
Abstract
BACKGROUND:
Acinetobacter baumannii is a major cause of nosocomial infections and high mortality rates. Evaluation of risk factors for such resistant infections may aid surveillance and diagnostic initiatives, as well as, can be crucial in early and appropriate antibiotic therapy.
OBJECTIVE:
To identify the risk factors in patients with resistant A. baumannii infection with respect to controls.
METHODS:
Prospective or retrospective cohort and case-control studies reporting the risk factors for resistant A. baumannii infection were collected through two data sources, MEDLINE/PubMed and OVID/Embase. Studies published in the English language were included while animal studies were excluded. The Newcastle-Ottawa Scale was used to assess the quality of studies. The odds ratio of developing antibiotic resistance in patients with A. baumannii infection was pooled using a random-effect model.
RESULTS:
The results are based on 38 studies with 60878 participants (6394 cases and 54484 controls). A total of 28, 14, 25, and 11 risk factors were identified for multi-drug resistant (MDRAB), extensive-drug resistant (XDRAB), carbapenem-resistant (CRAB) and imipenem resistant A. baumannii infection (IRAB), respectively. In the MDRAB infection group, exposure to carbapenem (OR 5.51; 95% CI: 3.88–7.81) and tracheostomy (OR 5.01; 95% CI: 2.12–11.84) were identified with maximal pool odd’s ratio. While previous use of amikacin (OR 4.94; 95% CI: 1.89–12.90) and exposure to carbapenem (OR 4.91; 95% CI: 2.65–9.10) were the foremost factors associated with developing CRAB infection. Further analysis revealed, mechanical ventilation (OR 7.21; 95% CI: 3.79–13.71) and ICU stay (OR 5.88; 95% CI: 3.27–10.57) as the most significant factors for XDRAB infection.
CONCLUSION:
The exposure of carbapenem, amikacin (previous) and mechanical ventilation were the most significant risk factors for multidrug, extensive-drug, and carbapenem resistance in patients with A. baumannii infection respectively. These findings may guide to control and prevent resistant infections by identifying the patients at higher risk of developing resistance.
Introduction
Acinetobacter baumannii is an aerobic non-fermenting gram-negative coccobacillus that has been reported as a prominent nosocomial pathogen with enhanced environmental resilience and a propensity to develop resistance to commonly prescribed antimicrobials [1]. Of all Acinetobacter species, A. baumannii is the most important member associated with infections in clinical practice and causes most of the reported outbreaks [2]. A. baumannii can cause infections in the blood, urinary tract, and lungs (pneumonia), as well as infections in other body wounds. It can also “colonise” or live in a patient without infecting them or creating symptoms, especially in respiratory secretions (sputum) or open wounds [3].
A. baumannii infection does not always act as an infecting pathogen due to its extensive distribution and colonisation capabilities [4,5]. Furthermore, the epidemiologic pattern of AB acquisition and dissemination appears to be distinct from that of other non-fermentative, gram-negative bacteria [5].
The emergence and spread of Acinetobacter species and its high resistance to most antibiotics available in clinical practice is an area of great concern [6]. A number of resistance mechanisms to many classes of antibiotics are known to exist in A. baumannii, including β-lactamases, multidrug efflux pumps, aminoglycoside-modifying enzymes, permeability defects, and the alteration of target sites [7–10]. In the case of carbapenem resistance, the mechanisms like beta-lactamases along with the carbapenem-hydrolysing activity including carbapenem-hydrolysing class D beta lactamases (CHDLs) and metallo-beta-lactamases (MBLs) are considered as major mechanisms [11]. Furthermore, A. baumannii appears to have a high propensity for developing antibiotic resistance [12]. The number of imipenem resistant A. baumannii strains has been continuously increasing in recent years, and these isolates are frequently multidrug-resistant [13–15].
These resistant infections often occur in older patients, many of whom have chronic underlying diseases and have previously received antimicrobial treatment [16]. In places with endemic colonization or epidemic outbreaks of infection, risk factors may differ [5,17].
