a possible connection between vaccines and autism. To this day, the CDC [7], the American Academy of Pediatrics [8], and multiple scientific sources continue to conclude that there is no evidence to relate vaccines to autism [1,9,10].
The absence of authoritative medical support does not mean that a hypothesis or theory is wrong. Where financially valuable products, such as vaccines or psychiatric drugs, are at stake, corruption in science is commonplace and medical denial of harms is rampant [11–15]. However, this author has been unable to find any articles linking vaccines to autism that provide even brief clinical descriptions of actual autism cases.
Vaccines: A very unlikely cause of autism
Autism and autism spectrum disorders are not acquired through harms to the brain. Vaccines cannot cause autism because autism is a developmental disorder and not a physical disorder. Confusing autism with a physical disorder and, conversely, confusing a physical disorder with autism, are both scientific mistakes. All or nearly all the identified victims of vaccination injury, as one would expect from a physical cause, have physical symptoms, often reflecting neurological harms. When neurological harms are present, the diagnoses must reflect the neurological disorders, such as encephalitis or encephalopathy, and not any symptoms which happen to resemble autism, attention-deficit hyperactivity disorder (ADHD), or oppositional defiant disorder (ODD).
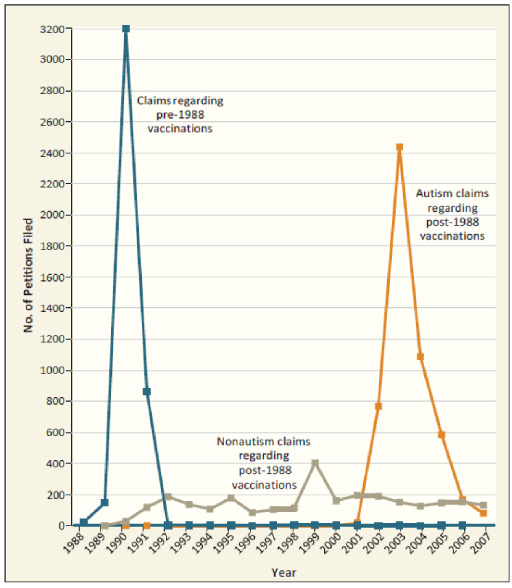
Claims filed with the Vaccine Injury Compensation Program, 1989–2007. Post-1988 vaccinations are those that occurred on or after October 1, 1988; pre-1988 vaccinations are those that occurred before that date. Data are from the Health Resources and Services Administration.
The article by Wakefield et al. illustrates a central problem in the vaccine/autism controversy—the failure to adequately describe the syndrome and to distinguish it from neurological disorders. In Wakefield et al., there was great emphasis on autism in the table; but no descriptions of the syndrome or even the sources of the diagnosis. The children were very ill with gastrointestinal disorders and many had been through neurological crises, such as encephalitis, high fever, and seizures.Two of the patients had a dramatic deterioration or regression in function, which is much more characteristic of physical disorders than of autism. Nearly all the others had specific signs of physical injury at the onset, which is also not characteristic of autism. Finally, despite the diagnostic tables, in the text the authors seem to suggest that there were no consistent psychiatric syndromes: “Despite consistent gastrointestinal findings, behavioural changes in these children were more heterogeneous” (p. 640). They also used the broad, nonspecific term “neuropsychiatric dysfunction” in describing their findings (p. 640). All that should have ended the autism controversy, but it did not, and Wakefield continued to promote the theory that vaccines can cause autism.
Instead, the broad, nonspecific terms at times used in Wakefield et al., such as “neuropsychiatric dysfunction” and “heterogeneous” behavioral changes, invite the conclusion that there were many diverse causes for the psychological and developmental problems in these children. Their gastrointestinal problems caused physical pain, social disability, stigma, multiple doctor visits, and overall stress as it does in any group of sick children suffering from colitis [16]. They may also have suffered lasting effects from encephalitis or other disorders that may or may not have been caused by the MMR vaccine. In addition, their parents would have been under stress from taking care of them.
