
Abstract
BACKGROUND:
Off-label drug (OLD) use is common in neonates.
OBJECTIVE:
There is a dearth of information associating the OLD use and the risk of medication errors in critically ill neonates. Hence, the present study was carried out.
METHODS:
Drug prescriptions in neonates admitted to the intensive care unit of a tertiary care hospital between September 2018 and June 2019 were evaluated. Details on their demographics, reason for admission in intensive care unit, drug-related information and serum creatinine were extracted. United States Food and Drug Administration approved drug labels were compared. World Health Organization (WHO) anatomy, therapeutic and chemical (ATC) classification was used for drug categorization. We assessed the risk of medication errors in the adult population using a validated tool: medication risk score (MERIS).
RESULTS:
One hundred and seventy-one neonates with 2394 prescriptions were included in this study. Seventy one percent of the neonates in the present study received at least one OLD/unlicensed prescription item. A trend in increased numbers of OLD/unlicensed drug use in more premature and lower birth weight neonates were observed. Medication risk score was significantly higher in neonates receiving OLD/unlicensed drugs compared to those with only labelled drugs. Very and extreme pre-term (along with very low and extremely low birth weight) neonates were at higher risk of medication errors compared to others. Presence of OLD/unlicensed prescribed items is associated with a potentially increased risk of medication errors by an odds ratio of 20.4 compared to labelled drugs.
CONCLUSION:
Significant proportions of critically ill neonates received at least one OLD/unlicensed drug and such use was associated with potentially increased risk of medication errors.
Background
Off-label drug (OLD) use implies using a drug for indications/age/in dosages/formulations/route that was not approved by drug regulatory authorities [1,2]. OLD use is rampant in the specialties of neonatology, paediatrics, geriatrics, psychiatry, and oncology [3,4]. OLD use is not illegal provided it is evidence-based and the concerned patients/legal representatives were informed and consented [5,6]. Drug regulatory authorities do not regulate drug prescription [7]. In children the available appropriate labelling for children is lagging adults and so off-label use in children is inevitable [8]. Children differ considerably in their maturation/development of organ systems that is particularly striking in the first few weeks of life [9]. Due to the challenges involved in conducting clinical trials in this population, pharmaceutical companies hardly engage in generating evidence for labelled drug use [10]. Use of off-label/unlicensed drugs were reported to prevail in over 65% of children and over 90% in the neonatal population [11,12]. Recently, Best Pharmaceuticals for Children Act and the Paediatric Research Equity Act resulted in changes in around 500 drug-related labels benefiting patients [13]. OLD use is associated with greater risk of harms and has been considered as a “Public health issue” for infants, children, and adolescents [14,15]. Pharmaceutical Companies have been blamed and lawsuits were filed for promoting OLD use [16]. Though previous studies have evaluated the prevalence of OLD use in neonatal population, there is a dearth of data in attributing the risks of medication errors with OLD. Only one study observed that nearly 70% of the neonates were administered a harmful drug [17]. Recently, medication risk score (MERIS) tool was developed and validated to assess the same in adult population [18]. The present study was carried out to evaluate the prevalence of OLD/unlicensed drug use in the neonatal population and the associated risk of medication errors in various groups of the neonatal population.
