
Abstract
BACKGROUND:
Neurosensory impairment is a common complication following inferior alveolar nerve (IAN) damage.
OBJECTIVE:
To document and report the various causes, diagnosis, and management of IAN damage secondary to orthodontic treatment.
METHODS:
An electronic search for studies that reported IAN damage in patients undergoing orthodontic treatment was performed up to July 15, 2020 using MEDLINE, Embase, and PubMed databases. Descriptive analyses and linear regression model were performed.
RESULTS:
A total of 15 case reports were identified including 16 patients with an overall mean age of 23.3. All the included studies reported temporary sensory alterations which manifested as anesthesia (19%, n = 3), paresthesia (75%, n = 12), or combined (6%, n = 1). The majority of cases managed by stopping the orthodontic force (75%, n = 12), followed by appliance adjustments (19%, n = 3), providing a bite plate (13%, n = 2), and/or providing pharmacological management (38%, n = 6). Full recovery median duration reported in all cases following the aforementioned managements was 17.5 days.
CONCLUSIONS:
IAN damage secondary to orthodontic treatment is emerging in the literature in recent years. Identifying high risk patients with close proximity to the IAN canal is a must to formulate a proper treatment plan to avoid such complications.
Introduction
Inferior alveolar nerve (IAN) damage has been extensively reported in the literature on a wide range of dental and surgical procedures, which can be broken down into local or systemic factors. Systemic factors that may cause nerve damage or altered sensation include multiple sclerosis, metastases, bacterial infection, viral infection, sarcoidosis, drug and blood induced diseases [1]. While local factors mediate neural damage through mechanical, chemical or thermal stimuli [2]. The local factor with the highest incidence of IAN damage is orthognathic surgery with a frequency of up to 83% in the first week and 18.4% at one year [3]. Moreover, third molar surgeries are a more common cause of IAN damage as there is a reported prevalence of 1.5% at 1 month and 0.6% at 1 year postoperatively [4]. Trauma, local tumors, endodontic surgery, and pre-prosthetic surgery may also induce IAN damage [5].
Damage of the IAN manifests differently amongst affected patients including altered sensation associated with the ipsilateral lower lip, chin, buccal mandibular gingivae, and teeth. These altered sensations include paresthesia, anesthesia, dysesthesia, hyperalgesia, allodynia, hypoesthesia, or hyperesthesia as classified by The International Association for the Study of Pain (IASP) [6]. These reported altered sensations could either be temporary or permanent depending on the performed procedure and its pertaining risks. However, it has been shown that about 90% of the IAN damages are temporary and resolve within eight weeks but should be considered as permanent if the damage persists more than six months [7]. Although cases of IAN damage have been widely reported in oral and maxillofacial surgical procedures, the aim of this review was to explore IAN damage related to nonsurgical orthodontics, which is a much rarer cause. There has been an increase in the number of case reports on temporary paresthesia following orthodontic procedures in recent years. This scoping review was conducted to document and report in depth, the various causes, diagnosis and management of IAN damage secondary to orthodontic treatment.
Materials and methods
Search protocol and study selection
An electronic search using MEDLINE via Ovid, Embase via Ovid, and PubMed databases was performed up to July 15, 2020 independently by two authors using the following search strategy: ((Orthodontic* OR Braces) AND (Inferior Alveolar Nerve OR Inferior Dental Nerve OR IAN) AND (Injur∗ OR Damage∗)). Additional records were also identified manually through searching the reference lists of the relevant publications. Following the duplicates removal using EndNote X9, records were screened through titles and/or abstracts for relevancy. Full-text articles then were assessed for eligibility.
Study criteria and data extraction
All clinical studies that reported inferior alveolar nerve damage in patients undergoing orthodontic treatment were included in the review. No restrictions on age or language were implemented. Studies that reported IAN damage due to a surgical intervention were excluded.
