
Abstract
BACKGROUND:
Inappropriate repeat testing is an objectively measurable type of health service overutilization which may harm patients.
OBJECTIVE:
To evaluate both the frequency and cost of inappropriate repeat testing in a tertiary hospital in terms of specialties.
METHODS:
This cross-sectional study was conducted in a tertiary hospital. Laboratory results of 26 tests ordered between 1 July 2014 and 30 June 2017 were evaluated retrospectively. Test that were repeated earlier than the minimum re-test interval were accepted as inappropriate repeat testing. After analyzing the descriptive statistics, the cluster analysis method was used to determine whether groups were formed within specialties.
RESULTS:
Specialties form two clusters were found: the first cluster included specialties mostly from surgical science and the second cluster included specialties mostly from medical science. It was found that the cluster that includes mostly surgical specialties repeats laboratory tests at a higher rate but causes a waste of less resources, whereas the cluster that includes mostly medical specialties repeats laboratory tests at a lower rate but causes a waste of more resources due to a higher volume of test orders.
CONCLUSION:
Due to the high rates of inappropriate repeat testing, surgical specialties seem to be the first target of intervention strategies, but medical specialties, which account for a higher volume of inappropriate repeat testing and higher unnecessary cost, should be the primary target of intervention strategies.
Keywords
Introduction
Laboratory tests are an essential part of healthcare delivery and provide a basis for clinical decision-making [1]. The increase in the use of laboratory tests, which almost doubles every five years since 1963, surpasses even the largest confounding factors, i.e. the increase in both the population and the proportion of elderly population [2]. There are significant regional and physician-based differences in the use of laboratory tests worldwide, which suggests that at least some of these tests are inappropriate [3]. For example, one study found a 89-fold difference in requests of brain-type natriuretic peptide (BNP) among family physicians in the UK [4]. False-positive abnormal results in healthy normal individuals, either from the methods of the study to determine reference ranges of laboratory tests or from inter-laboratory differences, triggered the subsequent tests, interventions and treatment protocols, leading to increased morbidity, delayed diagnosis, and iatrogenic anemia [5,6]. Inappropriate laboratory repeat testing also causes waste of resources besides the patient safety issues. For example, in the UK, the cost of inappropriate laboratory tests was £1 billion [7], while in the US it was estimated at $8.2 billion [8] in 2004. These figures are direct costs and do not include any other costs that may arise due to wrong decisions made as a result of an inappropriate repetition of tests.
Although it is known that family physicians are responsible for more than half of the laboratory test costs when evaluated in the general population [3], to the best of our knowledge, no studies in the literature have evaluated inappropriate repeat testing in terms of specialties. In this study, objective measures are used to determine inappropriate repeat testing so that it is easier to implement interventions and evaluate the success of interventions. Because measures are independent and are not influenced by the judgment of researchers, studies about inappropriate repeat testing can be easily repeated and compared to others worldwide. The aim of this study was to evaluate both frequency and cost of inappropriate test repetition in a tertiary hospital in terms of specialties.
Materials and methods
Study design
This cross-sectional study was carried out on tests that were recorded in the laboratory results database between 1 July 2014 and 30 June 2017 at the Canakkale Onsekiz Mart (COMU) University Hospital. This hospital consists of 280 physicians and 677 beds and is the only tertiary hospital in Canakkale province, which has 519,793 inhabitants.