Methods
Study ethics and procedure
We carried out a prospective observational study in neonatal intensive care unit (NICU) of a tertiary care hospital between September 2018 and June 2019 after obtaining approval from the Institutional Ethics Committee. Following the consent from one of the parents of the admitted neonates, we extracted the following details: demographic details (gestational age, gender and birth weight), reason for admission in NICU, serum creatinine and drug-related information (name, dose, route, frequency and duration). We excluded those neonates that did not receive any drug during their NICU stay as well as neonates who were re-admitted. Shull equation was used for deriving the estimated glomerular filtration rate (eGFR) [19]. We considered administration of all drugs except for intravenous fluids, any blood products, oxygen therapy and parenteral lipids/nutrition. Drug labels were obtained from United States Food and Drug Administration (USFDA) (https://nctr-crs.fda.gov/fdalabel/ui/search). The drug regulatory authority of the Kingdom of Bahrain, according to Decree No. 8 of the 2017 regulations for the registration of medicines, allows registration of medical products that are registered at any of the following drug regulatory authorities for a minimum of one year period: USFDA, Health Canada, European Drug Authority or one of the European countries accredited to the Commission, SWISSMEDIC – Swiss medicine, and Australian Drug Administration [20]. Use of drugs in the study population was considered off-label if the drug label indicated that the drug was not approved for use in neonatal population. In case of non-retrieval of labels, it was considered to have not been licensed by USFDA. World Health Organization (WHO) anatomy, therapeutic and chemical (ATC) classification was used for categorizing the drugs [21]. We assessed the risk of medication errors using a validated tool, mediation risk score (MERIS), that evaluates the risk under the following categories: number of drugs; eGFR score; and risk of harm/interaction score [18]. The drugs used in our study population were classified into low, medium, and high risk of harm/interaction based on the earlier validation in the adult population [18] and by a consensus amongst the in-house neonatologist. The classification list is provided in Table 1.
Classification of risk of harms and interactions of the drugs used in the study population
Classification of risk of harms and interactions of the drugs used in the study population
Demographic characteristics were represented using descriptive statistics. Numerical variables across the groups were tested using either Mann-Whitney U or Kruskal-Wallis H test following assessment of normal distribution of the variables. Trend analysis was assessed using the Jonchkheere-Terpstra test. Categorical variables were analysed using Chi-square test for association and trend using Cochran-Armitage Chi-square for trend analysis. MERIS score above 13 was considered as an increased risk for medication errors as suggested in the previous study [18]. Binary logistic regression was used to assess the risk of medication errors using presence of at least one OLD/unlicensed drug. A p-value of ≤0.05 was considered significant. SPSS version 25.0 for Windows (IBM Corp., Armonk, NY, USA) was used for statistical analysis.
Based on the gestational age, the neonates were classified as term (≥37 weeks), late pre-term (>32–36 weeks 6 days), early pre-term (>28–32 weeks) and extremely pre-term (<28 weeks). Similarly, based on their birth weights, the neonates were classified into following categories: normal birth weight (≥2500 g), low (1500–2499 g), very low (1000–1499 g), and extremely low birth weight (<1000 g) [22].
Results
Demographic details
One-hundred and seventy-one neonates were enrolled in this study. Their baseline characteristics are summarized in Table 2. The majority of the neonates belonged to late pre-term and low birth weight categories and 90.6% of the neonates were discharged alive from NICU.
Demographic characteristics of the study participants (N = 171)
Demographic characteristics of the study participants (N = 171)
$-Represented in mean (SD); @-Mentioned in median (range); NICU-Neonatal intensive care unit; IUGR-Intra-uterine growth restriction.
Two thousand three hundred and ninety-four prescriptions with 25943 items were provided to the study participants. Median (range) of number of drugs prescribed to the study participants was 8 (44). The numbers of drugs administered to the study population belonging to each of WHO ATC classes are as follows: systemic anti-infectives (n = 546); alimentary tract and metabolism (n = 515); cardiovascular system (n = 378); nervous system (n = 316); blood and blood forming agents (n = 129); sensory organ system (n = 84); and dermatological preparations (n = 75). Table 3 lists the number of drugs administered to the study participants classified based on their gestational age and birth weight categories. The majority of the prescribed drugs were anti-infective drugs for systemic use followed by alimentary tract and metabolism group as per WHO ATC classification (Table 4). Significant (p < 0.05) differences were observed in the proportions of drug classes administered to various gestational age groups of the neonates (term and pre-term neonates received significantly more number of systemic anti-infective drugs; term neonates received significantly more drugs belonging to the cardiovascular system; very and extremely pre-term neonates received significantly more drugs pertaining to the respiratory system; and term neonates received more dermatological drugs). Fifty-two prescribed items were not listed by WHO for the indications as administered to the study participants of which 51 received magnesium sulphate and one received sildenafil.
