
Abstract
OBJECTIVE:
This study aimed to investigate the knowledge, usage and attitude of physiotherapists towards non-steroidal anti-inflammatory drugs (NSAIDs) in Karachi, Pakistan.
METHODS:
A cross-sectional study was conducted among clinical physiotherapists working in Karachi who were enrolled through convenient sampling. A questionnaire was distributed to the participants, which consisted of questions regarding physiotherapists’ current knowledge, current practice and their attitude towards NSAIDs prescription.
RESULTS:
Responses of 310 physiotherapists out of the 350 questionnaires distributed were received (response rate = 88%). Results show that most physiotherapists (60.3%) recommended NSAIDs to their patients despite having a variable understanding of the contraindications, adverse reactions and drug interactions of NSAIDs. Most physiotherapists demonstrated poor knowledge of the legislation on NSAIDs prescription as most of them believed that they were allowed to advise (71.9%), prescribe (66.1%) and recommend (72.2%) NSAIDs to their patients.
CONCLUSION:
This study implicates that physiotherapists should be trained through proper educational sessions such as certification courses on pharmacotherapy (specifically pain medications) in order to become certified to prescribe NSAIDs and other analgesics.
Introduction
Non-steroidal anti-inflammatory drugs (NSAIDs) are one of the most commonly prescribed pain medications. The major therapeutic actions of NSAIDs are pain suppression (analgesia), reducing body temperature in fever (antipyretic effect) and reducing inflammation (anti-inflammatory effect). These drugs are widely used for painful conditions such as rheumatoid arthritis and gout and are also useful in treating mild to moderate fever [1]. NSAIDs are also responsible for approximately one-quarter of all adverse drug reaction reports [2] such as gastro-intestinal (GI) damage, inhibition of platelet aggregation and decreased kidney function. Due to these adverse side effects, the overuse of NSAIDs should be restricted as much as possible [1].
Among the healthcare professionals in Pakistan, only medical doctors are allowed to directly prescribe medications to their patients. In the UK, physiotherapists have been given the role of supplementary prescribers in 2003 and later in 2013 they were listed as independent prescribers [3]. The concept of supplementary prescription can be beneficial to the patients as their pain medications will be managed directly by the physiotherapists making the process cost-effective and early recovery can be possible [4]. It can also be beneficial to physicians as they will be able to focus on treating patients with critical illnesses or acute conditions. Physiotherapists must acquire extensive knowledge of pharmacotherapy in order to become supplementary prescribers [5]. In the UK, additional educational sessions are held including clinical practice in order to train physiotherapists to become prescribers [6].
NSAIDs are commonly used for musculoskeletal injuries such as strains and sprains as they involve inflammation and intense pain. Although inflammation is a necessary component of the healing process, anti-inflammatory drugs can be counter-productive and can delay the process of healing by blocking the inflammatory phase. But the reason behind its frequent prescription is that it helps in quick pain relief. For acute musculoskeletal injuries, oral analgesics are recommended for pain management [7]. In countries like Australia and New Zealand, prescribing medications is considered to be outside of physiotherapy practice, but it appears that physiotherapists often recommend medications like analgesics and NSAIDs to their patients [7].
There are various risk factors associated with NSAIDs affecting the GI tract, central nervous system (CNS) and cardiovascular system. NSAIDs may produce cardiovascular events such as myocardial infarction (MI) and ischemia. Recent studies have shown links between NSAIDs (both selective and non-selective) and adverse cardiovascular events [8]. In July 2015, the Food and Drug Administration (FDA) updated a statement of warning on non-aspirin NSAIDs which emphasized on the increased risk of MI and/or cerebrovascular accident (CVA) in patients taking these drugs [9]. Topical NSAIDs are known to have lower adverse effects because of their low tissue concentration of the active ingredient; still some patients experience adverse reactions such as skin and gastric irritation, asthma and renal impairments [8]. Research suggests that chronic NSAID use increases the risk of death from bleeding or perforated gastro-duodenal ulcers [8]. A study of the US shows that 16,500 NSAID-related deaths occur among patients with rheumatoid arthritis or osteoarthritis every year [10]. As some NSAIDs are over-the-counter drugs, they are frequently used for treating painful conditions and musculoskeletal injuries [11]. A study in Pakistan has shown the irrational prescribing habits of physicians regarding NSAIDs, low awareness in the public about the adverse effects and long-term dependency on NSAIDs [12].