Multiple studies have examined the risk variables for a resistant A. baumannii infection; however, the results have varied. Therefore, pooling of the data through meta-analysis is expected to provide concrete evidence in order to prevent infection and to optimize therapy, as well as identifying sources of diversity across various types of studies. Therefore, this study aimed to identify the risk factors in patients with resistant Acinetobacter baumannii infection with respect to controls.
Materials and methods
This systematic review and meta-analysis was conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) checklist [18–20]. A protocol for this review was developed and registered in the PROSPERO database (CRD42022299349) [21].
Literature search
A systematic electronic search was conducted in PubMed/MEDLINE and OVID databases for citations indexed from the year 2000 to 2021. The search strategy was developed as per the Cochrane checklist of developing a search strategy [22,23]. The MeSH terms used were “Risk Factors”, “Acinetobacter baumannii”, “Drug Resistance”, “Drug Resistance, Bacterial”, “Acinetobacter baumannii infections”, “Hospitals, public”, “Hospitals, private”, “Hospitals, teaching”, “Intensive Care Units”, “Hospital units”. The full PubMed/MEDLINE search strategy is listed in Supplementary Material S1. Filters as observational studies, humans, English, and journal articles were used. In order to maximise the inclusion of relevant data, these searches were expanded by reviewing the reference lists of qualifying studies in an iterative process.
Eligibility criteria
This systematic review and meta-analysis explores the potential risk factors for developing resistant A. baumannii infection in hospitalized patients. Prospective or retrospective observational, cohort and case-control studies were eligible for inclusion which reported the data on risk factors associated with the acquisition of resistant A. baumannii infection. This research excluded interventional study designs and non-comparative observational studies, case reports, and case series.
Studies examining patients with either hospital-acquired or community-acquired infections were included, provided that those patients were evaluated in a hospital/inpatient setting. The studies of mixed infections and studies that involving animal models were excluded. Studies published as full texts in the English language since the year 2000 was considered.
Study definitions
The primary objective of this study was to examine studies evaluating risk factors/predictors in patients with resistant A. baumannii infection evaluated in the hospital setting. In this study, the hospital setting comprises all types of units, including intensive care units (ICUs), casualties, or other wards in which patients were admitted at the time of collection of resistant A. baumannii microbiological specimen and undergone further treatment in a hospital setting. For a pathogen to be considered multidrug-resistant (MDR), it must be resistant to at least one agent across at least three classes of antimicrobials. The term “extensively drug-resistant” (XDR) refers to infections that are resistant to many drugs yet still susceptible to only two or fewer classes of antibiotics. If a drug susceptibility test shows negative for at least one antibiotic, then the microorganism is considered drug sensitive (DS). However, this study accepted certain considerable variation in the definitions of the individual studies. This study considered cases as multidrug-resistant, extensive drug-resistant, or carbapenem/imipenem-resistant Acinetobacter baumannii and controls as susceptible to A. baumannii infection or no infection.
Study selection
Papers were managed using EndNote software and all citations identified by literature searches were independently screened by two researchers. In primary screening titles and abstracts were screened and full-text articles were screened in secondary screening. During the screening, conflicts were adjudicated through group discussions.
Data extraction
A single reviewer performed data extraction and risk of bias assessment. The extraction was reviewed and confirmed by at least one other reviewer. Any disagreements were resolved by a group discussion among the study team. All data was extracted into a customized Microsoft Excel sheet.
General study characteristics were extracted, including first author, study design, enrolment period, countries, and setting. The sample size of the case and control, male and female, mean/median age along with standard deviation/range were extracted in population characteristics. Potential risk factors along with their odds ratio were extracted only if at least three studies examined them and those studies reported the numbers of individuals in each comparison group.
Quality assessment
This study assessed the methodological quality of each study on predefined criteria using the New-castle Ottawa risk of bias tool which probes the risk of selection, performance, detection, attrition, reporting, and other potential biases. The NOS (Newcastle-Ottawa Scale) assessed the quality of each study based on three-dimensional criteria and included (i) selection of population (4 points), (ii) comparability of groups (2 points), and (iii) outcome/exposure of interest (3 points). The quality of studies was identified with the scores in which a score from 7–9 indicated high quality, 4–6 indicated intermediate quality and 0–3 a very high risk of bias [24].