Comparison of number of drugs and prescription items in all age and birth weight categories
Comparison of number of drugs and prescription items in all age and birth weight categories
WHO ATC classification of prescription items in the study population
ATM-Alimentary tract and metabolism; AI-Anti-infective drugs for systemic use; CVS-Cardiovascular system; D-Dermatological preparation; NS-Nervous system; RS-Respiratory system; S-Sensory organ system; B-Blood and blood forming agents; ∗-Statistically significant (p ≤ 0.05).
One-hundred and twenty-one [70.8%, 95% CI: 64.0–77.6%] neonates received at least one off-label or unlicensed drug. Mean (SD) number of off-label or unlicensed drugs was 6.3 (6.7) and the total number of OLDU in the study population was 548. The distributions of labelled, off-label and unlicensed drug categories according to body weight and gestational age categories are depicted in Fig. 1. Significantly more neonates in the categories of either extreme pre-term or very low birth weight received higher numbers of off-label or unlicensed drugs (Fig. 2). The majority of the drugs were not approved in the paediatric age group (292/548, 53.3%); and 12% (66/548) were not approved in children less than 6 months of age (Table 5). Comparison of OLD use with labelled drugs as per WHO ATC groups is depicted in Fig. 3. More OLD/unlicensed drug were observed in the categories of dermatology [70/75 (93.3%)] according to gestational age categories; and 71/75 (94.7%) according to birth weight categories (Fig. 3). Seventeen (0.7%) prescriptions had drugs that were contra-indicated; 15 were hydrocortisone and two had aminoplasmin.
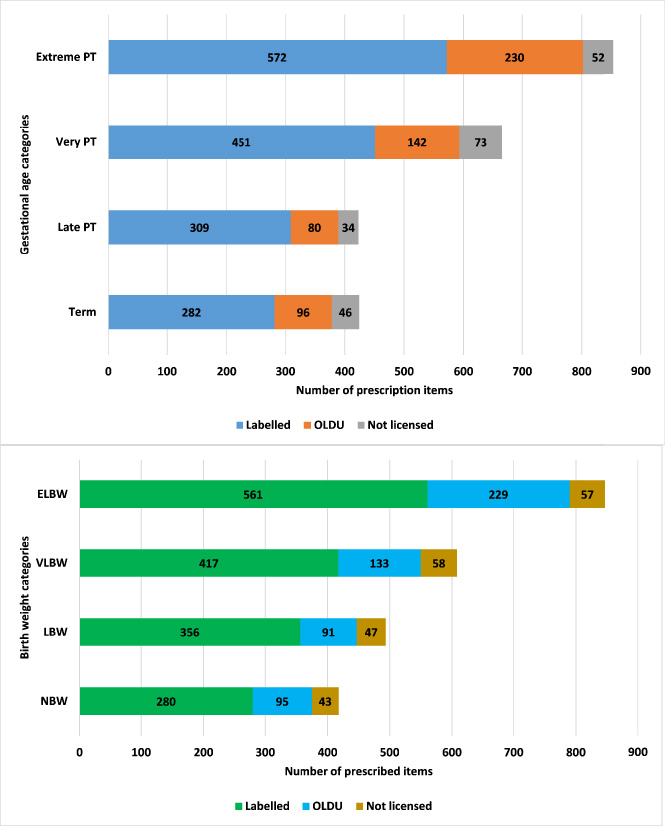
Proportion of labelled, off-label and unlicensed drugs in various sub-categories according to gestational age and birth weight in the study population. PT-Preterm; OLDU-Off-label drug use; NBW-Normal birth weight; LBW-Low birth weight; VLBW-Very low birth weight; ELBW-Extremely low birth weight.

Comparison of numbers of off-label or unlicensed drugs used in patients with different gestational age or birth weight categories. Statistically significant (= 0.0001) differences were observed in the numbers of either off-label or unlicensed drugs used in various categories of gestational age and birth weight. OLD-Off-label drug; PT-Preterm; NBW-Normal birth weight; LBW-Low birth weight; VLBW-Very low birth weight; ELBW-Extremely low birth weight.