To date, no study has been conducted in Pakistan which evaluates the knowledge and attitude of physiotherapists towards prescribing NSAIDs to patients. This study is based on the concept that physiotherapists should have sufficient knowledge of pharmacotherapy in order to manage their patients’ chronic pain by prescribing accurate medications during their treatment sessions. The objective of this study is to investigate the knowledge, usage and attitude of physiotherapists towards NSAIDs in Karachi, Pakistan.
Methodology
A cross-sectional approach was used to investigate the knowledge, attitudes and usage of NSAIDs among clinical physiotherapists working in various government hospitals, private physiotherapy clinics and NGO-based clinics throughout Karachi. A total of 350 clinical physiotherapists were approached in this study using convenience sampling (a non-probability sampling technique used to draw participants from a population that is close to hand) and among them 310 physiotherapists responded. The sample size for this study was calculated using the OpenEpi online sample calculator [13]. The participants were asked to fill out the questionnaires which included the consent form, demographic data and main questionnaire form. Informed consent was obtained prior to participation and each participant was informed about the objective of this study. Ethical approval for this study was provided by the Institutional Review Board of Jinnah Postgraduate Medical Centre.
The questionnaire was adapted from a previous study by Grimmer et al. [14] (see Appendix) which contained 18 items, both open- and close-ended questions and had the following four sections: Physiotherapist’s demographics, knowledge of NSAIDS and their quality use, current use of NSAIDs in clinical practice and attitude towards the use of NSAIDS in clinical practice.
Data analysis
Data was analyzed using the software SPSS version 23.0 [15]. Descriptive statistics were used, i.e. frequencies and percentages were taken for each response and results were summarized in the form of tables and figures. For the open-ended items that measured physiotherapists’ knowledge of NSAIDs, key themes were made to categorize the responses which were then compared to the correct answers. Frequencies and percentages were calculated for the correct and incorrect responses.
Results
Responses from 310 physiotherapists out of the 350 questionnaires distributed were received, giving a response rate of 88%. Among the 310 respondents, 66% were females (n = 205) and 34% were males (n = 105). The most common age group reported was 21–25 years (34.5%). About 58.7% of the physiotherapists had clinical experience less than or equal to five years. Among the total sample, 63.5% of the physiotherapists worked at private outpatient clinics, 29.4% at government hospitals and 7.1% at NGO-based clinics.
In the demographic section of the questionnaire, participants were asked about their recent knowledge update on NSAIDs, to which the responses were: ‘Less than one year’ (32%), ‘recently’ (30%), ‘1–5 years’ (17%), ‘never’ (10%), ‘5–10 years’ (6%) and ‘more than 10 years’ (5%). Most respondents (74.5%) stated that they had actively sought information on NSAIDs for which the most common sources were ‘Via another physiotherapist’ (51.5%), ‘Journal articles’ (43.7%), ‘General medical practitioner’ (40.7%), ‘Training schools’ (32%), ‘Direct from drug companies’ (26%), ‘Advertising campaign’ (22.1%), ‘Local pharmacist’ (21.6%), and ‘Others’ (12.6%). The majority of the physiotherapists stated that they obtained this information via another physiotherapist.