Statistical analysis
The meta-analysis were performed using RevMan 5.4 software provided by the Cochrane collaborations [25]. The odds ratio and associated 95% confidence interval of developing antibiotic resistance in patients with A. baumannii infection were pooled. Statistical heterogeneity among studies was assessed using the I 2 value in which I 2 > 50% was considered the evidence of heterogeneity [26]. Depending upon the I 2 value, the Mantel–Haenszel fixed or random effect models were used to pool the final evidence. Forest plots of each risk factor were synthesized to summarize the evidence.
Possible publication bias was quantitatively ruled out using Egger’s test and funnel plots which were produced in Comprehensive Meta-Analysis (CMA) software. Further the results were considered statistically significant if P-value was less than 0.05 [27]. The sensitivity analysis was performed by omitting studies one by one on each risk factor to identify the source of heterogeneity [26,28].
Results
Study selection
The literature search identified 1325 citations from electronic databases. After removing duplicates, 996 titles and abstracts were eligible for primary screening. Using a low threshold of eligibility criteria for review of titles and abstracts, 87 full-text articles were retrieved. Following a full-text review, 38 [12,14,29–64] articles were included for meta-analysis based on the eligibility criteria. The PRISMA diagram of this study is presented in Fig. 1. Out of the 38 eligible articles, 19 articles examined multi-drug resitant A. baumannii infection (MDRAB), and the remaining 19 articles examined carbapenem/imipenem (CRAB/IRAB) and extensive drug resistant A. baumannii infection (XDRAB).
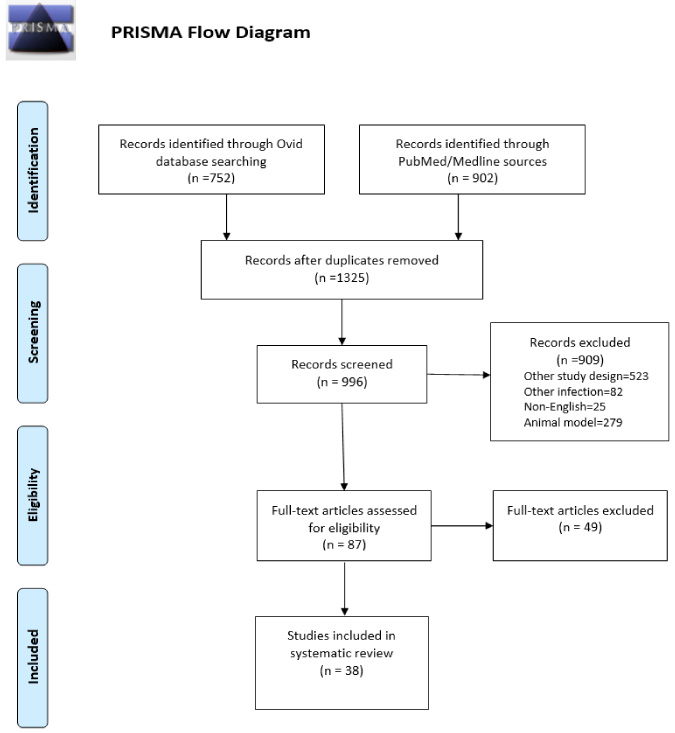
PRISMA flow diagram.
The main characteristics of included studies are represented in Table 1. The studies published from 2000-2021 included 60878 participants, of whom 6394 had resistant A. baumannii infection and 54484 were the control group with susceptible A. baumannii infections or no infections. 13 studies were conducted in China followed by 6 from the USA. The study designs in 38 articles were case-control [13], retrospective study [12], prospective cohort [8], and retrospective cohort [5]. The case and control groups were matched in 4 studies. In 31 studies the samples were selected from a single setting while in 7 studies samples were selected from multi-centre settings.
Population characteristics of the studies
Population characteristics of the studies
∗Sub-studies with different group of participants.