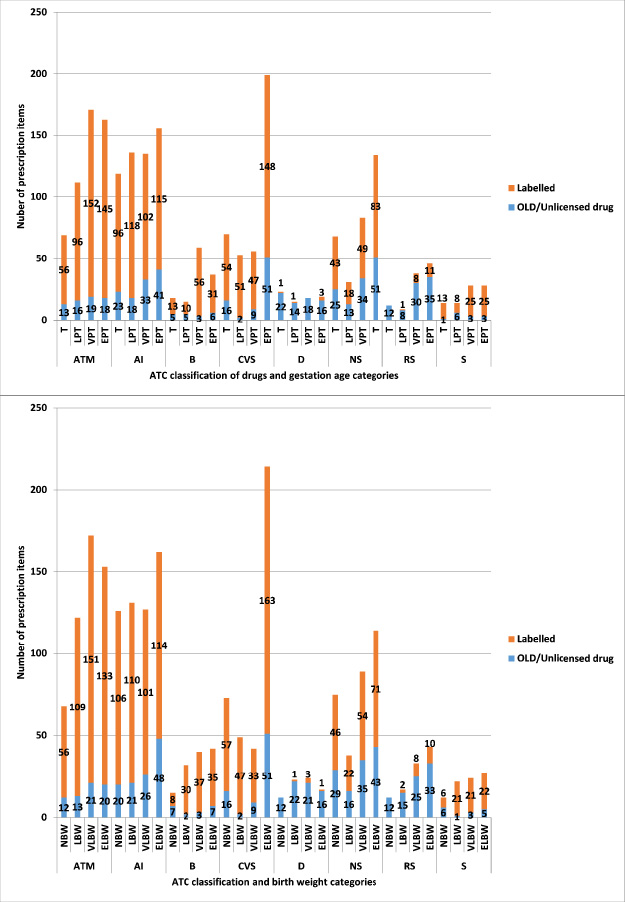
Comparison of use of OLD/unlicensed drug with labelled drugs in various WHO ATC groups. ATM-Alimentary tract and metabolism; AI-Anti-infective drugs for systemic use; CVS-Cardiovascular system; D-Dermatological preparation; NS-Nervous system; S-Sensory organ system; B-Blood and blood forming agents; OLD-Off-label drug; T-term; LPT-Late pre-term; VPT-Very pre-term; EPT-Extreme pre-term; NBW-Normal birth weight; LBW-Low birth weight; VLBW-Very low birth weight; ELBW-Extremely low birth weight.
Classification of OLDU (as per defined age-limits from US FDA approved SPC) amongst the prescription items in the study population
OLDU-Off-label drug use.
Mean (SD) of serum creatinine amongst the study population was 64.7 (16.8) μmol∕L and the corresponding eGFR was 35.1 (12.8) ml∕min∕1.73 m2. All components for assessing the MERIS score were available for 148 participants. The MERIS evaluation revealed average (SD) scores for the number of drugs, eGFR and harm/interaction of 15.6 (4.8), 17.2 (3) and 11.2 (2.7) respectively with a final score of 41 (7.7). Assessment of the total and individual components of MERIS according to the gestational age and birth weight categories are depicted in Fig. 4. Significantly higher scores for all the sub-components as well as for the total MERIS was observed for younger neonates as well as lower birth weights. Out of the 148 neonates evaluated for MERIS, 45 received only labelled drugs while the remaining at least one OLD/unlicensed drug. Significantly (p = 0.01) higher scores except in eGFR category were observed for neonates receiving at least one of either off-label drug or unlicensed drug compared to those receiving only labelled drugs (Fig. 5). Out of 103 neonates with at least one OLD/unlicensed drug use, 84 (81.6%) had higher risks of medication error as per MERIS compared to only 8/45 (17.8%) with labelled drugs; and this was statistically significant (p < 0.0001). Similarly, higher proportions of very pre-term and extreme pre-term neonates (also very low and extremely low birth weight) neonates had significantly (p = 0.0001) more risk of medication errors (with MERIS score >13) compared to term and late pre-term neonates (Fig. 6). Binary logistic regression analysis revealed a trend between the use of OLD/unlicensed drugs and the risk of medication errors compared to use of only labelled drugs [OR:20.4, 95%CI: 8.2, 50.9; p = 0.0001].
