
Abstract
BACKGROUND:
In the recent decades, there has been an emerging population of people living with HIV/AIDS (PLWH) participating in vocational rehabilitation services to become gainfully employed.
OBJECTIVE:
The purpose of this study is to apply the Behavioral Model for Vulnerable Populations to gain a better understanding of (a) the characteristics of people living with HIV who reported use of vocational rehabilitation (VR) and/or American Job Centers (AJC), (b) factors that contribute to use of these services, and (c) the effects of use of federal employment services on access to care and reduced health-risk behaviors.
METHODS:
Survey research methods were used to collect data from a diverse sample of volunteer respondents.
RESULTS:
The majority of respondents were from low-income backgrounds and many had experienced significant barriers to employment such as homelessness, drug abuse, and incarceration. Chi-square tests of independence, factor analysis and structural equation modeling were used to address the research questions. The fit of the final structural equation model was good (RMSEA = 0.063, with 90% upper bound of 0.061, CFI = 0.95, TLI = 0.94). Overall, the findings indicate that the extent to which barriers to employment are experienced differs among those who used federal employment services and those who do not use either of these services.
CONCLUSION:
Although use of VR is associated with a reduction in health-risk behaviors, an important outcome associated with reduced onward HIV transmission, no such relationship was found with respect to use of AJC services. However, use of VR or AJC services was associated with increased access to care, indicating that both of these federal employment programs play an important role in achieving goals of the National HIV/AIDS Strategy.
Introduction
Emergent disabilities have been defined by either being newly identified within a population or having previously existed but rapidly increasing incidence within a particular geographical range or segment of the population (Koch & Rumrill, 2016). In the early 1980s, HIV/AIDS was characterized as an emergent disability when it was first recognized in the United States population. Over the years the demographic and geographic patterns of HIV prevalence have continued to change. Once thought of as a gay male disease, currently about a quarter of people living with HIV in the US are women who were exposed to HIV through heterosexual contact (CDC, May 2016). Furthermore, the epicenter of HIV has shifted from coastal urban centers to the South, which now accounts for 44% of all people living with HIV (CDC, March 2016). Due to advancements in medical treatment, HIV is also an emergent disability group within the population of people with disabilities who seek employment services.
In the early years, many people living with HIV (PLWH) did not seek vocational rehabilitation (VR) services because HIV/AIDS was widely viewed as a death sentence. However, since the 1996 introduction of highly active anti-retroviral therapy, which suppresses the replication of the HIV virus by combining 3 or more HIV medications from different classes of HIV drugs, there has been an emerging population of PLWH participating in VR services (Conyers, 2008; Hergenrather, Zeglin, Conyers, Misrok & Rhodes, 2016). Jung and Bellini (2009) examined rates of access and use of State VR programs by PLWH from 2002 to 2007 and found that “the rates of VR consumers with HIV to the estimated number of unemployed PLWH slightly increased over the years from 6.46% to 10.89% ” (p.3). Because the U.S. Department of Labor does not collect information on the disability status of consumers using their services, it is not possible to track rates of participation in their American Job Centers (formerly known as One Stop Career Centers) over time. VR, administered through the U.S. Department of Education (JAN, 2016), and AJC, administered by the U.S. Department of Labor (DOL, 2016), are the two primary employment services provided by the federal government. AJC are open to the public to access employment resources and supports and do not specialize in services for individuals with disabilities, although people with disabilities can use these services. VR services, on the other hand, are specifically designed to meet the needs of individuals with disabilities who must meet established eligibility requirements that are assessed by a rehabilitation counselor who is trained to assist people with disabilities gain employment (RSA, 2016). Additionally, within the VR system, vocational rehabilitation counselors have funds that they can expend to assist individual consumers to help reduce barriers to employment. Since there are no restrictions on access or eligibility to AJC, some people with disabilities will use both VR and AJC services in their pursuit of employment. With recent policy initiatives that encourage federal agencies to provide employment services to improve individual and public health outcomes, the rates of PLWH using vocational services will likely continue to rise.
In 2010, the White House Office of National AIDS Policy introduced the first U.S. National HIV/AIDS Strategy (NHAS) to help guide the nation’s efforts to address the domestic HIV epidemic by establishing a five-year plan outlining strategic priorities with measurable outcomes to (a) reduce new HIV infections, (b) increase access to care to improve health outcomes for PLWH, (c) reduce HIV-related health disparities, and (d) achieve a more coordinated national response to the HIV epidemic (White House Office of National AIDS Policy, 2010b). Notably, the 2010 National HIV/AIDS Strategy Federal Implementation Plan specifically directs federal agencies to “consider ways to increase supports for employers to hire and maintain employment of people with HIV and how to integrate them in broader employment initiatives for people with disabilities” (p. 25).
This increased focus on vocational services in HIV public health policy is part of a larger trend to place a greater emphasis on examining the social determinants of health to complement more traditional HIV prevention efforts that had been primarily focused on changing individual behaviors. The Centers for Disease Control and Prevention’s National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention (2010) published a White Paper on the Social Determinants of Health that highlights the need to focus on “interpersonal, network, community and societal influences of disease transmission and health,” (p. 1) including developing comprehensive interventions that address “where we live, work, learn and play” (p. 1). This policy shift is also reflected in the updated NHAS (White House Office of National AIDS Policy, 2015), which details a revised five-year plan through 2020 that places a significant emphasis on the need to address key social determinants of health by strengthening integration of services and linking PLWH to basic services including employment.
