
Abstract
BACKGROUND:
Renal transplant patients receive several drugs concomitantly.
OBJECTIVE:
Limited literature exists evaluating the drug use in this population that is at high risk for drug-induced acute kidney injury and complications due to under-or over-dosage of immunosuppressant drugs due to drug–drug interactions.
METHODS:
A retrospective observational study was carried out in 269 renal transplant patients in whom either oral or parenteral drugs were evaluated. World Health Organization (WHO) indicators of drug utilization such as the average number of drugs prescribed, daily defined dose, and proportion of drugs listed as WHO essential drugs were evaluated. Details on the drugs with nephrotoxic potential were obtained. Drug–drug interactions were assessed concerning the severity (major, moderate, and minor) as well as type (pharmacokinetic, pharmacodynamic, and toxicity).
RESULTS:
One-hundred and ninety-eight drugs were administered to the study participants. The median (range) total number of drugs received by the study participants was 23 (6–55). The proportion of drugs listed in the WHO essential drug database was 57.1 (16.7–100)%. Forty-six drugs with potential nephrotoxicity and seven drugs that were contra-indicated in patients with chronic renal disease/end-stage renal disease were administered to the study participants. The mean (SD) numbers of drug interactions observed amongst the study participants were 18.4 (10.1). Age (β: 0.2, 95% CI: 0.1, 0.3) and duration of renal transplantation (β: −0.3, 95% CI: −0.5, −0.1) were the significant predictors of drug burden. A total of 645 drug interactions were identified amongst the study participants (major – 240; moderate – 270; and minor – 135) of which the majority were pharmacokinetic followed by toxicity risk. Age was significantly associated with the risk of potential drug interaction (OR: 2.6, 95% CI: 1.8, 12.4; p = 0.001).
CONCLUSION:
Drug treatment in renal transplant patients poses a significant burden in terms of nephrotoxicity potential and drug–drug interactions. A dedicated ambulatory clinical pharmacy service monitoring the drug use coupled with drug deprescribing strategies are the need of the hour in this population.
Introduction
Patients who have undergone renal transplantation have a significant burden of consuming several drugs every day, predominantly immunosuppressant drugs [1]. Renal transplant patients require lifelong therapy of immunosuppressives, and drugs for treating hypertension and diabetes [2]. Polypharmacy is rampant in patients with renal transplantation and is a major contributor to medication non-compliance, which is reported in 45.5% of cadaveric renal transplantation and 28.6% from living donors [3]. Renal transplant patients are vulnerable to adverse events owing to drug–drug interactions and narrow therapeutic indices of immunosuppressants [4]. On average 5.6 drug interactions were observed per patient with renal transplantation and one-tenth of hospital admissions have been attributed to such adverse events [5]. Several drugs get eliminated predominantly by kidneys either directly, or as metabolites (from the liver). Drugs with nephrotoxic potential increase the risk of acute kidney injury, and failure of the transplanted kidneys. The most common underlying etiology of renal transplantation is end-stage renal failure caused by systemic hypertension and diabetes [6]. A recent estimate from the United States revealed that nearly 72% of adults with chronic kidney disease received at least one nephrotoxic drug of which 47.2% were prescribed one and 52.8% at least 2 [7]. A recent study in 1730 adult renal transplant patients revealed at least one NSAID prescription of whom 13% developed acute kidney injury and 5% developed hyperkalemia [8]. The quality of life of renal transplant patients is influenced by the administered drugs [9]. Against this backdrop, we carried out the present study to evaluate drug use in our renal transplant patients.
Methods
Study ethics and design
This retrospective observational study was carried out at the Department of Nephrology, Salmaniya Medical Complex, Kingdom of Bahrain between May and August 2021. Ethical approval was obtained from the Institutional Ethics Committee from the College of Medicine and Medical Sciences, Arabian Gulf University (E05-PI-5/21) and Salmaniya Medical Complex (73120521).