The quality of all included studies was determined by NOS assessment. Out of total studies, 25 studies were of high quality and 13 were of moderate quality. None of the studies had a high risk of bias (Table 1). Sensitivity analysis by the exclusion of one study at a time showed that there were only minor changes in the quantitative pooled odd’s ratio and 95% confidence interval. No evidence of publication bias was detected according to Egger’s test and funnel plot. Sensitivity analysis and funnel plots are presented in Supplementary Materials S2–S5.
Main results
Risk factors for Multi-drug resitant A. baumannii infection (MDRAB) infection relative to control patients
In the case of MDRAB infection, a total of 28 risk factors were identified (Table 2). All identified risk factors were dichotomous variables. The maximal pooled odd’s ratio was seen in exposure of carbapenems [OR 5.51, 95% CI 3.88–7.80, p < 0.001], followed by tracheostomy [OR 5.01, 95% CI 2.12–11.84, p < 0.001] and urinary catheter [OR 4.57, 95% CI 2.49–8.41, p < 0.001].
Risk factors for MDR A. baumannii infection relative to control patients
Risk factors for MDR A. baumannii infection relative to control patients
Of the 28 risk factors, 19 statistically significant risk factors were - mechanical ventilation, exposure to carbapenem, tracheostomy, urinary catheter, ICU stay, exposure to aminoglycosides, exposure to fluoroquinolone, malignancy, exposure to quinolones, central venous catheter, exposure of vancomycin, respiratory disease, exposure of third generation cephalosporins, hospitalization, cancer, cardiovascular disease, previous use of antibiotics, exposure of piperacillin-tazobactam and surgery. The forest plots presenting the risk factors with pooled odd’s ratio are given in Supplementary Material S2.
A total of 22 risk factors were identified for CRAB infection, that are represented in Table 3. Of these, the uppermost risk factors were previous use of amikacin [OR 4.94, 95% CI 1.89–12.9, p < 0.001], previous use of carbapenem [OR 4.91, 95% CI 2.65–9.1, p < 0.001] and pneumonia [OR 4.71, 95% CI 2.03–10.93, p < 0.001].
Risk factors for Carbapenem-resistant A. baumannii infection relative to control patients
Risk factors for Carbapenem-resistant A. baumannii infection relative to control patients
Of the 22 risk factors, 9 statistically significant were- previous use of amikacin, previous use of carbapenems, pneumonia, mechanical ventilation, previous use of piperacillin-tazobactam, catheter-related infection, central venous catheter, urinary catheter, and ICU stay. Supplementary Material S3 contains forest plots depicting risk factors with pooled odd’s ratio.
A total of 11 risk factors in which only male as a risk factor is statistically insignificant (Table 4). The statistically significant risk factors were exposure to aminoglycosides, arterial catheter, ICU stay, exposure to carbapenems, surgery, central venous catheter, mechanical ventilation, parenteral nutrition, nasogastric tube, and malignancy.
Risk factors for Imipenem resistant A. baumannii infection relative to control patients
Risk factors for Imipenem resistant A. baumannii infection relative to control patients
Risk factors for XDR A. baumannii infection relative to control patients
ICU stay [OR 3.51, 95% CI 1.18–10.49, p = 0.02], carbapenem exposure [OR 2.94, 95% CI 1.76–4.92, p < 0.001] and surgery [OR 2.9, 95% CI 1.79–4.69, p < 0.001] were the foremost factors associated with developing IRAB infection. The forest plots of risk factors with quantitative pooled odd’s ratio are included in Supplementary Material S4.
Mechanical ventilation [OR 7.21, 95% CI 3.79–13.71, p < 0.001], ICU stay [OR 5.88, 95% CI 3.27–10.57, p = 0.52] and bedridden [OR 4.18, 95% CI 2.09–8.38, p < 0.001] were the highest-ranking significant risk factors for XDRAB infection (Table 5).