To determine inappropriate repeat testing, the time of the result was included for each test and compared with the time of the result from the previous test. If the time interval between the two tests was shorter than the minimum test interval, the second test was accepted as an inappropriate repeat test. Minimum re-test intervals were mostly obtained from the report of the National Minimum Re-testing Intervals in Pathology composed by The Royal College of Pathologists, The Association for Clinical Biochemistry and Laboratory Medicine and The Institute of Biomedical Science [9]. In addition, a literature search was performed to determine the minimum re-test intervals of tests which were not included in this report: Erythrocyte sedimentation rate [10], antinuclear antibody [11] and vitamin B12 [12]. If the minimum re-test interval was presented as a time interval (i.e. 4–8 weeks), the lowest value was accepted as the minimum re-test interval. In general, in the literature, the shortest duration between the first and second tests will be accepted as minimum re-test interval if performing the second test makes clinical sense. Hence, the following question arises: “How can we decide whether the test makes clinical sense or not?” There are an excessive number of parameters that may affect the clinical importance of the test, such as half-life of the biomarkers, cost effectiveness, effects on clinical decisions of physician and/or contribution to patient prognosis [9]. It should also be noted that more than half of the minimum re-test intervals in the literature are based on the opinions of experts, but still the minimum re-test interval is the most objective measure for overutilization of laboratory tests.
Specifying criteria for inappropriately repeated laboratory tests
Specifying criteria for inappropriately repeated laboratory tests
ANA: Antinuclear antibody, ANCA: Antineutrophil cytoplasmic antibodies, ALT: Alanine aminotransferase, ASO: Anti-streptolysin O, AST: Aspartate aminotransferase, CA15.3: Cancer antigen 15-3, CA19.9: Cancer antigen 19-9, CA125: Cancer antigen 125, CRP: C-reactive protein, ESR: Erythrocyte sedimentation rate, GGT: Gamma-glutamyl transferase, HDL-C: High-density lipoprotein cholesterol, LDL-C: Low-density lipoprotein cholesterol, tPSA: Total prostate specific antigen, TSH: Thyroid-stimulating hormone.
Minimum intervals for each kind of laboratory tests are listed in Table 1, with exceptions that exclude the test from evaluation. To exclude acute poisoning, acute liver injury and preeclampsia, which make the minimum re-test interval obscure for aspartate aminotransferase (AST) and alanine aminotransferase (ALT), patients with F10.0 – F19.0, T36 – T65, W57, X20 – X29, X44 – X49, X89, X90, Y10 – Y19, A05, K71, K72, P93, Z03.6, Z57.4, Z57.5, O26.6, S36.1, T86.4, Z94.4, O14, O15, B15 – B17 diagnosis codes according to the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD 10) [13] were excluded from the study. To exclude hypertriglyceridemia, which makes the minimum re-test interval obscure for total cholesterol, high-density lipoprotein cholesterol (HDL-C) and low-density lipoprotein cholesterol (LDL-C) and patients with the E78.1 diagnosis code according to ICD 10 [13] were excluded from the study. To exclude chronic kidney disease, which makes the minimum re-test interval obscure for ferritin and patients with the N18 diagnosis code according to ICD 10 [13] were excluded out of the study. In total 784,394 test results were obtained, but 62,337 (7.9%) were excluded due to exceptions specified in Table 1, and 48,263 (6.2%) were excluded due to missing records.
Hierarchical cluster analysis is a subtype of cluster analysis. In this analysis, clusters take shape step by step instead of determining all clusters in one step. At the beginning of agglomerative hierarchical cluster analysis, every subject represents their different clusters. These clusters then conjoin according to their similarities (or dissimilarities) until they form a single cluster that includes all subjects [14]. This analysis has several different types of algorithms, one of which is the centroid clustering method, which involves merging clusters with the most similar mean vectors [14]. This method is preferred when the cluster sizes are not equal [15]. In fact, there are too many clustering algorithms and none can be accepted as best. So, it is allowed to run different algorithms or methods of clustering on the same data to find out which describe the data best when there is no aim to prove (or disprove) a hypothesis [16].
After analyzing the descriptive statistics, the agglomerative hierarchical cluster analysis was conducted to determine whether the specialties cluster in the context of inappropriate repeat testing. The centroid clustering method was used for cluster analysis. Due to the continuous nature of the variables, Pearson correlation was used as the dissimilarity measure [14]. The final number of groups were decided according to a dendrogram [15]. For cluster analysis, two variables were used: inappropriate test repetition rate within a specialty and unnecessary cost ratio of a specialty within the total. Variables were transformed into a z score before cluster analysis to standardize the variables [14].