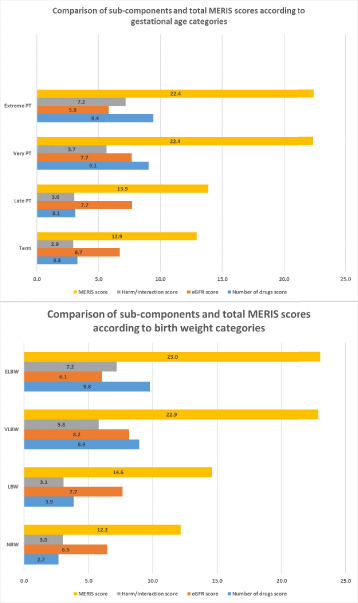
Medicine risk score (MERIS) in each sub category of the study population. Statistically significant (= 0.0001) differences were observed in all scores between various categories of gestational age and birth weight. PT-Pre-term; NBW-Normal birth weight; LBW-Low birth weight; VLBW-Very low birth weight; ELBW-Extremely low birth weight.
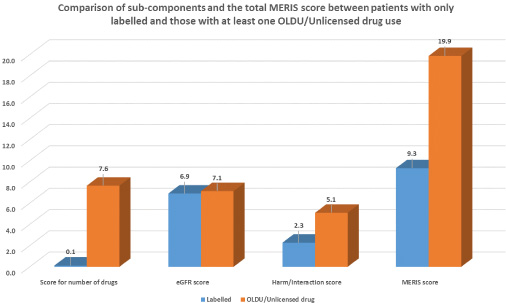
Comparisons of the individual components and total medication risk score (MERIS) between neonates with at least one off-label drug compared to those with only labelled drugs. Significant differences (p < 0.05) were observed in all scores except for the eGFR score between neonates receiving only labelled compared to those with at least one of the OLDU or unlicensed drugs. OLDU-Off-label drug use; MERIS-Medication risk score.
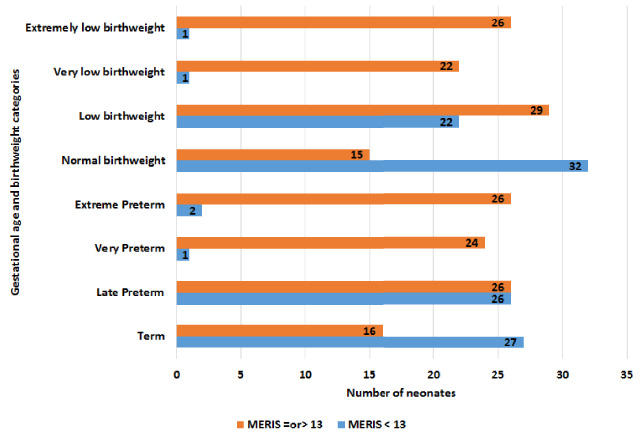
Comparison of risk of medication errors in various gestational age groups and birth weight categories. Significant proportions (p < 0.05) of very and extremely, and very low and extremely low birthweight neonates had medication risk scores (MERIS) ≥13 compared to other groups.
The American Academy of Pediatrics in its policy statement has stated that “off-label drug use does not constitute improper, illegal, contraindicated or investigational use” [13]. USFDA approves a drug and drug label based on substantial evidence based on adequate and well-controlled evidence [23]. In children, OLD use has been observed to triple the risk of adverse drug reactions [24]. We observed that majority of the OLD/unlicensed drug use were drugs belonging to dermatology and nervous system categories according to WHO ATC classification. This is similar like studies from European and Australian intensive care units [25–27]. However, drugs in the category of alimentary tract and metabolism was reported with the highest frequency of being used off-label from USA; and anti-infective drugs from developing countries [4,28]. Pharmaceutical companies have stepped forward in conducting more paediatric studies as evident by the increased clinical trial reports, but it is certainly a long way to go in neonates [29]. Several regulations such as European Union Pediatric regulation have hardly made any significant impact in the prevalence of OLD use in children [30].