Seven risk factors were statistically significant from a total of 14 risk factors: Mechanical ventilation, bedridden, central venous catheter, urinary catheter, surgery, malignancy, and chemotherapy. The forest plots of all 14 risk factors for XDRAB infection are presented in Supplementary Material S5.
Discussion
Acinetobacter baumannii is a common cause of nosocomial infection and is being investigated as one of the leading causes of the antibiotic resistance crisis [65]. According to the World Health Organization (WHO), A. baumannii is one of the most threatening of the ESKAPE organisms (Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter species) that are resistant to antibacterial treatments. When compared to other non-baumannii species, the resistant species is linked to a higher mortality rate among infected patients [66,67]. A. baumannii can cause a wide range of infections, the majority of which affect the respiratory tract, particularly ventilator-associated pneumonia, bacteremia, and skin wound infections [68]. The Centers for Disease Control and Prevention (CDC) also reported that the majority of clinically relevant A. baumannii strains are multidrug-resistant, accounting for up to 20% of infections in intensive care units (ICUs) and 7% of infections in patients who are physically attached to medical equipment (5). Resistant A. baumannii infections are highly prevalent in the nations, where the studies included in this review were performed. China, the United States, Turkey, Brazil, Greece, Spain, France, Thailand, Egypt, Germany, and Israel are among these countries [69]. Even though there has been research that has investigated risk factors for resistant A. baumannii infection and has come to bifurcated and conflicting conclusions. For example, a total of 83 percent of controls and 95 percent of patients exposed to the cephalosporins acquired MDRAB infection, according to Huang et al. [51] while Zhou et al. reported that patients with MDRAB infection had a higher exposure ratio of cephalosporins (21 percent controls vs. 14 percent of cases) [55]. In yet another example, Dent et al. [43] reported that 78.5% of controls and 90.9% of patients exposed to the antibiotics developed MDRAB infection. In contrast, in a similar study [51], a higher exposure ratio was observed among patients with MDRAB infection (86.6% controls vs. 89.2% of cases).
Some of the included studies [53,57,62] have published risk profiles in large sample sizes, while other studies [14,35,58] have concluded results based on small size. Therefore, this discrepancy in results could be attributed to sample size differences and a general lack of statistical power.
Furthermore, some researchers are attempting to determine the risk factor for mixed infections, which commonly include resistant A. baumannii and Pseudomonas aeruginosa or combinations of ESKAPE organisms.
In this review, total of 38 studies in eleven countries involving several thousands of patients were meta-analysed by the reviewer. Data from all studies in which risk factors for the acquisition of antibiotic resistance in A. baumannii infections were extracted. The majority of the studies were evaluating the risk factor for acquisition of MDR followed by Carbapenem/imipenem resistance, and XDRAB infection. The control group in the majority of studies was susceptible to A. baumannii infection, while a fewer number of studies included patients with no infection as a control group. Consistent with the initial idea, the risk factor profiles differed between different antibiotic-resistant species. In the case of risk factors for developing multidrug-resistant A. baumannii infection, despite considerable heterogeneity in the definition of controls, this review accepted the definition given by the individual study.
The MDRAB has been a common cause of hospital outbreaks owing to its capacity to rapidly alter its genome and its ability to persist on inanimate surfaces and medical equipment with high disinfection resistance [70]. This review identified the following risk factors for developing multidrug resistance with pooled odd’s ratio greater than one: mechanical ventilation, exposure to carbapenem, tracheostomy, urinary catheter, ICU stays, exposure to aminoglycosides, exposure to fluoroquinolone, malignancy, exposure of quinolones, central venous catheter, exposure of vancomycin, respiratory disease, exposure of third-generation cephalosporins, hospitalization, exposure of cephalosporins, cancer, cardiovascular disease, previous use of antibiotics, exposure of piperacillin-tazobactam, total parenteral nutrition, the existence of comorbidity less than 2, exposure of fourth-generation cephalosporins, use of immunosuppressive agents, chronic obstructive pulmonary disease and diabetes mellitus. Whereas other risk factors like female gender, surgery, and comorbidity >2 were having odds ratio less than one. The increased likelihood of infection with MDRAB is provoked by these risk factors, which are mainly present in patients who have severe illness and greater susceptibility to infection, which leads to exposure to greater antibiotic selection pressure.
