
Abstract
BACKGROUND:
Human error has been studied for large decades with special application to critical infrastructures and processes where the impact of such errors can induce severe or catastrophic consequences. In this sense it is of utmost importance to extend this type of analysis to other fields as medicine.
OBJECTIVE:
This study proposes a semi-quantitative human error risk assessment methodology, including the analysis of the so-called Performance Shaping Factors (PSFs), in order to contribute to health services improvement.
METHODS:
A questionnaire including the considered PSFs is answered in order to determine the impact of each PSF and its influence on human error. It allows performing a Human Error Risk Assessment (HERA) for both the patient (HERAp) and the quality of the service (HERAq).
RESULTS:
The results show the PSFs with the highest impact factor. After applying corrective measures, it is possible to observe the impact on the reduction of the risk for patient and for the quality of the service.
CONCLUSIONS:
The application of the methodology with the inclusion of the impact of PSFs allows minimizing or mitigating failure modes with greater risk as well as increasing patient safety and promoting a better quality of medical procedures.
Introduction
Currently, the practice of medicine is considered a risky activity mainly for the patient [1]. Errors occur due to the high complexity of mostly health care services, leading to the occurrence of adverse or undesired events [2]. Failures in communication and ineffective teamwork are examples reported as frequent sources of patient safety problems. It is necessary that the strategies meet the patient’s safety needs more effectively and efficiently [3]. By organizing resources more effectively according to health needs, eliminating waste and working for prevention and care and in a safe mode, the service can be considered as a quality healthcare service [4].
Since the 1990s with the Harvard Medical School study and later the IOM (Institute of Medicine) report - “To Err is Human”, patient safety has been placed on the public health agendas of several countries worldwide and it has been argued that the majority of adverse events that occur in health care services, about half of them are due to preventable human errors, with high associated costs, in the order of millions [1,5,6]. Breaches of security occur in various areas of health care, but it is in a complex system such as the Operating Room that events are more serious and with greater impact and much more frequent than what would be desired [2]. It is essential to apply a set of proactive measures for adverse events [2].
The “human error”, should be seen centered on the system and not on people who work in health care services, where errors are seen as consequences and not as causes [6–8]. To do so, it must be applied a proactive risk management instead of a reactive one [7]. It is here that the methodology proposed in this paper can play a fundamental role.
Complex systems and human error have been studied for a long time in the industry through Human Reliability Analysis (HRA) methodologies to quantify and reduce the probability of “human error” [9]. For mapping a process and identifying points of weakness or risk, methodologies such as Failure Mode and Effects Analysis (FMEA) or Fault Tree Analysis (FTA) are used [10].
Performance Shaping Factors (PSFs), or sometimes also referred as Performance Influencing Factors (PIFs), are any factor that affects human performance [10], whether personal, environmental or behavioral, in a qualitative way to identify the contribution of human performance or in a quantitative way to calculate the Human Error Probability (HEP) [11]. The HRA methodology that best defines PSFs is SPAR-H, referring factors as time available, stress, complexity, experience, training, procedures, man-machine interface factors and physical fitness [12].
For these reasons PSFs are very important and must be taken into account, as they influence behavior, affect performance and consequently “human error”, with consequences, leading to failures and wrong responses in complex systems [10].
Human factors have been an interest of study for some time. Kossaify et al. [13] published a review of thirty-three papers dealing with factors affecting the quality of care in health care institutions. As reported by the authors issues affecting teamwork include mainly self-awareness, work environment, leadership, ethics, cooperation, communication and competition. Zhao et al. [14] developed a work to seek consensus-based indices for quality assessment of the public health service to evaluate the service quality of public health in Shenzhen and other cities in China. Vasconcelos et al. [3] identified the attributes for patient safety at a primary healthcare level and analyzed conceptions of patients, professionals, and managers about how these attributes were being addressed. An investigation about the tools used to assess safety culture in the primary health care was also performed [15].
One of the methodologies that have been applied to health systems is the Failure Modes and Effects Analysis (FMEA) in a way to assess the risk of items or process failures to identify the most important areas for improvement [16]. This methodology can be exemplified by some works, as the one developed by Battaglini et al. [17] for a risk assessment on a hematology ward renovation in a tertiary hospital in Italy or the study performed by Celotto et al. [18] in a way to prevent and contrast violence on healthcare workers.
FMEA follows the importance given to the concept of quality and patient safety, referred to as a risk analysis methodology by the ISO 31010 standard [19] and presenting itself as a strong risk analysis methodology, advised by organizations such as the Joint Commission International (JCI), so that each Hospital performs a proactive annual risk assessment [20]. Although the FMEA has advantages in allowing the prioritization of failures and implementing corrective measures in order to reduce the probability of occurrence and increase security [16], usually it does not include PSFs [21]. It is in this sense that this work appears, in order to create a modified FMEA for health sector (mhFMEA) that takes into account the PSFs in the risk analysis of a health care system.
Determining the probability of occurrence of human error.