Modern psychiatric theory and practice has abetted the tendency to confuse non-physical developmental and psychosocial disorders such as autism with genuinely biological disorders. This is epitomized in the evolution of the editions of the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders. The First Edition began by distinguishing psychogenic disorders from disorders of unknown etiology and from biologically based disorders [17]. By contrast, the Third Edition in 1980 assumes that all psychiatric disorders are physical in origin and medical in conceptualization (see the discussion of the transition in [18], p. 1–2). The most recent edition (2013) completely blurs the distinction between psychosocial disorders and disorders of unknown etiology or orders of biological origin. The “medical model” is impressed on every diagnosis.
As an illustration, lead poisoning in children can cause encephalopathy at higher doses and a wide range of adverse effects in lower ranges, including cognitive decline, developmental delays, and behavior problems [19] (p. 3798). A proper understanding of these disorders requires their direct association with brain damage or dysfunction caused by lead intoxication, rather than mistakenly labelling them as if they were psychosocial diagnostic entities such as autism, ADHD, or Oppositional Defiant Disorder.
If vaccines do not cause the classic syndrome of autism, why is this article necessary? It is necessary because the chimerical vaccine/autism controversy has become a cudgel used by more absolutist defenders of vaccines to stifle the examination of any possible or potential connections between vaccines and genuine neurological injuries that might at times resemble autism without being autism. The vaccine/autism controversy has also been used as a distraction when authoritative sources announce that the MMR cannot cause autism—and then proceed to mention no other possible neurological injuries from the vaccine. Dismissively declaring that the MMR vaccine cannot cause autism has become a substitute for researching or describing those neurological it may cause (see ahead).
It is widely recognized that the MMR can, on rare occasion, cause encephalopathy. Weibel et al. 1 (see below) reviewed claims submitted to the National Vaccine Injury Compensation Program and concluded that the MMR was causing encephalopathy, which they defined as “acute encephalopathy followed by permanent brain injury or death” associated with the administration of attenuated measles vaccines. This is vaccine-related disorder has been easier to detect than other adverse effects because it usually occurs in close temporal proximity to the vaccination. As determined by WHO [20] (p. 46), encephalopathy is considered reportable only if it occurs 6–12 days after measles/MMR vaccine and only 0–2 days after DPT vaccines.
Encephalopathy is a broad term that simply means disease of the brain. However, in practical use it is usually used, as in the WHO instance, to designate the aftermath of serious injury caused by a specific cause, such as infection or vaccination. The existence of such a potential severe, ill-defined potentially lethal affliction from the MMR vaccine should lead to serious concern about lesser neurological impairments that are being overlooked. The section in this report titled “The Absence of Placebo Controls in Vaccine Trials for FDA-Approval” will discuss the importance of clinical trials in detecting adverse events that occur a short time after immunization.
Bleuler originally used the term autism in a 1908 journal article and incorporated it into his medical book, Dementia Praecox, as “autismus” [21] (p. 304) to describe aspects of withdrawal into fantasy life in schizophrenia. However, the clinical the use of the term in the context of what is now called schizophrenia has faded. Leo Kanner discovered and defined the psychosocial syndrome of autism as wholly distinct from schizophrenia and with its own unique characteristics, and that definition remains in use today.