Study procedure
Patients who underwent renal transplantation and were followed up in the Nephrology Department were recruited. Those without drug-related details were excluded. Only those drugs administered either orally or parenteral route were considered. The following details were obtained for each study participant: demographic characteristics (age and sex), date of renal transplantation, diagnoses, serum immunosuppressant levels, and their drug-related details. World Health Organization (WHO) indicators of drug utilization such as the average number of drugs prescribed, daily defined dose, and proportion of drugs prescribed from the WHO essential drug list will be evaluated [10]. Drugs with potential nephrotoxicity and drugs contraindicated in patients with chronic renal disease and end-stage renal failure as listed in the recent literature was taken as reference points [11]. The prescribed drug was considered as fixed-dose combinations (FDC) when two or more active ingredients remain as a single dosage formulation. Potential drug interactions were evaluated using the Drugs.com ® database that includes the details from IBM Watson Micromedex®, Cerner Multum®, and American Society of Health-System Pharmacists® [12]. Only the drug–drug interactions were evaluated and were classified into one of the following types: pharmacokinetics – when the concomitant drug influences the drug absorption or changes the blood levels of the drug or inhibits the metabolizing enzymes or renal excretion; pharmacodynamics – when concomitant drug influences the therapeutic effect of the drug; and toxicity when there was an increased risk of adverse events. Descriptive statistics were used for representing the demographic variables. Linear regression analysis was carried out for identifying the factors associated with drug burden with the following independent variables: age, sex, and duration of renal transplantation. Beta coefficient (β) was used for representing the unit change in the drug burden with 95% confidence intervals (95% CI). Similarly, logistic regression was carried out with the above-mentioned dependent variables with the risk of potential drug interactions. Odds ratio (OR) with 95% CI was used as the effect estimate in logistic regression. A p-value of ≤0.05 was considered significant. SPSS version 26.0 for Windows (IBM Corp., Armonk, NY, USA) was used for statistical analysis.
Results
Demographics
Two hundred and sixty-nine patients were recruited, and their demographic characteristics are represented in Table 1.
Summary of demographic characteristics of the study participants (N = 269)
Summary of demographic characteristics of the study participants (N = 269)
The values are mentioned in median (range) unless specified; BPH – Benign prostatic hyperplasia; others include systemic lupus erythematosus, epilepsy, migraine, stroke, atrial fibrillation, peripheral vascular disease, ischemic heart disease, discoid lupus erythematosus, multiple sclerosis, and bronchial asthma.
One-hundred and ninety-eight drugs were administered to the study participants. One-hundred and seventy-eight (89.9%) were administered orally, 18 (9.1%) were administered parenterally, and two (1%) drugs were administered in both oral and parenteral formulations. The median (range) total number of drugs received by the study participants was 23 (6–55). The details of the drugs, doses administered per day, and cumulative doses are represented in Electronic Supplementary Table 1. Linear regression analysis identified age (β: 0.2, 95% CI: 0.1, 0.3) and duration of renal transplantation (β: −0.3, 95% CI: −0.5, −0.1) as significant (p = 0.004 and 0.003, respectively) predictors. The proportion of drugs listed in the WHO essential drug database was 57.1 (16.7–100)%.
Drugs with potential nephrotoxicity and contra-indicated drugs
Forty-six drugs with potential nephrotoxicity were administered to the study participants. The median, lower and upper ranges of the daily doses and cumulative doses upon DDDs are depicted in Figs 1 and 2. The median ratios for the daily, and cumulative dose ratios were 0.85, and 20.2, respectively.
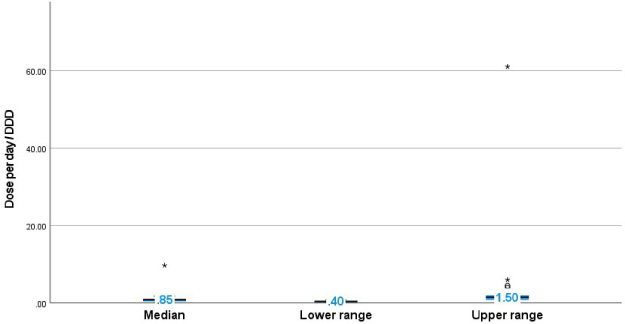
Daily dose/DDD of the drugs administered in the study population. The boxplot depicts the median, lower and upper ranges of the daily dose/DDD ratios.