The following data were extracted from each included study: study information, patients details including their dental abnormalities and orthodontic managements applied. Moreover, type of IAN damage complication, the causative tooth and orthodontic force, and management applied and outcome (e.g. time to recovery) were sought. Any disagreements between the authors on study selection or data extraction were resolved by consensus and discussion with other reviewers if needed. The reporting of this scoping review follows the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for scoping reviews (PRISMA-ScR) checklist [8].
Statistical analyses
Descriptive analyses were performed including the mean, median, and range of various variables from the data extracted. We also fitted a linear regression with recovery time as the outcome to investigate the effects of age, sex, side and region. Results were presented as tables and charts including scatter plot, and box and whisker plot.
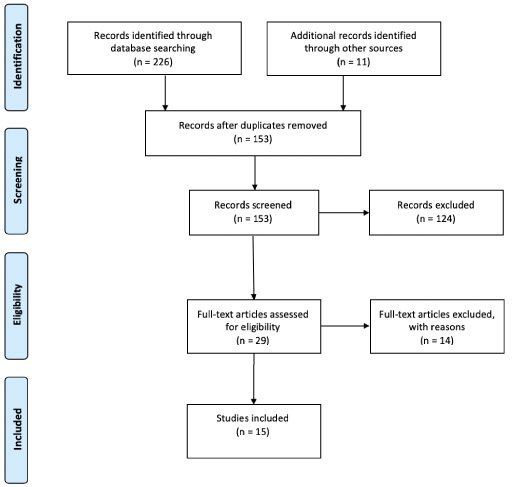
PRISMA flow diagram.
The electronic and manual search yielded a total of 237 records. After duplicates removal, 153 records were screened, of which 124 records were excluded due to irrelevancy. Twenty-nine full-text articles then fully assessed for eligibility and only 15 articles of them met the inclusion criteria (Fig. 1). The main reason for excluding most of the full-text articles was reporting cases with no IAN damage during orthodontic treatment (Appendix). Table 1 shows a summary of the data extracted from the included studies.
A summary of the data extracted from the included studies
A summary of the data extracted from the included studies
The 15 included studies were case reports only and published between 1985 and 2019 from the United Kingdom [9–14], United States of America [15,16], Brazil [17,18], Germany [19], Italy [20], Spain [5], Norway [21], and Canada [22].
Gender and age distribution
A total of 16 patients were included in this review; females (63%, n = 10), males (31%, n = 5), and unknown (6%, n = 1). The overall mean age (SD) was 23.3 (11.6) and the median (min, max) was 19 (12, 57).
Orthodontic management applied to lower dentition
Different indications that warranted orthodontic treatment were observed in the included studies and managed with fixed appliances (88%, n = 14), removable appliance (6%, n = 1), or fixed appliance with temporary anchorage device (TAD) (6%, n = 1).
The complications of IAN damage and areas affected
All the included cases reported temporary sensory alterations following IAN damage and manifested as anesthesia (19%, n = 3), paresthesia (75%, n = 12), or combined (6%, n = 1); mostly on the right side (62.5% RHS n = 10 and 37.5% LHS n = 6). The majority of the damages have affected the mental region (50%, n = 8; RHS n = 4, LHS n = 4) including the lower lip and chin followed by the lower lip only (37.5%, n = 6; RHS n = 4, LHS n = 2). In addition to the extraoral areas, intraoral areas have also been reported to be affected in two cases, one affected the area that innervated by the right IAN and one case affected the area innervated by the right mental nerve branch only. Table 2 shows the descriptive analyses of the included cases regarding the affected areas and the time reported to full recovery.
Descriptive analyses of the included cases in this review
Descriptive analyses of the included cases in this review
The IAN damage was caused by orthodontic movement of all mandibular molars and second premolars following an application of specific orthodontic force such as placement of new archwires, elastics, springs, TAD, or orthodontic adhesive material. The mandibular molars that reported to be the causative factor include lower right first molar/LR6 (n = 1), lower right second molar/LR7 (n = 5), lower right third molar/LR8 (n = 1), lower left second molar/LL7 (n = 4), and lower left third molar/LL8 (n = 1). Whereas mandibular second premolars were reported in six cases including lower right second premolar/LR5 (n = 5) and lower left second premolar/LL5 (n = 1). Most of the studies reported that long roots and close proximity to the IAN canal, or mental foramen while orthodontically moving the teeth were the most likely explanations of such complication.