Autism as originally described by Leo Kanner is a developmental condition that has no specific relationship to any medical symptoms or diseases and this description persisted throughout his work [22,23]. In his seminal article in 1943, Kanner described these children as essentially unable to relate to people as if they are alive and human. Instead, they treat others as objects. When autistic children do relate to people, they may focus on them as one would physical objects or even as parts of objects, rather than as people with whom to share feelings or to have empathy:
Objects that do not change their appearance and position, that retain their sameness and never threaten to interfere with the child’s aloneness, are readily accepted by the autistic child. He has a good relation to objects; he is interested in them, can play with them happily for hours. He can be very fond of them, or get angry at them if, for instance, he cannot fit them into a certain space. (p. 246)
The children’s relation to people is altogether different. Every one of the children, upon entering the office, immediately went after blocks, toys, or other objects, without paying the least attention to the persons present. …Comings and goings, even of the mother, did not seem to register. Conversation going on in the room elicited no interest. If the adults did not try to enter the child’s domain, he would at times, while moving between them, gently touch a hand or a knee as on other occasions he patted the desk or the couch. But he never looked into anyone’s face. If an adult forcibly intruded himself by taking a block away or stepping on an object that the child needed, the child struggled and became angry with the hand or the foot, which was dealt with per se and not as a part of a person. He never addressed a word or a look to the owner of the hand and or foot. …When pricked, he showed fear of the pin but not of the person who pricked him. (p. 246–247)
Kanner described the probable origins of this startling lack of human engagement in these children:
In the whole group, there are very few really warm-hearted fathers and mothers. For the most part, the parents, grandparents, and collaterals are persons strongly preoccupied with abstractions of a scientific, literary, or artistic nature, and limited in genuine interest in people. Even some of the happiest marriages are rather cold and formal affairs. (p. 250)
Continued failures to find a physical basis for autism
No consistent physical causes, physical markers or symptoms have ever been established for autism. None are included in the criteria of the American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders (DSM) from the 3rd edition (1968), when it first appeared, to the current 5th Edition (2013). Consistent with the DSM, Adams and Victor’s Textbook of Neurology [24] stated, “The basis of childhood autism is as much a mystery today as it was when Kanner and Asperger described it. Most of the children are physically normal except for larger head size, on average, but with no other somatic abnormalities” (p. 1076–1077). They added, “no environmental factors, including the often-mentioned measles-mumps-rubella (MMR) vaccination, mercury exposure, and food allergies, have been credibly connected to autism” (p. 1077).
Using the chimerical vaccine/autism to stifle research and accurate disclosures
Autism became the buzz word—more nearly the cudgel—used to discourage, dismiss, and ignore the multiple potential vaccine harms discussed in many articles in the scientific literature (see below). The controversy is used as a rug under which to sweep and hide the many more obvious neurological and neuropsychiatric adverse effects caused by vaccines. When discussing vaccine adverse effects involving the brain, which include encephalitis, authoritative medical sources routinely state that there is no evidence that vaccines cause “autism,” while neglecting to discuss the more probable or well-documented harms to the brain, mind and behavior.
As an example, in 2002, a review titled “Neurological adverse events associated with vaccination” was published in Neurology [25]. The authors wrote, “The present review provides an update on progress in the adverse central nervous system events that are associated with vaccines. Only major studies that showed evidence to substantiate such associations are considered here” (p. 333). The MMR vaccination section was the only one with no references to any known adverse events. Instead, the entire 350-word MMR section, one of the longer ones, was devoted entirely to critiquing Wakefield et al. and the alleged connection between MMR and autism. Thus, the authors and the important journal, Neurology, used the urgency of the false vaccine/autism controversy to avoid linking the MMR to any adverse effects whatsoever in a major review. No other vaccine escaped from having some adverse neurological effects.
Making a scapegoat of the MMR/autism controversy persists. The following excerpt covers the entire discussion of hazards of MMR vaccine directed at family physicians by Spencer et al. in an article in the American Family Physician entitled “Vaccine Adverse Events: Separating Myth From Reality”:
An article linking autism to the MMR vaccine was retracted for fraud, but this misinformation persists and has caused long-lasting public health consequences. Multiple studies have found no causal link between vaccination and autism, but the falsified report continues to cause parental concern. Physicians must acknowledge these fears and inform concerned parents about the benefits of immunization and the potential harm of vaccine refusal. Febrile seizures that occur seven to 10 days after the first dose of the MMR vaccine are uncommon, but the risk is increased when the first dose is given after the recommended age of 12 to 15 months. The risk of immune thrombocytopenic purpura is increased after both natural measles infection and for up to six weeks after MMR vaccination (Table 2). Infection with measles, mumps, or rubella causes more severe adverse effects than the MMR vaccine, and vaccine refusal has been linked to recent outbreaks of these infections. (p. 787–789)
In the above excerpt, the attack on Wakefield et al. coopts the entire discussion of potential neurological harms from the MMR.
The prestigious tome, Nelson Textbook of Pediatrics [19], exemplifies the cover up. It barely touches on vaccine adverse effects and, in respect to the MMR or MMRV, it is no more informative than Spencer et al.’s American Family Physician article. Almost all the pediatric textbook has to say about neurological effects occurs in this one sentence: “Encephalopathy and autism have not been shown to be causally associated with the measles-mumps-rubella vaccine or vaccine constituents” (p. 1675). The use of the word “autism” is most remarkable in this context because there are so many neurological syndromes associated with the MMR vaccine that the autism controversy, by comparison, deserves no attention at all. Once again, autism becomes chimerical rug under which all the neurological or neuropsychiatric vaccine harms will be hidden.