Knowledge of NSAIDs
Participants were asked about the availability of common NSAIDs, i.e. they are either available over-the-counter or by doctor’s prescription. The majority of the respondents correctly identified over-the-counter drugs while some reported incorrect answers. From the drugs mentioned in the questionnaire, over-the-counter drugs were Indocid, aspirin, Voltaren gel, Feldene gel, Digesic and Voltral tablets. Among the other three drugs, ACT-3 (trade name for ibuprofen) is not available in Pakistan, and Celebrex (celecoxib) and Neurofen (ibuprofen) brands are not commonly used and other brands were used instead. Therefore, the responses for these three drugs were not considered valid.
The most common correct responses for risk factors of oral NSAIDs were gastrointestinal tract (GIT)-related risks (55%), renal complications (20.6%), cardiovascular risks (15.8%) and allergic reactions (14.5%). For topical NSAIDs, the correct responses were skin irritation (29.4%), skin rashes (19.6%), burning and redness of skin (18.6%) and allergic reactions (20.6%).
Common conditions for which NSAIDs are recommended as reported by the respondents were arthritis (34.1%) (including osteoarthritis and rheumatoid arthritis), soft tissue injuries (15.1%), back pain (13.3%), pain management (22.1%), frozen shoulder (6.2%), inflammatory conditions (15.1%), headache (2.9%) and others (11.8%). Only 4.1% incorrect answers (e.g. diarrhoea, pregnancy, lung diseases) were received; most respondents reported correct information.
When asked about the drugs which may interact with NSAIDs, the respondents provided a wide variety of drugs containing both correct and incorrect answers. Among these the most frequent correct answers were corticosteroids (n = 63), diuretics (n = 48), ibuprofen (n = 29), aspirin (n = 28), lithium (n = 27), beta-blockers (n = 23) and others. Although aspirin and ibuprofen belong to the NSAIDs category, their collateral use may be harmful to the patients. The majority of physiotherapists showed a poor knowledge of drug interactions and most of the responses were left blank for this question.
When asked about the conditions for which NSAIDs may be contraindicated, the respondents reported GIT problems (34.9%), kidney problems (17.3%), pregnancy (14.5%), cardiovascular pathologies (12.6%), allergic to the drug (9.5%), liver problems (6.9%) and bone pathologies (3.5%). Only 2.8% incorrect answers (e.g. acute pain, chronic pain) were received; the majority of the responses were correct. The adverse reactions reported by the respondents were GIT disturbances (44.4%), kidney problems (13.9%), skin problems (6.5%), allergic reactions (11.3%) and cardiovascular pathologies (5.5%). Also, only 22% of the respondents reported having seen patients that experienced adverse reactions to NSAIDs in their daily practice.
An overview of the physiotherapists’ knowledge of the legislation is reported in Table 1. The majority of the respondents believed that they were allowed to advise, prescribe and recommend NSAIDs to their patients.
Physiotherapists’ knowledge of the legislation regarding NSAIDs
Physiotherapists’ knowledge of the legislation regarding NSAIDs
About 60.3% of the physiotherapists stated that they recommended NSAIDs to their patients in their daily practice among which over-the-counter oral medications (47.1%) and over-the-counter topical medications (33.9%) were the most common recommendations. The recommendation that patients must seek the guidance of a general physician was reported by 27.9% respondents while 15% said they would refer to a pharmacist. Factors considered by physiotherapists before recommending NSAIDs are given in Fig. 1.
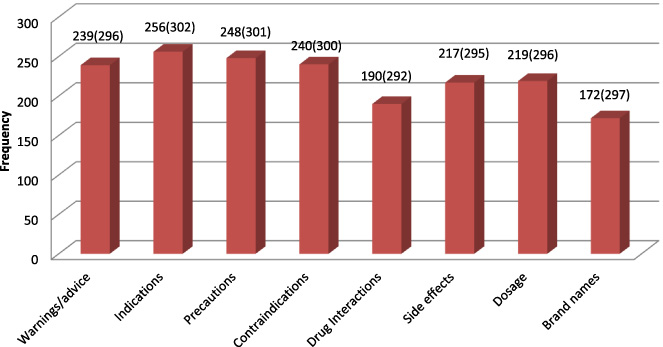
Factors to be considered before recommending NSAIDs. (Note: The numbers above the bars indicate the number of respondents who answered yes followed in parentheses by the total sample size for each question.)