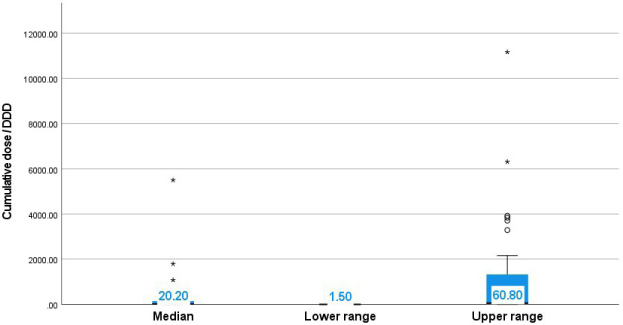
Cumulative doses/DDD amongst the study population. The boxplot depicts the median, lower and upper ranges of the cumulative dose/DDD ratios.
Seven drugs that were contraindicated in patients with chronic renal disease/end-stage renal disease were observed to be administered in the study participants. The details on their doses and ratios of doses/DDDs are represented in Table 2.
Contra-indicated drugs administered in the study participants
NA – DDDs are not available.
Sixteen drugs were administered as FDCs of which amoxicillin/clavulanic acid, paracetamol/orphenadrine, and sulfamethoxazole/trimethoprim formed the majority (Fig. 3).
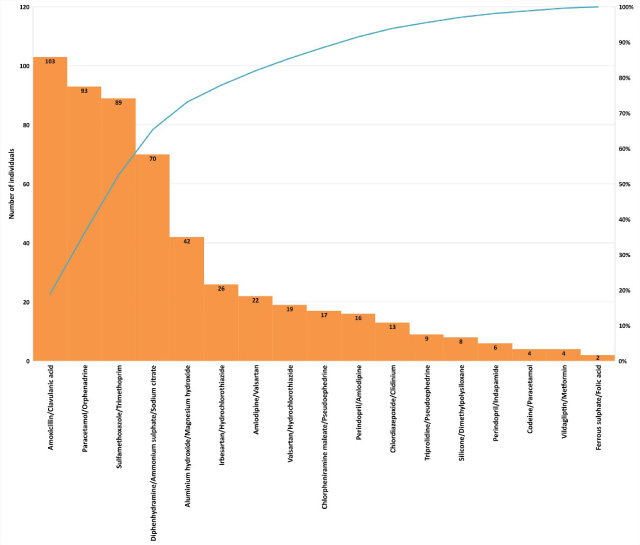
Fixed dose combinations administered in the study participants. This Pareto chart represents the distribution of drugs administered as fixed dose combinations.
A total of 645 drug interactions were identified amongst the study participants (major – 240; moderate – 270; and minor – 135). Most of the interactions were moderate in severity and were pharmacokinetic followed by an increased risk of adverse events (Fig. 4). The mean (SD) numbers of drug interactions observed amongst the study participants were 18.4 (10.1). Age was the only significant variable associated with the risk of potential drug interaction (OR: 2.6, 95% CI: 1.8, 12.4; p = 0.001).
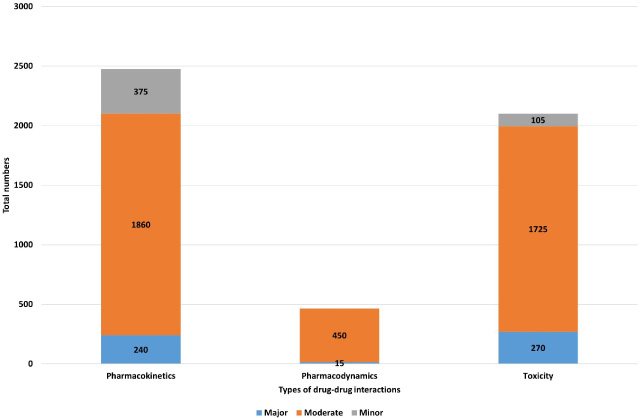
Types of drug–drug interactions identified amongst the study participants. The stacked bar chart represents the numbers of each type and severity states of drug–drug interactions.
We evaluated 269 patients with renal transplantation to understand the drug burden in this vulnerable population. We observed that a significant number of potentially nephrotoxic drugs and drugs contra-indicated in patients with chronic renal failure were administered to the study participants. All the study participants received drugs that could be involved in drug–drug interactions. Most of the identified interactions were moderate in severity and pharmacokinetic in nature. Age and duration of renal transplantation were significantly associated with drug burden and age was the significant factor determining the risk of potential drug interaction.