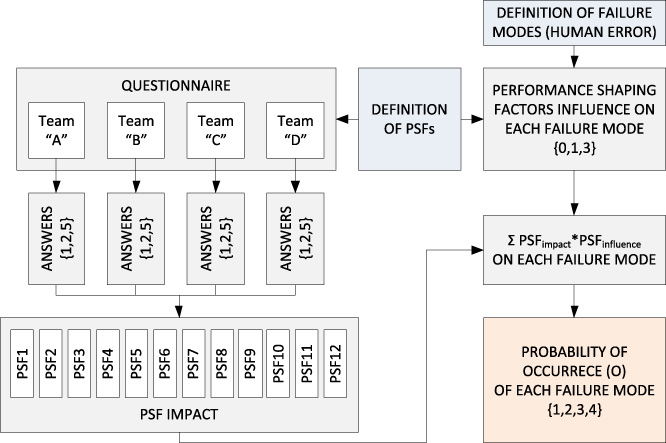
In order to understand the mhFMEA methodology proposed in this work, Fig. 1 illustrates the main steps to perform just to obtain the probability of occurrence (O) of each failure mode (human error). To determine the impact of each PSF at the initial stage of the mhFMEA methodology, an anonymous questionnaire is applied to each team of health professionals in a health care service. The selected twelve PSFs under consideration on the questionnaire of the proposed methodology were:
PSF1 – Available time PSF2 – Task complexity PSF3 – Experience PSF4 – Training PSF5 – Psychological stress/stressors PSF6 – Physiological stress/stressors PSF7 – Operating protocols PSF8 – Man-machine interface/ergonomics PSF9 – Task adequacy PSF10 – Teamwork performance PSF11 – Environmental conditions PSF12 – Organizational factors
A factor is assigned to each team of health professionals (1, 2 or 5) for each PSF resulting from the answers of the anonymous questionnaire (see Table 1). Then, for each PSF an average number is achieved, considered as the PSFimpact. The impact of each PSF represents the average of all teams involved in the process. After determining the impact of each PSF and identified all potential failure modes (FMs) underneath the service in analysis, the influence of each PSF on each failure mode is discussed and a weight is determined taking into account if it has:
Direct influence (3); Some influence (1); No influence (0).
Then, for the determination of the probability of occurrence (O) of each failure mode it is firstly used the following expression:
Performance Shaping Factors (PSF) questionnaire
Probability of occurrence of each failure mode (human error)
On the development of the mhFMEA methodology follows a second stage that corresponds to the determination of the severity of the consequences of each failure mode (human error). Tables 3 and 4 show how to achieve the severity index (S) for the patient and for the quality of service, respectively.
Severity for patient of each failure mode (human error)
Severity for quality of each failure mode (human error)
In the last step of the mhFMEA methodology, the possibility of avoiding (E) each failure mode (human error) is evaluated through the existing controls. Table 5 shows how to determine the avoiding possibility index (A).
Avoiding possibility of failure mode (human error)
To perform the final step of the proposed methodology concerning the determination of the Human Error Risk Assessment (HERA) for each failure mode (human error) the following expressions are used for the patient (HERAp) and for the quality of the service (HERAq), respectively:
In order to finish the analysis and implement measures to decrease the risk of each failure mode (human error) based on HERAp and HERAq, it must be followed a risk matrix, as shown in Table 6.
Risk classification matrix
Subsequently, failure modes are prioritized for the application of corrective measures.
In this study, the mhFMEA was applied on the Operating Room of one of the main Hospitals in Portugal and the teams involved were: Anesthesiology team, Surgery team, Nursing team and Medical Action Assistants team.
The impact of each PSF, resulting from the average of the multiplication factors attributed to each team of health professionals, based on the anonymous questionnaire are:
PSF1 – Available time: (2.50) PSF2 – Task complexity: (3.50) PSF3 – Experience: (1.00) PSF4 – Training: (2.00) PSF5 – Psychological stress/stressors: (3.50) PSF6 – Physiological stress/stressors: (3.50) PSF7 – Operating protocols: (5.00) PSF8 – Man-machine interface/ergonomics: (2.50) PSF9 – Task adequacy: (1.50) PSF10 – Teamwork performance: (2.25) PSF11 – Environmental conditions: (2.00) PSF12 – Organizational factors: (4.25)
In this study, 58 failure modes related to the preoperative, perioperative and postoperative stages were identified. In a way to better illustrate the methodology a simple example will be followed throughout the rest of the work. In this case we will follow from now on the example of FM8 (Anaphylactic reaction/ignorance of known allergy in the patient). After determining the influence of each PSF on the failure modes, the probability of occurrence (O) of each failure mode was achieved as well as the severity of the consequences for the patient (Sp), the severity of the consequences for the quality of the service (Sq) and the possibility to avoid (A) each failure mode, as previously explained. For FM8 all PSFs have direct influence (score 3) except PSF1, PSF8 and PSF12 where it was considered that could have some influence (score 1). Based on this, FM8 reaches a score of 82 points that, according to Table 2, corresponds to a probability of occurrence (O) of 3 (meaning probable). For this FM it was considered a Sp of 5 (death of the patient), a Sq of 4 (serious non-compliance) and a A of 4 (low possibility of avoiding the failure mode).