When asked which NSAIDs they recommended, respondents reported a wide variety of medications among which the most frequent were Nuberol Forte 15.5% (paracetamol + orphenadrin citrate) (which in fact does not belong to the NSAID category), diclofenac sodium 10.3%, Voltaren gel 10.3% (diclofenac diethylammonium), ibuprofen 7.1%, aspirin 6.1% and others 26.6%, while about 23.5% responses were missing.
When asked whether they record any discussions on medications in their clinical records, 66.7% reported that they did not record any discussions on medications in their clinical records. In the “Current Practice” section of the questionnaire, participants were asked about the sources they have used to obtain information on NSAIDs in the past six months (demonstrated in Table 2). The most common source reported was Internet sources on drugs. A similar question was asked in the demographics section with the intention to check whether the physiotherapists voluntarily updated their knowledge on NSAIDs in the recent time period. Those who answered yes were further asked about the sources similar to those in this question with three additional options, i.e. “Via another physiotherapist”, “training schools” and “advertising campaign”.
Sources used to obtain information on NSAIDs in the past six months
When asked whether they believed that physiotherapists should be allowed to prescribe NSAIDs, 82.5% of the participants stated that they believe physiotherapists should be able to prescribe NSAIDs (see Fig. 2). When asked whether they have enough knowledge about NSAIDs to advise patients on its safe use, 62.5% of the respondents believed that they had enough knowledge of NSAIDs.
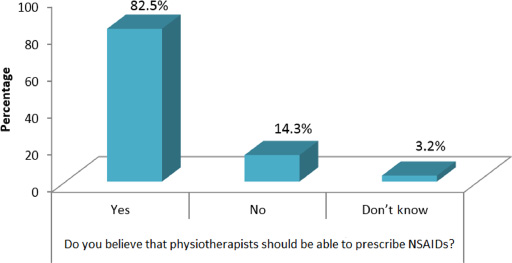
Physiotherapists’ attitude towards NSAIDs prescription.
When asked who they think is responsible for educating physiotherapists about NSAIDs, 72.5% of the respondents stated that physiotherapists are responsible and 59.9% stated that training schools are responsible (see Table 3).
Who should be responsible for educating physiotherapists about NSAIDs?
This study indicates that most physiotherapists in Karachi recommend NSAIDs to their patients, although they lack comprehensive knowledge of NSAID usage, and especially knowledge of adverse reactions and drug interactions. When inquired about their knowledge on legislation, the majority of physiotherapists believed that they were allowed to advise, prescribe and recommend NSAIDs, when in reality these acts are prohibited for physiotherapists in Pakistan. In contrast, the study by Noronha et al. [16] shows that there were lower percentages of respondents who believed that they were allowed to advise, prescribe and recommend NSAIDs, given that their country legislation also forbids physiotherapists to perform these actions. Also, the study by Lansbury et al. [19] showed that the majority of the respondents advised patients about prescription medications although most of them stated that they had insufficient knowledge of pharmacology.
When asked about risk factors of oral NSAIDs, most respondents reported GIT-related risks while fewer responses were reported for cardiovascular, kidney and allergic conditions. Although the risks factors of oral and topical NSAIDs are almost identical [17], in this study, most respondents reported skin irritations and allergic reactions as the main risks of topical NSAIDs. Topical NSAIDs are much safer than oral NSAIDs, but adverse reactions still occur such as gastric irritation, asthma and renal impairments [8]. These findings are similar to the study by Green et al. [8] which also identified the status of knowledge, usage and attitude of physiotherapists towards NSAIDs. Our results also demonstrated that arthritis, pain management and soft tissue injuries were the most commonly reported clinical indications for NSAIDs; which are all correct, demonstrating a satisfactory knowledge for the clinical indications for NSAIDs. Similar findings are seen in the study by Grimmer et al. [14], which also investigated physiotherapists’ knowledge, use and attitude towards NSAIDs; in this study, the most commonly reported conditions reported were osteoarthritis, rheumatoid arthritis and musculoskeletal injuries.