Nephrotoxic drugs are an important factor resulting in acute kidney injury amongst the in-patients to an extent of around 25% [13]. Episodes of acute kidney injury in renal transplant patients have been shown to negatively impact the graft function with a mortality of 2.1% [14]. We observed that in general, the drugs were administered at far lower doses than their DDDs in our population. Non-steroidal drugs (NSAIDs) formed a large majority of the drugs that are contraindicated in this population. A European study revealed that 63% of patients with renal transplantation admitted taking any of the NSAIDs of which nearly one-fifth of them consume several times a week and 4% daily [15]. A week of NSAID therapy was observed with a 5% increase in the risk of acute kidney injury, while chronic administration was shown to increase the risk to nearly 3.25 times in renal transplant patients [16]. The authors in that study observed that ibuprofen followed by naproxen were the most common NSAIDs resulting in acute kidney injury and relatively lower risks were observed with sulindac, diflunisal, and ketorolac. We observed a considerable number of patients in our study receiving ibuprofen/naproxen while none with those attributed with lower nephrotoxicity risk. NSAID use is inevitable in patients with chronic kidney disease as well as in patients with renal transplantation (particularly with sub-optimal renal clearance) as around two-thirds of the population suffer moderate or severe pain [17]. Alternative pain killers include opioids, but they are associated with an increased risk of central nervous system toxicities and a study from chronic kidney disease patients revealed a higher mortality risk with opioids compared to NSAIDs [18]. NSAIDs also exhibit dose-dependent nephrotoxicity and only higher dosages were observed to result in AKI [16]. Considering the present evidence, it may be prudent to use NSAIDs with low nephrotoxic potential (such as sulindac, diflunisal, and ketorolac) particularly at lower doses in renal transplant patients.
We identified a significant burden of drug–drug interactions in the study participants. This is comparable to a previous estimate that showed a prevalence of severe interactions in 88% of renal transplant patients [19]. Also, most of the interactions were related to alterations in the pharmacokinetics like the populations receiving anticancer drugs, or antimicrobial drugs for treating human immunodeficiency virus [20,21]. Immunosuppressants are the major drug class received by renal transplant patients and serial therapeutic drug monitoring is required for maintaining optimal therapeutic response. The altered pharmacokinetics can result either in under-or over-immunosuppression that is associated with lethal consequences. The fact that most of the drug–drug interactions alter the pharmacokinetics re-emphasizes the need for frequent therapeutic drug monitoring and adverse drug reactions. Additionally, personalizing the administration of immunosuppressants according to the influencing polymorphisms shall facilitate the optimization of therapy in this population [22]. This calls for establishing a dedicated group of pharmacists with allied health care professionals in intensely following up those with red flags on the drug interactions. It is the need of the hour to implement ambulatory clinical pharmacy service for renal transplant patients [23]. Polypharmacy is one of the main factors leading to drug–drug interactions and a recent study estimated that nearly 41% of renal transplant patients were receiving 10 or more medications [24]. Similarly, elderly patients were identified to have a significant risk for drug interactions and polypharmacy in the present study that corroborates with previous reports [25,26]. Similarly, we also observed that the drug burden is more during the early years following renal transplantation. Marienne et al. [27] evaluated the complexity of medication regimen in renal transplants and observed that 42% received 10 or more drugs at the time of renal transplantation, while 38% at the end of one year. We did not evaluate and compare the drug–drug interactions from other databases such as Lexicomp®. Neither we evaluated the occurrence of either adverse drug reactions or rejection episodes or serum levels of immunosuppressant drugs. A recent study evaluating clinically relevant drug–drug interactions for immunosuppressive drugs revealed that it could vary between 4 and 8% depending on the databases used [4]. Hence, there is a need for developing a consensus on the deprescription strategy in patients with renal transplantation based on parameters such as the levels of immune response, post-transplant renal function, lipid profile and other key blood parameters, and untoward adverse events following drug administration.
Conclusion
Drug treatment in renal transplant patients poses a significant burden in terms of nephrotoxicity potential and drug–drug interactions. A dedicated ambulatory clinical pharmacy service monitoring the drug use and strategies for drug deprescription are the need of the hour in this population.
Ethics statement
The study was approved by the Institutional Ethics Committee from College of Medicine and Medical Sciences, Arabian Gulf University (E05-PI-5/21) and Salmaniya Medical Complex (73120521).
Conflict of interest
None to report.
Data availability statement
The data is available from the corresponding author upon reasonable request.
Funding
None to report.