In the cost analysis, the quantity of each test was multiplied by the amount of money that was paid for each test to the hospital by the governmental reimbursement institution of Turkey [17]. Although the costs mentioned were for inpatients, only the formal values were available. The exchange rate of the Turkish Central Bank on 4 January 2016 was used to convert Turkish Lira (TRY) to USD.
In this study, Pediatric and Adolescent Mental Health and Diseases, Pediatric Surgery, Medical Genetics, Nuclear Medicine, Radiology, Underwater and Hyperbaric Medicine, Medical Microbiology and Health Board were combined under the subgroup of Other Specialties, because of the ratio of the requested tests to the total tests was below 0.1%.
Means and standard deviations were given in a format of mean (SD). All analyses were performed by IBM SPSS Statistics for Windows, version 20.0 (IBM Corp., Armonk, NY, USA) software.
Ethics
Ethical approval was obtained from the Committee of COMU Clinical Research Ethics under number E.33585. Written permission was obtained from the Chief Executive of COMU University Hospital for accessing the laboratory database to obtain test results.
Results
In total, 673,794 test results of 77,450 patients were evaluated. The mean age of the patients was 44.5 (22.3) and ranged from 0 to 103. Of all patients, 33,692 (43.5%) were male and 43,758 (56.5%) were female. A mean of 8.7 (13.8) tests were performed per patient. Of the tests, 290,888 (43.2%) were performed for men and 382,906 (56.8%) for women. The highest number of tests was ordered by Internal Medicine with 253,169 (37.6%) tests and the lowest was 424 (0.1%) by Plastic and Reconstructive Surgery.
Of the total of 673,794 tests, 109,370 (16.2%) were inappropriate repeat tests. The most inappropriate repeat testing was ordered by Internal Medicine (47,873 test), whereas the highest percentage of inappropriate repeat testing was ordered by Thoracic Surgery (50.2%). The least inappropriate test repetition was ordered by Plastic and Reconstructive Surgery (50 tests), whereas the lowest percentage of inappropriate repeat testing was ordered by Physical Therapy and Rehabilitation (3.9%). The total number of test requests, the number of inappropriate repeat tests and the ratio of inappropriate repeat testing according to specialties are described in Table 2.
Number of test requests, inappropriate repeat testing and unnecessary cost according to specialties
Number of test requests, inappropriate repeat testing and unnecessary cost according to specialties
Other specialties: Health Board + Medical Microbiology + Medical Genetics + Nuclear Medicine + Pediatric and Adolescent Mental Health and Diseases + Pediatric Surgery + Radiology + Underwater and Hyperbaric Medicine.
During the three year period that was evaluated in this study, it was determined that $66,761.3 was wasted on inappropriate repeat testing. Internal Medicine caused both the highest volume and highest percentage ($29,007,5–43,40%) of unnecessary cost while Plastic and Reconstructive Surgery caused both the lowest volume and lowest percentage ($18,9–0,03%) of unnecessary cost. Unnecessary cost caused by all specialties is given in Table 2.
As a result of cluster analysis, Emergency Medicine, Family Medicine, Internal Medicine, Other Departments, Dermatology, Physical Therapy and Rehabilitation, Ophthalmology, Gynecology and Obstetrics, Cardiology, Neurology, Otorhinolaryngology, Pediatrics, Plastic and Reconstructive Surgery, Psychiatry, and Urology constituted a cluster (mean inappropriate test repeat rate: 10.7%, mean unnecessary cost ratio: 5.6%) while Anesthesiology and Reanimation, Neurosurgery, General Surgery, Thoracic Surgery, Infectious Diseases, Pulmonary Diseases, Cardiovascular Surgery, Transplantation Unit and Orthopedics and Traumatology constituted another cluster (mean inappropriate test repeat rate: 35.3%, mean unnecessary cost ratio: 1.7%). The dendrogram of the cluster analysis is given in Fig. 1 and the clusters are summarized in Table 3.