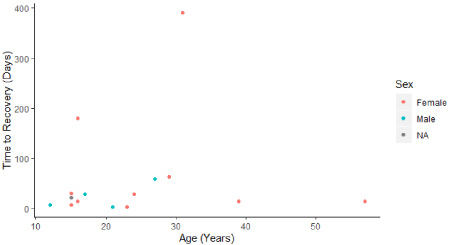
Scatter plot showing the effect of age on recovery duration.

Box and whisker plot showing the effect of gender on recovery duration.
The management of the affected patients were stopping the orthodontic force by inactivating or removing the appliance (75%, n = 12), adjusting the appliance (19%, n = 3), providing a bite plate (13%, n = 2), and/or providing pharmacological management (38%, n = 6). Following the aforementioned managements, all the cases reported to be fully recovered to normal sensation. The time required to fully recover in days calculated as a median (min, max) was 17.5 (2, 390). Figures 2 and 3 show the reported time to recovery in days by age and gender.
Discussion
In this scoping review we identified 15 studies published between 1985 to 2019 which reported 16 different cases of temporary sensory alterations of the IAN secondary to orthodontic treatment. We found that female patients were reported more than male patients with almost two-thirds of overall cases being affected on the right-hand side. The majority of the reported cases with IAN damage due to orthodontics have experienced temporary paresthesia, whereas anesthesia or combined of both alterations were also reported. The temporary altered sensations reported were affecting the mental region including the lower lip and chin, lower lip only, or the intraoral and/or extraoral areas innervated by the IAN. The majority of cases were managed by stopping the orthodontic forces, while the median duration to reach full recovery was 17.5 days.

Intraoral dermatomes innervated by IAN in blue and mental nerve (as IAN branch) in green (including the lower lips).
In order to comprehend the orthodontic movements that may cause IAN damage, one must grasp the basic anatomical course of the IAN (branch of the mandibular nerve V3). The mylohyoid and lingual nerves branch from the main trunk of the mandibular nerve before it enters the mandibular foramen, thus the tongue, lingual mucosa and lower mental symphysis regions were not affected in the included studies of this review [23]. Figure 4 shows the intraoral dermatomes that IAN innervates including its mental nerve (branch of the IAN) as described by Renton and Egbuniwe [23].
Although it is uncommon for a close relationship to exist between the apices of first and second molars or premolars and the IAN canal, it should not be immediately excluded. There are well-documented radiographic signs used, that convey a close proximity of roots to the IAN canal, especially for third molar surgery. Some of these signs are darkening of the root, interruption of white lines of the canal, diversion of canal, deflection of the root, and narrowing of the root or the canal [24,25]. From the studies included in this review, only two studies have reported these signs, one reported darkening of the root and the second reported deviation of the canal [9,13]. In the remainder of the studies none of the previous signs were reported, however excessively long roots were reported in the mandibular second molar in three studies, which may be a specific risk factor [11,19,20]. It has been shown that 2% of lower second molars roots are radiographically related to the IAN canal [26]. Therefore, it is somewhat surprising that paresthesia during orthodontic treatment is not more common.