Without any citation, the pediatric textbook also dismisses any danger of the vaccine causing SSPE (Subacute sclerosing panencephalitis), although it is the most frequently reported adverse effect in postmarketing of the virus (see ahead).
Evidence for neurological injury caused by MMR and other vaccines
According to Williams et al. [26], “In 2004 the Clinical Consult Case Review (CCCR) working group was formed within the CDC-funded Clinical Immunization Safety Assessment (CISA) Network to review individual cases of adverse events following immunizations (AEFI).” Their approach was not able to determine the frequency of adverse events but noted that, across a broad spectrum of vaccines, neurological events were the most-commonly reported adverse events by their sources and in the scientific literature.
The individual cases of neurological events evaluated by Williams et al. [26] as “probable” or “possible” were:
Brachial neuritis, status epilepticus, cerebellar ataxia, periodic myalgia, neuritis, inconsolable crying, bulging fontanelle, fussy, transverse myelitis, chronic inflammatory demyelinating polyneuropathy, transverse myelitis, meningitis/meningoencephalitis, facial diplegia, and acute polyneuropathy. (Table 3, p. 6923)
The above list of disorders, which includes “inconsolable crying” and “fussy” among a variety of known neurological disorders, exemplifies the confusion of failing to distinguish between an organic, physical or neurological disorder and a psychological or behavioral symptom that results from it. A child with a mild brain injury that has caused social withdrawal, distractibility, irritability, or apprehensiveness should not be diagnosed with autism, attention-deficit hyperactivity disorder (ADHD), Oppositional Defiant Disorder (ODD) or an anxiety disorder. Given the broad range of potential neurological adverse effects from vaccines, it is important to avoiding becoming distracted by symptoms that probably reflect on an underlying and perhaps subtle case of a physical disorder, in particular a generalized mild brain dysfunction diagnosable as a minor neurocognitive disorder [27] or a mild case of chronic brain impairment (CBI) [28]. Encephalitis, for example, can result in many psychological or psychiatric symptoms from psychosis and dementia to personality changes, which may show up during the acute phase of the disorder or years afterward [29].
The 2020, FDA-Approved Full Prescribing Information for ProQuad, a “Measles, Mumps, Rubella and Varicella Virus Vaccine Live Suspension for subcutaneous injection,” has a lengthy post-marketing adverse event section. Merck & Co. [30] are the sole providers of the MMR vaccine in the United States, and hence the only source for information about its testing. Here are excerpts from the post-marketing reports for two categories that have most of the neurological adverse effects:
The following adverse events have been identified during post-approval use of either the components of ProQuad or ProQuad. Because the events are in some cases described in the literature or reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to vaccine exposure.
Infections and infestations
…
Nervous system disorders
The extremely broad array of potential neurological disorders, many of them most likely appearing soon after the vaccine exposure, points to the necessity of requiring placebo-controlled clinical trials for the approval of new vaccines and to test older ones, even if only for adverse effects (see ahead). It also points to the vast potential for children and adults developing a broad array of psychological symptoms in response to vaccine-injury to the brain.
In each category, the adverse effects are ordered by frequency, so that the most frequent are listed first and the least frequent last. Notice the numerous forms encephalitis and meningitis are listed first as the most frequent adverse events. Although causality cannot be proven for any one of the events reported to the FDA, patterns like this do provide considerable evidence that many of the reports are probably caused by the vaccine.
Subacute sclerosing panencephalitis (SSPE) is the most frequently reported infectious adverse event related to the vaccine. This presents several difficulties. First, it is “nearly always fatal” and, second, it has a long-delayed appearance 7–10 years after apparent recovery from the virus when the agent seems to reactivate [19] (p. 1773-1674). As noted earlier, despite these reports enumerated by the manufacturer, the risk from vaccination is dismissed by Nelson Textbook of Pediatrics without so much as a citation.