Differences in the drug regulatory agencies in drug approvals and consequent label information were also observed in previous studies [31]. American Academy of Paediatrics insists on obtaining consent from the parents if a drug is used either in an off-label manner or if it is unlicensed [32]. Partly, onus lies with the practising physicians in publishing their experience with such drugs that adds to the scientific literature and may aid in therapeutic decision-making. Pediatric advocacy groups must continue insisting label changes in neonatal population.
Medication errors have been reported to occur at an incidence between 5–13% in NICU [33–35]. The Institute for Safe Medication Practice has classified 10 drugs/drug classes as high alert medications as they are highly susceptible to dosing errors with serious consequences [36]. Using the MERIS tool, we observed that nearly 61.5% of neonates in the present study had potential risk of medication errors. Using the MERIS tool, we observed that the odds of medication error risk may be 20.4 times higher than using only labelled drugs.
While applying the MERIS tool in the neonatal population, we observed a limitation that one of the components, eGFR score, was not discriminatory between the sub-populations and did not contribute significantly to the total scores. In the present study, eGFR was based on serum creatinine. We used the Shull’s equation in the present study for evaluating eGFR as we did not have length measurements of the neonates. Assessing the eGFR with one of the equations containing length of the neonates may improve the utility of this item in the scoring tool. Several novel biomarkers such as cystatin C can accurately predict the glomerular perfusion rate in neonates, it is often not practically feasible in developing countries to inculcate this as the standard of care and hence serum creatinine based equations are adhere to as in the present study. However, neonatal specific eGFR based on a validated biomarker would add more value in developing such scoring systems. Alternately, number of drugs with potential renal toxicity may be considered instead of eGFR score. Although MERIS has been developed and validated in adult population, we do not have any validated paediatric/neonate specific medication error tool. Apart from this, the study is also limited in not exploring the level of scientific evidence for OLD use and the mentions in drug compendia such as Micromedex or British National Formulary; and no validated scoring system was used to assess the severity of illnesses. Also, the classification list of drugs for assessing the MERIS tool based on their potential to cause harms/interaction was validated by four neonatologist and one clinical pharmacologist. Amongst the neonatologist, the experience in the field ranged between 10–26 years and the clinical pharmacologist had 12 years of experience. It is preferable to validate the tool with large network of potentially diverse population involved in neonatal care. In the original article related to the MERIS tool, during the initial phase of model development, co-morbidity was considered as one of the elements that was subsequently left. Future studies validating such a tool in the neonatal population should consider co-morbid diseases as an element.
Conclusion
In conclusion, significant proportions of critically ill neonates received either off-label or unlicensed drug and consequently were associated with a potential risk of medication errors. However, it must be noted that we did not actually measure the medication errors but the potential risk. We observed that the eGFR component based on serum creatinine of the MERIS score that was adapted in the presents study, does not discriminate between those with the risk of medication errors and those without. We recommend validating a modified MERIS tool using alternate measuring method for eGFR based on novel biomarkers or using scoring systems that include length as one of the variables as stated above. This is critical in neonates considering the rapid maturation of nephrons during the post-natal period. Developing neonate-specific tool for assessing the risk of medication errors may aid in better understanding the characteristics of neonates and drugs/drug classes that are more prone for medication errors. The results of this study should be considered as preliminary evidence in identifying that there is a potential risk of medication errors particularly with OLDU in neonates.
Footnotes
Author contributions
KS conceived the idea; KS, MA and EA carried out the study and collected data; KS performed data analysis and wrote the first draft of the manuscript; KS, MA and EA were involved in the manuscript revision, and all authors accepted the final version. The authors had complete access to the data supporting the publication.
Conflict of interest
The authors do not have any conflict of interest.