The majority of studies used panoramic radiographs as pre-operatives. However, if intimate contact between the IAN canal and tooth root is suspected it would be best to take a cone beam computed tomography (CBCT) to investigate these cases and leave the treatment plan uncompromised [12]. The introduction of CBCT imaging provides a more efficient and accurate method to predict the position of teeth roots and the IAN canal especially the bucco-lingual relationship, as it is not revealed in conventional radiography [16]. Numerous studies have been published to compare the sensitivity and specificity of CBCT imaging and panoramic radiographs. In a study by Tantanapornkul et al. [27], CBCT images versus panoramic radiographs were used to determine the diagnostic accuracy of the location of the IAN canal and the roots of third molars prior to extractions. The CBCT images had a higher sensitivity (93% vs 70%) and specificity (77% vs 63%) compared to panoramic radiographs. However, it is not recommended to use CBCT routinely for all orthodontic patients. CBCT should be prescribed only when there is an expected diagnostic benefit for the patient or when there is a significant improvement in the clinical outcome [28]. Moreover, in the advent that paresthesia does develop during orthodontic treatment it is imperative to take a CBCT to rule out a more serious cause.
The main classification method of peripheral nerve injuries is Seddon’s classification [29], which provides important insight in determining the prognosis and treatment strategy. A brief outline of the classification is described below: Neuropraxia: temporary interruptions in conductions of impulse down the nerve fiber, as a result of blunt trauma. Recovery takes place without Wallerian degeneration; hence it is considered to be the mildest form of nerve injury. Axonotmesis: it is a loss of the relative continuity of the axon and its covering of myelin, but preservation of the connective tissue framework of the nerve. Neurotmesis: is the most severe nerve injury, where the nerve is divided. No conduction occur in the nerve and surgical intervention is warranted.
In the majority of the studies that reported mental nerve paresthesia the main teeth affected are the lower second molar and lower second premolar. Moreover, these teeth in the included studies were lingually inclined, which may predispose them to a closer relationship to the IAN canal. The leveling and uprighting would result in the apical part of the root to tilt against the IAN. Additionally, two studies included lower third molars, in one of the studies an intrusive force was applied which compressed the mandibular canal [22]. In the second study, distal movement and uprighting was applied on the lower right third molar, which impinged on the IAN canal [16]. The injuries described earlier are of a mechanical nature due to compression of the nerve by the tooth root during its movement. These compression injuries correspond to neuropraxia in Seddon’s classification. Although clinically they result in sensory dysfunction, but the injury is mild in nature and full recovery is seen within 12 weeks. However, the median recovery duration in the included studies was 17.5 days. If the reported symptoms do not resolve or improve within 2–4 weeks an immediate referral should be made to rule out systemic, intracranial, or extracranial causes. Patel and O’Neill [30] reported a case of a 14-year old male patient who complained of unexplained right-sided facial paresthesia after 9 months of commencing orthodontic treatment; further investigations revealed the patient had a cavernous hemangioma and the symptoms subsided after surgical intervention.
In a total of six studies adjunctive pharmacological management was given, which included steroids, vitamin B, and anti-inflammatory medications. Three out of the six studies provided Vitamin B supplementation. The importance of Vitamin B has been highlighted in several studies which have shown that Vitamin B1, B6, and B12 interact synergistically to improve neuropathy, motor control, nociception, and neuropathic pain [31]. Additionally, an animal study by Altun and Kurutas [32] has shown that supplementation of Vitamin B complex and Vitamin B12 in tissue levels following crush injuries, may be beneficial to nerve regeneration. Moreover, a clinical study by Sun et al. [33] reported that early steroid therapy has been successful in reducing nerve injury associated neuroinflammation, which may lead to accelerated function recovery of nerves. However, no current evidence exists to favor prescribing medication to alleviate the inferior alveolar anesthesia or paresthesia. In the remainder of the studies the clinicians either removed the appliance and stopped the orthodontic treatment or commenced forced interruption followed by tooth extrusion. A systemic review by Coulthard et al. [7] found the quality of evidence to be very low to investigate the effectiveness of surgical, medical and psychological factors for iatrogenic inferior alveolar and lingual nerve damage. Under the current scope of evidence, no recommendation can be made on prescribing medication to help alleviate the paresthesia.