Measles inclusion body encephalitis, as its name suggests, is caused by measles and, as the postmarketing reports confirm, it can be caused by Merk’s live virus vaccine. Reports concerning the clinical features and course of the vaccine-induced encephalitis are relatively sparse, but it can cause death.
There is a mistaken belief that pharmaceutical companies try to pad their Full Prescribing Informations with many adverse events. In that way, they supposedly cover themselves from being sued for failing to warn about the possible array of harms. This is not true. As a psychiatrist and scientific expert in product lawsuits against pharmaceutical companies, I have seen drug companies fight with all their might to prevent any hint that their products might have serious side effects [11–13]. Yes, the companies do strive to pad their educational information with relatively minor adverse effects to allay and distract the reader; but they try harder to prevent any serious harms from being seen by doctors and consumers.
As noted earlier, Weibel et al. reviewed claims submitted to the National Vaccine Injury Compensation Program and concluded that the MMR was causing encephalopathy, which they defined as “acute encephalopathy followed by permanent brain injury or death” associated with the administration of further attenuated measles vaccines. After reviewing the case reports on encephalopathy, they concluded, “This clustering suggests that a causal relationship between measles vaccine and encephalopathy may exist as a rare complication of measles immunization” (p. 383). Given the vagueness of the term “encephalopathy,” more research focus must be given to a broad array of potential injuries resulting from vaccine-induced minimal or missed cases of encephalitis, meningitis, or any number of flu-like or measles-like infections that can compromise brain function.
Consistent with the findings of Weibel et al., the national Vaccine Injury Table [31] of the National Vaccine Injury Compensation Program, which specifies certain vaccine related injuries that are accepted for compensation from the federal government, recognizes “encephalopathy or encephalitis” (p. 1). These are the same vaccine-induced disorders denied by many other authoritative sources, including Nelson Textbook of Pediatrics.
Analysis based on the vaccine adverse events reporting system (VAERS), 1994–2000
Geier and Geier [32] evaluated the neurological adverse effects of the live, combined MMR vaccination:
In this study, the VAERS database was analyzed retrospectively for serious neurologic symptoms following primary pediatric MMR immunization from 1994 through 2000 that developed within 30 days among those residing in the US. The serious neurologic adverse reactions analyzed included: cerebellar ataxia, autism, mental retardation and permanent brain damage. (p. 204, bold added)
In the above paragraph, the study finds that “autism” can be caused by the MMR vaccination, but incorrectly lumps it with neurological disorders. From the data, there is no way to determine if these reports of autism represent anything more than they seem to have represented in Wakefield’s study, which was probably a wide variety of psychiatric or psychological symptoms potentially associated with brain injury or other physical illnesses.
When they compared the MMR to reports for another vaccine, the MMR adverse effects were significant:
Cerebellar ataxia, autism, mental retardation and permanent brain damage were all statistically significantly increased following primary MMR vaccination in comparison to DTwcP 2 vaccination. (p. 205)
They expressed the source of their concerns:
It has recently been hypothesized that by combining the three live viral components of MMR vaccine that there is an increased severity of adverse reactions following MMR vaccination than would be expected based upon the reactogenicity profiles of each of the component vaccines of MMR vaccine administered individually. We have analyzed other studies that have examined the reactivity of individual components of MMR and combined MMR vaccines, and found this to be true. (p. 207)
They found their concerns confirmed:
In conclusion, this study showed a highly statistically significant increase in serious neurologic conditions following primary pediatric MMR vaccination in comparison to a DTwcP vaccine control group. This finding confirms and extends a number of previous studies showing that patients are at increased risk for developing serious neurologic disorders for about
The warning that patients are at serious risk of neurological disorders in the first 5–10 days should have been an alert to the FDA to conduct genuine placebo-controlled clinical trials for vaccines for both the approval of new vaccines and the review of older ones.
In another study based on the VAERS data, Geier and Geier [33] found a significantly higher rate of serious adverse effects in an early pertussis vaccine, whole-cell DTP, compared to a more recent one, acellular DTaP. They concluded, “this analysis demonstrates that the temporal association between whole-cell DTP vaccination and a myriad of serious adverse reactions is not due to coincidence. It is believed that the high levels of endotoxin present in whole-cell DTP vaccine may be correlated with a higher incidence of adverse events” (p. 181). The “significantly lower incidence rate” were those “of attributed deaths, convulsions, disabilities and life-threatening reactions (p <0:01) and of chronic brain damage (p <0:05)” (p. 181). The most statistically significant differences were found for sudden death, encephalopathy, and seizures.