Responses for drug interactions include corticosteroids, diuretics, lithium and beta-blockers along with ibuprofen, aspirin and diclofenac even though they belong to the same category of anti-inflammatory drugs but their interaction may cause harmful effects. Only a few respondents have reported antihypertensive drugs (n = 8), anti-coagulants (n = 3), warfarin (n = 4) and anti-depressants (n = 4). Most physiotherapists are unaware of the drug interactions of NSAIDs. Contrary to these findings, the study by Green et al. [8] shows that the majority of the respondents reported anti-coagulants, anti-hypertensive drugs and other NSAIDs. But the researchers concluded that there is limited knowledge of NSAIDs among physiotherapists in this area, as only a few respondents who recommended NSAIDs correctly identified these drug interactions. Also, most respondents have stated that they do not record any discussions on drug usage in clinical records. This is an alarming sign as most of them recommend NSAIDs to their patients.
Most respondents stated that they believe physiotherapists should be able to prescribe NSAIDs while only a few stated that they have no role in NSAIDs prescription. Although most respondents stated that they have sufficient knowledge of NSAIDs, the study concludes that they have insufficient knowledge. In contrast, the study by Noronha et al. [16] shows that most physiotherapists believed they are not qualified enough to prescribe NSAIDs. A study by Kumar and Grimmer [18] highlighted the ‘grey areas’ concerning the use of topical NSAIDs in physiotherapy management and recommending oral NSAIDs to patients. This study shows there is a lack of proper knowledge on NSAIDs among physiotherapists.
Physiotherapy undergraduate programs need to update their courses on medications and pharmacotherapy in order to properly educate physiotherapists regarding every aspect of NSAIDs prescription and other analgesic medications.
Conclusion
In conclusion, most physiotherapists recommend NSAIDs to their patients despite having a poor understanding of the health risks, adverse reactions and pharmacological interactions of NSAIDs. As physiotherapists are expected to practice within their domain of expertise, this study shows that most of them are in fact practising outside their domain, i.e. they advise and recommend pain medications in their practice settings. This study implicates that physiotherapists should be trained through educational sessions such as certification courses on pharmacotherapy (in particular pain medications) in order to become certified to prescribe NSAIDs and other analgesics. Also, the government should make appropriate legislative changes about physiotherapists’ roles and responsibilities in terms of medication prescription. These efforts will prove to be helpful for physiotherapists that incorporate pain medications in their practice in a way that is evidence-based and safe for the patients.
Footnotes
Acknowledgements
The authors would like to thank their mentors for their valuable guidance and support during the process of this research project. They are also thankful to their classmates for their help and cooperation.
Conflict of interest
The authors have no conflict of interest to report.
Questionnaire (adapted from Grimmer et al.)
(Please tick the correct response)