To emphasize, using clear aligners as an orthodontic option is increasing dramatically, especially with the current advances and technologies available in the orthodontic field. There is a clear trend of providing such treatment not only by orthodontists, but general dentists as well. The studies included in this review have been affected with IAN damage secondary to orthodontic treatment, even though almost all cases were treated by orthodontists. Thus, experienced clinicians in orthodontics should be the orthodontic treatment providers for patients with high or unclear proximity to the IAN. Moreover, several companies have launched their services to provide a direct-to-consumer or “DIY” orthodontics, in which the patients might not be examined or evaluated clinically in person, but remotely and asked to take their own impression or having an intraoral scan in-store [34]. The legal and ethical implications will not be discussed, but its clinical implications should be clearly emphasized. No studies so far have been carried out to investigate whether clear aligner providers of the aforementioned services are relying on intraoral scans or self-impressions mainly to provide such treatment and if further radiographic investigation were taken such as panoramic or CBCT for patients with close or unclear proximity to the IAN. Also, a new teleorthodontics concept has been utilized for clear aligner providers to monitor the orthodontic progress with their patients remotely; in which intraoral images be taken by the patients’ smartphones regularly [35]. However, whether radiographic evaluation was implemented in such new technology during the remote orthodontic treatment journey was not clear. Therefore, questioning the radiographic surveillance in orthodontic patients with high risk of IAN damage is inevitable.
The main limitation of this scoping review was the number of cases identified due to the rarity of the complication reviewed. However, IAN damage secondary to orthodontic treatment is emerging in the literature and worth emphasizing the etiological factors and management modalities in such cases. Proper clinical examination including radiographical investigations is a standard of care, and dental practitioners should only provide orthodontic treatment with competency within their scope of clinical practice. Identifying patients with high or unclear proximity to the IAN canal should be dealt professionally while putting the patients’ best interests first.
Footnotes
Acknowledgements
The authors would like to thank Dr Barrak Alahmad from Harvard T.H. Chan School of Public Health, Harvard University, for his genuine help in performing the statistical analyses of this study.
Conflict of interest
None of the authors declare any conflict of interest relevant to this article.
Ethical approval
Not applicable.
Table showing the reasons for studies exclusion
| No. | Study | Exclusion reason |
| 10 | Celebi N, Canakci GY, Sakin C, Kurt G, Alkan A. Combined orthodontic and surgical therapy for a deeply impacted third molar related with a dentigerous cyst. J Maxillofac Oral Surg. 2015;14(Suppl 1):93–5. | No IAN damage reported during orthodontic treatment. |
| 11 | Kalantar Motamedi MR, Heidarpour M, Siadat S, Kalantar Motamedi A, Bahreman AA. Orthodontic Extraction of High-Risk Impacted Mandibular Third Molars in Close Proximity to the Mandibular Canal: A Systematic Review. J Oral Maxillofac Surg. 2015;73(9):1672–85. | Not a clinical study. Systematic review on orthodontic extraction. |
| 12 | Ma Z, Xu G, Yang C, Xie Q, Shen Y, Zhang S. Efficacy of the technique of piezoelectric corticotomy for orthodontic traction of impacted mandibular third molars. Br J Oral Maxillofac Surg. 2015;53(4):326–31. | No IAN damage reported during orthodontic treatment. |
| 13 | Huang TT, Chang CJ, Chen KC, Lo JB, Chen MY, Huang JS. Outcome Analysis and Unexpected-Scenario Prediction in 2-Stage Orthodontic Lower Third Molar Extraction. J Oral Maxillofac Surg. 2018;76(3):503.e1–.e8. | No IAN damage reported during orthodontic treatment. |
| 14 | Wang Z, Liu Z, Shi Y, Fang D, Li S, Zhang D. A Novel Orthodontic Extraction Method for Removal of Impacted Mandibular Third Molars in Close Proximity to Inferior Alveolar Nerve. Journal of Oral and Maxillofacial Surgery. 2019;77(8):1575.e1–.e6. | No IAN damage reported during orthodontic treatment. |