Meanwhile, the Geier and Geier studies continue to be ignored in textbooks and reviews as if no such data existed.
Post-vaccinal encephalomyelitis rates in the UK
According to Bennito and Scolding, “Post-infectious and inflammatory encephalomyelitis are broadly represented by the syndrome acute disseminated encephalomyelitis (ADEM). ADEM forms one of several categories of primary inflammatory demyelinating disorders of the central nervous system” (p. i22). The report about the MMR stated:
Both the USA and UK have enough vaccine to cover their entire populations. Previously reported incidences of post-vaccinal encephalomyelitis following use of this vaccine are of the order of 10–300 cases for every one million vaccinations. A conservative projection would mean approximately 600 cases of ADEM if the UK were to vaccinate its entire population.
They also observed, “Presently, however, the non-neural 3 measles, mumps, and rubella vaccinations are commonly associated with post–vaccination encephalomyelitis. The incidence is 1–2 per million for live measles vaccinations” (p. 124).
1994–1996 Institute of Medicine (IOC) and CDC findings of vaccine adverse effects
The Institute of Medicine was an independent research organization chartered by the National Academy of Sciences (later to become a part of the NAS). In 1994, it did an analysis of all vaccines for their reported adverse events and attempted to rate each one’s potential to become an actual adverse effect [34]. The Institute’s data and conclusions were republished two years later in a CDC report [35].
In the category of “Evidence favored acceptance of a causal relationship,” the CDC report listed the following: “Thrombocytopenia, Anaphylaxis, and Death from measles-vaccine–strain viral infection” (Table 3, p. 30).
In the category of “Inadequate evidence to accept or reject a causal relationship,” the Institute of Medicine listed the following: “Encephalopathy, Subacute sclerosing panencephalitis, Residual seizure disorder, Sensorineural deafness, Optic neuritis, Transverse myelitis, Guillain-Barré syndrome, Thrombocytopenia, and Insulin-dependent diabetes mellitus” (Table 3, p. 4). This list of possible adverse effected should have created concerns and encouraged further research into these potential adverse effects.
In the category of “Evidence favored rejection of a causal relationship,” they found “none.” This clarified that they were not rejecting any of the adverse events labeled “Inadequate evidence to accept or reject a causal relationship” (Table 3, p. 30).
I can find no evidence that the CDC ever again published analyses of this kind from the Institute of Medicine or from any other authority or source. The Institute of Medicine would go on to publish only one more report in 2012 [36].
Institute of Medicine 2012 review of vaccine adverse effects
In 2012 the Institute of Medicine published a book titled Adverse Events Associated with Childhood Vaccines: Evidence Bearing on Causality. It contained detailed analyses and conclusions for possible adverse reactions to the various categories of vaccine. In each chapter on a specific vaccine it concluded with a chart that offered a “Causality Conclusion” for every potential adverse reaction for which it found sufficient data to examine. The categories were the same as used in their 1994 report and the republication by the CDC in 1996.
The data for the MMR vaccine is presented in Tables 4–13 in the Summary of Epidemiologic Assessments, Mechanistic Assessments, and Causality Conclusions for Measles, Mumps, and Rubella Vaccine (p. 218–222). The Institute “Convincingly Supports” its “Causality Conclusions” for the MMR for these three events: measles inclusion body encephalitis (in individuals with demonstrated immunodeficiencies), febrile seizures, and anaphylaxis. It “Favors Acceptance” for its Causality Conclusions for the following two events: transient arthralgia in children and transient arthralgia in women. This list of five confirmed MMR adverse effects already exceeds the listed adverse effects in all contemporary authoritative sources we have previously cited.