CRAB infection is associated with high healthcare costs, and significant mortality, causing worldwide concern, yet there are limited studies on examining the risk factors for its acquisition [71].
This review explored the following risk factors: previous use of Amikacin, previous use of carbapenems, pneumonia, mechanical ventilation, previous use of piperacillin-tazobactam, catheter-related infection, central venous catheter, urinary catheter, and ICU stay. Whereas risk factors like liver disease, previous use of beta-lactams/beta-lactamase inhibitors, previous use of aminoglycosides, and respiratory diseases as underlying health conditions were statistically insignificant protective factors. All these points indicate that antimicrobial stewardship for hospitalized patients should be reinforced.
Two systematic reviews, published in 2006 [72] and 2018 [73], have examined the risk profiles for carbapenem and extreme drug resistance in A. baumannii-infected patients. However, Lim et al. [73] only investigated antibiotic use as a risk factor, while Falagas et al. [72] only published a systematic review (no meta-analysis) of possible risk variables. There are no systematic reviews and meta-analyses published specifically for the risk factors for the acquisition of imipenem resistant as well as extended drug-resistant A. baumannii infection. In this study, a total of eleven risk factors met the eligibility criteria for IRAB. Among these risk factors, only the male gender was not statistically significant and its pooled odds ratio was less than one. The statistically significant risk factors found were exposure to aminoglycosides, arterial catheter, ICU stay, exposure to carbapenems, surgery, central venous catheter, mechanical ventilation, parenteral nutrition, nasogastric tube, and malignancy. The risk factors such as ICU stay and arterial catheter shows a high risk for the development of acquisition of IRAB infection. For XDRAB, among 14 eligible risk factors, seven were statistically significant which includes use of mechanical ventilation, bedridden, central venous catheter, urinary catheter, surgery, malignancy, and chemotherapy. On the other hand, pooled odds ratio of risk factors- ICU stays, liver disorder, end-stage renal disease, haemodialysis, diabetes, male gender and cerebral vascular diseases represented insignificant results.
The installation of mechanical ventilation and central venous catheter were the two risk factors that were common in all four examined groups since the majority of hospitalized ill patients have undergone the insertion of these two medical devices. Furthermore, use of central venous catheter, urinary catheter, ICU stay, surgery, diabetes mellitus, male gender, malignancy, carbapenem exposure, and aminoglycoside exposure were customary risk factors in at least one of the three groups evaluated. Additionally, it also indicates that medical device sterilization and decontamination will play an important role in preventing the acquisition of resistant infection.
Strengths and limitations
This review does not contain any studies of high risk of bias. The sensitivity analysis confirmed that the meta-analysed results were robust. The findings of the meta-analysis were interpreted with caution given that some potential risk factors were evaluated based on data from a small number of studies. Data for some risk factors showed significant heterogeneity across the studies.
This study contains the articles obtained from only two databases and articles other than English languages were excluded. All analysed data were dichotomous variables. The risk factors in univariate analysis were only included because risk factors in multivariate analysis were less and thereby cannot be pooled. The majority of the studies included were retrospective and all were observational which can increase the risk of selection bias, outcome reporting bias, and confounding. Nonetheless, all studies acquired NOS scores indicating high quality of studies and no obvious publication bias was observed for any of the factors. Risk factor profiling of antibiotic resistance should be further analyzed in large, well-controlled observational studies.
Conclusion
The exposure of carbapenem, amikacin (previous), and mechanical ventilation were the most significant risk factors for multidrug, extensive-drug, and carbapenem resistance in patients with A. baumannii infection respectively. These findings may assist to control and prevent resistant infections by identifying the patients at higher risk of developing resistance.
Footnotes
Acknowledgements
The authors thank the National Institute of Pharmaceutical Education and Research (NIPER), S.A.S. Nagar for making available the library, computer laboratory facility and online access of articles and other resources.
Conflict of interest
There are no conflicts of interest.