1. Age:
○ 21–25 ○ 31–35 ○ 41–45
○ 26–30 ○ 36–40 ○ 46–50
2. Gender:
○ Male ○ Female
3. Year of graduation:_____________________________
4. Which province are you from?
○ Sindh ○ Baluchistan
○ Punjab ○ KPK
5. Where are you currently practicing:
○ Private outpatient clinic ○ NGO based clinic
○ Government hospital
6. When did you last update your knowledge on NSAIDs:
○ Never ○ Less than one year ○ 5–10 years
○ Recently ○ 1–5 years ○ More than 10 years
7. Did you seek out this information yourself?
○ Yes
○ No
* If yes, how did you obtain this information (tick as many as required):
○ Via another physiotherapist
○ Journal articles
○ Direct from drug companies
○ General medical practitioner
○ Local pharmacist
○ Training schools (e.g. university)
○ Advertising campaign
○ Other:____________________________
1. Where are the following medications obtained:
2. List the risks you know are associated with the use of NSAIDS:
3. Legislation allows (please tick the appropriate response):
∙ Physiotherapists to advise on the use of NSAIDs
○ Yes ○ No ○ Don’t know
∙ Physiotherapists to prescribe NSAIDs
○ Yes ○ No ○ Don’t know
∙ Physiotherapists to recommend NSAIDs:
○ Yes ○ No ○ Don’t know
∙ Physiotherapists to supply oral NSAIDs:
○ Yes ○ No ○ Don’t know
∙ Physiotherapists to supply topical NSAIDs:
○ Yes ○ No ○ Don’t know
∙ Physiotherapists to use NSAIDs in patient treatment:
○ Yes ○ No ○ Don’t know
4. List three conditions for which NSAIDs are recommended as part of management:
1._________________________________________
2._________________________________________
3._________________________________________
5. List three common drugs with which NSAIDs interact:
1.__________________________________________
2.__________________________________________
3.__________________________________________
6. List three conditions for which NSAIDs may be contraindicated:
1.__________________________________________
2.__________________________________________
3.__________________________________________
7. List common adverse reactions to NSAIDs:
1.__________________________________________
2.__________________________________________
3.__________________________________________
8. Do you know if any of your patients had adverse reactions to NSAIDs?
○ Yes○ No○ Don’t know
*If yes, briefly describe: __________________________
1. Does your practice/institution have a policy regarding physiotherapists recommending NSAIDs to patients?
○ Yes ○ No ○ Don’t know
*If yes – Do you follow this policy?
○ Yes ○ No
*If no or don’t know – Do you think such a policy would be beneficial?
○ Yes ○ No ○ Don’t know
2. Do you commonly recommend NSAIDs to your patients?
○ Yes ○ No
(Tick as many as required)
○ Over-the-counter oral medication ○ Over-the-counter topical medication
○ Prescription oral medication ○ Refer to GP
○ Prescription topical medication ○ Refer to pharmacist
3. Do you consider the following facts before recommending NSAIDs?
Warnings/advice Yes ○ No ○ Drug interactions Yes ○ No ○
Indications Yes ○ No ○ Side effects Yes ○ No ○
Precautions Yes ○ No ○ Dosage Yes ○ No ○
Contraindications Yes ○ No ○ Brand names Yes ○ No ○
4. Which NSAIDs do you usually recommend? _________________________________
5. Do you record any discussions on medications in your clinical records?
○ Yes ○ No
6. Which of the following sources have you used in the past six months to find out about NSAIDs?
○ Current MIMS (Medical Inventory ○ Instructions on packets
Management System) drug database ○ Drug company information
○ Internet sources on drugs ○ Drug company studies
○ Medical practitioner ○ Other
○ Pharmacists ○ None
○ Research papers
1. Do you believe that:
a) Physiotherapists should be able to prescribe NSAIDs?
○ Yes ○ No ○ Don’t know
b) You have enough knowledge about NSAIDs to advise patients on safe use?
○ Yes ○ No ○ Don’t know
2. Whose responsibility do you think it is to provide information on NSAIDs to physiotherapists?
(Tick as many as you wish)
○ Physiotherapists should seek it themselves
○ Drug companies
○ Local pharmacists
○ General practitioners
○ Training schools (e.g. School of Physiotherapy/Pharmacy in a university)
○ Physiotherapy conferences
○ Other (please describe):________________________________________
3. Could you summarize your attitude towards the place of NSAIDs in physiotherapy practice?
_______________________________________________________________________________
_______________________________________________________________________________