The Institute put most of the MMR adverse events in the category of Inadequate Evidence to Accept or Reject Causal Association, the category that can reasonably be considered a list of potential vaccine adverse vaccine effects requiring more research. It includes in this important category the following potential adverse events: encephalitis, encephalopathy, afebrile seizures, ataxia, acute disseminated encephalomyelitis, transverse myelitis, optic neuritis, neuromyelitis optica, multiple sclerosis onset in adults, multiple sclerosis onset in children, Guillain-Barre syndrome, chronic inflammatory disseminated polyneuropathy, opsoclonus myoclonus syndrome, brachial neuritis, chronic arthralgia in women, chronic arthritis in women, chronic arthropathy in children, arthropathy in men, hepatitis, chronic fatigue syndrome, fibromyalgia and hearing loss.
In the category Favors Rejection, the Institute put two events—autism and Type I diabetes.
The National Academies of Sciences, Engineering and Medicine issued a Press Release [37] well in advance of the 2012 book, with the falsely reassuring headline, Few Health Problems Are Caused By Vaccines, Iom [sic] Report Finds. The reader would never know that the institute had found strong evidence for five adverse events for the MMR by itself and more than 20 adverse events whose causative association remained to be determined.
Declining research and education concerning vaccine-induced neurological adverse effects
Only July 21, 2015, the Institute of Medicine became part of the National Academy of Medicine. Given the 2011 Press Release from the National Academies undermining the seriousness of the published data on vaccine harms from the old IOC in 2012, it is not surprising that further integration into the National Academies put an end to anything like the book Adverse Events Associated with Childhood Vaccines: Evidence Bearing on Causality. I have been unable to locate any further Institute of IOC or National Academy of Medicine publications providing this kind of thorough evaluation of potential vaccine adverse effects.
The field of research and education on vaccine harms continues to become increasingly suppressed. As an egregious example, throughout Adams and Victor’s Textbook of Neurology [24], nothing is reported about MMR and neurological harms—just that the MMR vaccine does not cause autism. There is nothing about any vaccines causing encephalopathy, encephalitis, or any other neurological disorder. The search, however, is hampered by the fact that, unlike the previous 10th edition (2014), the word “vaccine” has been deleted from the index!
The lead for Cochrane’s extensive promotional piece for their new review of MMR-V vaccines [38] begins with an announcement in bold [39] (p. 1):
New evidence published in the Cochrane
Library today finds MMR, MMRV and MMR+V
vaccines are effective and that they are not
associated with increased risk of autism.
Once again, we confront that avoidance of all adverse effects by merely repeating that the vaccines are “not associated with increased risk of autism”—leaving the mistaken impression that there are no risks at all.
News outlets, such as Medical News Today, got the message with its headline [40]: “Review says MMR vaccine is effective, does not cause autism”.
The absence of placebo controls in vaccine trials for FDA-approval
Although long-term data gathering studies involving surveillance and monitoring are required to study long-term adverse effects that are associated with vaccines, a surprising number of harms occur in the first few weeks. For example, encephalopathy is considered reportable by WHO [20] (p. 46) only if it occurs 6–12 days after measles/MMR vaccine and only 0-2 days after DPT vaccines. Geier and Geier, noted above, stated “that patients are at increased risk for developing serious neurologic disorders for about 5–10 days following pediatric MMR vaccination” (p. 207–208). When a treatment causes such short-term adverse effects, the ideal method of study is the placebo-controlled clinical trial.
The FDA requires controlled clinical trials for the approval of vaccines but remarkably it does not require placebo-controlled clinical trials as it does for most or all other drugs 4 . Instead, it allows the vaccine company to compare its potential new product to another already approved vaccine.
Encephalopathy is a very broad term meaning any disease of the brain, usually severe enough to cause physical and mental symptoms, and often secondary to some other event, such a poisoning or infection. Although severity is not a part of its formal definition, most investigators apply the diagnosis only to severe conditions. That encephalopathy is recognized as a possible or probable result of measles/MMR within a mere 6-12 days after vaccination suggests the possibility of much lesser manifestations of brain disease that might be much more common and easy to detect on shorter trials.
In the absence of urgent needs, such as a pandemic, it would be relatively easy to take the time and effort to conduct genuine placebo-controlled clinical trials by random selection from the normal populations to be vaccinated.