HERAp and HERAq were then calculated and a prioritization of the failure modes was made taking into account the classification of the risk of human error for the patient on HERAp and the quality of the service on HERAq. Table 7 shows the results of such classification. As it can be seen in Table 7 the FM8 is considered “Unacceptable” for HERAp (60) and “Acceptable with remarks” for HERAq (48).
Classification of failure modes (human errors)
Classification of failure modes (human errors) after the implementation of recommendations
This results lead to the proposal of application of corrective measures individually for the teams of health professional, related to the PSFs that result in higher risk, in a way to decrease the probability of occurrence of the most critical failure modes (human errors). Based on the fulfillment of these recommendations a new risk classification of the failure modes (human errors) was performed, as shown in Table 8. The recommendations were designed to be directed to the PSFs with the greatest impact on the surgical process. Some of these recommendations were related to:
Making the use of understandable and appropriate action protocols mandatory for the tasks (PSF 7) Promoting the reduction of the complexity of the technology involved (PSF 2) Applying strategies to reduce psychological stress (PSF 5) Applying strategies to reduce physical stress (PSF 6) Application of measures to increase skills and knowledge that promote teamwork (PSF 10) Promotion and participation in actions related to the surgical acts to be performed every 2 years (PSF 4)
Returning to our example of FM8, the answers to the questionnaire after the implementation of all recommendations allowed to observe a new score of 42 points that, according to Table 2, corresponds to a probability of occurrence (O) of 2 (meaning unlikely). Thus, HERAp (40) and HERAq (32) are both now considered “Acceptable with remarks”.
In cases where the failure modes are unacceptable or acceptable with remarks but with low probability for the probability of occurrence (O), the implementation of other corrective measures may be important in preventing or avoiding (A) the occurrence of these failure modes, with impact on the severity of the consequences for the patient (Sp) or the quality of the service (Sq).
The health system is complex and like other complex systems it is fundamental to apply HRA methodologies to reduce the risk not only for the patient, but mainly for the patient. The HRA methodology mhFMEA proposed for a health care service was developed in an Operating Room of one of the main Hospitals in Portugal, subject to factors that can affect the human performance (PSFs) allowed: To determine the impact of each PSF, taking into account the teams of health professionals in the service and determine the influence of it on each failure mode; To determine the probability of occurrence (O) of the failure modes (human errors); To determine the consequences of each failure mode for the patient (Sp) or quality of the service (Sq) as well as the possibility of avoiding (A) each failure mode; The calculation of HERAp and HERAq and the risk classification of each failure mode for the patient and for the quality of service for subsequent prioritization and application of corrective measures.
The failure mode (human error) that was initially considered as unacceptable in HERAp is related to pre-operating conditions and specifically by “Anaphylactic reaction/ignorance of known allergy in the patient” (FM8). For HERAq were considered as unacceptable the “Patient without signed informed consent” (FM1), “The nursing team did not confirm the sterilization” (FM24), “Medication error due to non-compliance with the pre-anesthetic drug regimen” (FM30), “Transmission of pathogenic microorganisms through the use of damaged or poorly disinfected nasolaryngoscopes” (FM54) and “Poor labeling or loss of products for analysis - diagnostic errors” (FM58).
The application of corrective measures after prioritizing the failure modes taking into account the assessment of the probability of failure (O) allowed the minimization or mitigation of failure modes with higher risk, with the calculation of a new impact of PSFs and consequently a new probability of occurrence (O) of each failure mode.
In this way, it is possible to reduce the risk for the patient and improve the quality of the service provided, and thus contributing to a higher patient safety and a higher quality in providing a health care, with the inclusion of the PSFs. The proposed methodology can be adapted to any health care service where the goal is to assure safety and quality.
The main limitation of the methodology is related to the fact that the determination of the probability of occurrence of each failure mode (human error) is based on the answers given by persons and thus with the possibility that they may be biased according to specific interests or objectives. It is not easy to overcome this issue, but the establishment of a practice of factual records that allow removing some subjectivity from the answers to the questionnaires could be an important step towards a greater credibility of the results achieved.
As future work, and although the mhFMEA methodology is already automated in a spreadsheet, the development of a more synthesized, intuitive and easy-to-use application (App) by health professionals in a health care service would be an important tool for each team leader of health professionals allowing to apply it and improve safety and the quality of the service by changing the identified PSFs.
Footnotes
Acknowledgements
The authors wish to thank the study participants for their contribution to the research.
Conflict of interest
None to report.
Ethical approval
This study was approved by the Clinical Research Centre of Lisbon University Hospital Center (Centro Hospitalar de Lisboa Central EPE) - Health Ethics Committee (CES 940/2020).
Funding
None to report.