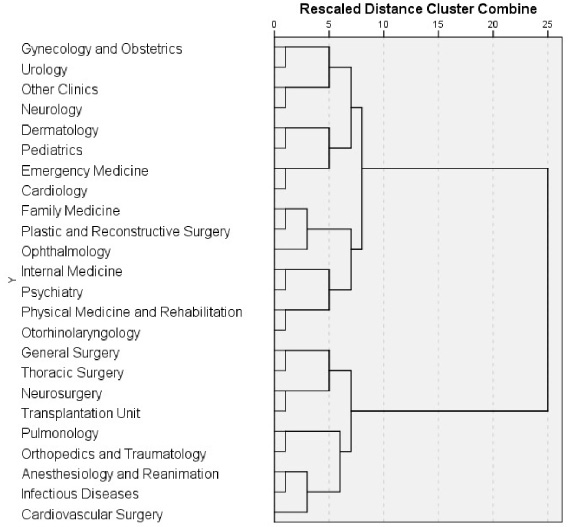
Dendrogram of cluster analysis (how the specialties were clustered by the variables of the inappropriate repeat testing rate within specialty and the unnecessary cost rate within total).
Clusters of specialties in terms of inappropriate repeat testing (within specialty) and unnecessary cost expenditure (within total)
*: Specialties from surgical science.
In our study, the frequency of unnecessary test repetition was found to be 16.2%. This rate is even more than double than that of 7.4% found in a recent meta-analysis [18]. However, the rate of inappropriate repeat testing is nearly the same as the one determined in a Canadian study (16.4%) which was conducted with a similar methodology for just six common laboratory tests [5].
In the three year period that was evaluated, a total of $66,761.3 was spent unnecessarily on inappropriate repeat testing. When the population served by COMU University Hospital is compared to the whole country, it can be estimated that in this three year period, more than $10 million was wasted on inappropriate repeat testing alone at tertiary hospitals countrywide. It should be noted that these costs were only direct costs. If the cost of sequential procedures that follow inappropriate repeat testing is calculated, the cost may reach much higher amounts.
Specialties with the highest ratio of inappropriate repeat testing were Thoracic Surgery (50.0%), Transplantation Unit (44.2%) and Anesthesiology and Reanimation (41.7%), while Internal Medicine (47,873), Cardiology (10,194) and Neurology (10,156) respectively accounted for the highest volume of inappropriate repeat testing. It was seen that specialties with the highest ratio of inappropriate repeat testing were from surgical science whereas specialties with the highest volume of inappropriate repeat testing were from clinical medical science. In one study, it was found that some of the pre-operative tests may cause inappropriate repeat testing, although the definition of unnecessary test repetition is different from our study [19]. It was determined that Internal Medicine (43.4%), Neurology (8.8%) and Cardiology (7.3%) accounted for the highest unnecessary cost, respectively.
Cluster analysis shows that the cluster with a lower frequency of inappropriate repeat testing and a higher amount of unnecessary cost was composed mostly by specialties from clinical medical science, whereas the other cluster with a higher frequency of inappropriate repeat testing and a lower amount of unnecessary cost was composed mostly by specialties from surgical science. Due to the high rates of inappropriate repeat testing, specialties from surgical science seem to be the first target of intervention strategies, but specialties from clinical medicine science, which account for higher volume of inappropriate repeat testing and higher unnecessary cost, should be the primary target of intervention strategies.
Since our study was conducted in a tertiary hospital, the primary care level was not sufficiently evaluated, but considering that primary care physicians were responsible for almost 55% of the laboratory test requests, it is very unlikely to be successful in laboratory intervention strategies without including primary care [20]. Investigating unique situations and dynamics on laboratory test uses of specialties will be beneficial in establishing more effective health policies and providing safer health care services.
Footnotes
Conflict of interest
None declared.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.