Since vaccine neurological injuries may be relatively rare, and some may not appear until months or years after vaccination, it would useful to conduct large, lengthy placebo-controlled clinical trials. Drug companies very rarely if ever do large, long-term placebo controlled clinical trials in part because it would potentially unethical to deprive sick patients of the experimental drug or of other drugs excluded from the trial protocol over a lengthy period. But there are no sick patients in most vaccine trials. The vast majority are normal children who might, like any other child, contract a disorder like measles, mumps, or rubella. Indeed, most of the children in vaccine studies would be protected by herd immunity among the other children who have already been vaccinated or who are being administered a new vaccine. The herd immunity would place them at very little or no risk from being deprived of a vaccine for a placebo-controlled clinical trial. Large, long-term placebo-controlled trials could be conducted with relative ease.
All existing and future potential vaccines need to be subjected to large, long-term placebo-controlled clinical trials. The extraordinary concession by the FDA not to require placebo controls for preapproval clinical trials for vaccines suggests compliance to extreme pressure from drug companies. It further suggests that the drug companies are worried about adverse effects that might show up, even in the kind of limited short-term placebo-controlled trials routinely and almost invariably required by the FDA.
Another approach—cohort event monitoring for at least the first consecutive 10,000 people—could provide useful information concerning immediate and delayed adverse effects, as well as effectiveness. The cohort can be kept for future reference as a cross-check with any spontaneous reports that show up as the exposure increases.
Well-designed placebo-controlled double-blind randomized clinical trials with sufficient power can demonstrate causation of an effect in that particular controlled context. Cohort-event monitoring can provide detailed clinical and other information to justify a possible causal interpretation in a wider context of clinical use, perhaps including a mechanistic reason for the effect in some cases. Conversely, controlled clinical trials cannot be used to exclude the possibility of rare adverse causal effects.
Conclusions
Vaccine defenders have used the vaccine/autism controversy strawman to dismiss all claims and any research concerning genuine neurological harms from vaccines. By leaving behind the vaccine/autism controversy, more focus can be given to genuine vaccine-induced neurological effects that can impair brain, mind, and behavior. Although it is currently difficult to determine their incidence, their existence requires greater attention. Since many of the worst potential adverse neurological effects, such as encephalopathy, occur shortly after vaccination, placebo-controlled clinical trials are a necessity and must be conducted for all existing and new vaccines, perhaps using cohort event monitoring as a backup where urgency for roll-out would be too delayed by a suitably large controlled study [41].
There is little or no evidence that vaccines or any other form of intrusion into the brain can cause the psychosocial, developmental clinical entity called autism or any similar syndrome or disorder. All or nearly all the identified victims of vaccination injury, as one would expect from a physical cause, have physical symptoms as a result of neurological harms. A broad range of neurological disorders including encephalopathy, encephalitis, dementia from any cause, anoxia, and traumatic brain injury (TBI) can cause disengagement from other people, difficulty focusing attention, or difficulty inhibiting anger; but these are symptoms of the neurological disorder and should not be misdiagnosed as autism, attention-deficit hyperactivity disorder (ADHD) or oppositional defiant disorder (ODD). Nor should these neurological effects be confused with even more vague or broad psychiatric diagnoses, such as neuropsychiatric disorder or anxiety disorder.
When a vaccine causes something that resembles a developmental or behavioral disorder, or probably any psychiatric disorder or psychiatric/psychological symptoms, the vaccine has almost certainly caused a distinct and potentially discernable underlying brain disorder, such as a minor neurocognitive disorder [27] or chronic brain impairment (CBI) [28]. Encephalitis, for example, can result in many psychological or psychiatric symptoms, which may show up during the acute phase of the disorder or years later [29]. Future research on vaccine injuries should focus on subtle injuries to the central nervous system rather than upon disorders typically classified as psychological, psychiatric, or developmental.
Footnotes
Conflict of interest
Dr. Breggin does forensic work, often on behalf of individuals harmed by medications.
1
Robert E. Weibel was from the Division of Vaccine Injury Compensation, National Vaccine Injury Compensation Program, Health Resources and Services Administration, Public Health Service, Rockville, Maryland, USA.
2
Diphtheria, tetanus and whole-cell pertussis vaccine.
3
Non-neural means not containing material from the nervous system of animals.
4
This author, who is most familiar with the FDA approval process for psychiatric drugs, is unaware of any psychiatric drug that has been approved without a placebo-controlled clinical trial.