Advances in HIV treatment and research have demonstrated that adherence to antiretroviral therapy reduces the levels of HIV virus in the body, which not only improves individual health outcomes but also dramatically reduces the risk of transmitting HIV to others (Gardner, McLees, Steiner, Rio & Burman, 2011). However, linking and retaining PLWH into care is a significant challenge to public health. The most recent national data indicate that of all of the people living with HIV in the United States, only 40% were engaged in HIV medical care and just 30% achieve the optimal goal of viral suppression (Bradley et al., 2014). In light of the fact that medical advancements alone have not been able to end the HIV/AIDS epidemic despite their efficacy, examining social determinants of health such as the provision of employment services is a new and important area of research.
Key research findings support the individual and public health benefits of employment and vocational services for PLWH (Nachega et al., 2015; Richardson et al., 2013; Richardson, Wood, Li & Kerr, 2010; Rueda et al., 2011, 2012). No research, however, has examined the relative impact of different types of employment services on supporting the goals of the NHAS. One study, framed within the Andersen Model of Health Care Utilization, specifically investigated the impact of the use of VR services on outcomes associated with the NHAS and found that use of VR services had a significant direct effect on reducing health risk behaviors, increasing access to care, and increasing use of supplemental vocational services (Conyers & Boomer, 2014). Because other employment service options for PLWH including private rehabilitation services, non-profit VR services and HIV-specific employment services are extremely limited due to lack of funding, the purpose of this study is to compare the impact of the use of VR to the use of AJC on achieving key public health outcomes: increasing access to care and reducing health-risk behaviors. Consistent with our previous study that examined the impact of VR services on supplemental employment services, health-risk behaviors and access to care, the current study is framed within the Behavioral Model of Vulnerable Populations (BMVP; Gelberg, Andersen & Leake, 2000), which expands Andersen’s Behavioral Model of Health Care Utilization (Andersen, 1995). Job confidence, health perception and reduced HIV stigma have all been identified as enabling factors that can contribute to the use of VR (Conyers, 2011) but no research has examined if these enabling factors would also contribute to the use of AJC. Given the changing demographics and health potential of PLWH it is essential to have a better understanding of the public health benefits of the different federal employment services that could help to contribute to achieving the goals of the NHAS. To address this need, the three research questions are (a) what are the characteristics of PLWH who use VR or AJC services? (b) What is the relationship among factors that contribute to VR use and AJC use? And, (c) What are the separate effects of VR use and AJC use on access to health care and reduced health-risk? Although both VR and AJC use are hypothesized to have an impact on public health outcomes, use of VR is hypothesized to have a stronger association with public health outcomes than the use of AJC because of the more intensive nature of VR services.
Method
Participants and instrument
This study used structural equation modeling to analyze a subset of data from the National Working Positive Vocational Development and Employment Needs Survey Study (NWPC-VDES; Conyers, 2011). The original data set consisted of responses from 2,506 volunteer participants who were recruited from AIDS Service Organizations (ASO) and networks across the US to complete the NWPC-VDES. The survey took about 30–45 minutes to complete and covered content related to demographic variables, knowledge and use of vocational resources, employment status questions and HIV health-related subscales from the HIV Medical Outcomes Study (Wu, 1999). Selection criteria for the current study included participants who reported use of VR services, AJC services, or no use of federal employment services. The subset of data used for this study consisted of 1,984 participants from diverse racial (34% Black, 42% White, 17% Latino, 7% other), gender (66% male, 34% female) and sexual orientation (46% heterosexual, 46% gay, 8% bisexual) backgrounds. The mean age of the sample was 46. The majority of respondents were from low-income backgrounds (50% receive less than $15,000 per year) and many had experienced significant barriers to employment such as homelessness (53%), drug abuse (39%) and incarceration (33%). About a quarter of respondents reported never using the Internet or email. Within the sample, 25% had used VR services and 20% reported use of AJCs.
Data analysis
Chi-square tests of independence were conducted in SAS/STAT® software, v13.1 (Copyright 2013) to assess whether there is an association between the participant characteristics (such as race, income group, etc.) and the use of VR services and/or AJC services, or neither service. In the presence of a significant association, standardized Pearson residuals (ɛ*) greater than two were examined to explore the nature of the significant association (Agresti, 2007; Sharpe, 2015). Under the null hypothesis of no association between service use and a specific participant characteristic, the standardized Pearson residuals have an asymptotic standard normal distribution and thus values exceeding 2 represent deviations from the independence assumption for the corresponding cell in the table.
Structural equation modeling was conducted using Mplus v7 (Los Angeles, CA; Muthén & Muthén, 2012). An initial factor analysis identified the three exogenous latent factors of job confidence, health perception and reduced HIV stigma; items with factor loadings of λ= 0.3 or greater were retained. A structural equation model (SEM) combined the results from the factor analysis with probit and linear regressions to more fully explore the associations between the three exogenous latent variables with the two endogenous latent variables of health risk behaviors and access to medical and mental health. Two binary indicator variables, use of VR and use of AJC, were included in the model to assess the effect of the job confidence, health perceptions, and reduced stigma on the use of these two services as well as the effect use of these services had on the outcomes of health risk behaviors and access to medical/mental health care. Each of these variables is defined in Table 1. The SEM was fit using a robust weighted least-squares estimator (WLSMV) in Mplus (Brown, 2006; Muthén, Du Toit & Spisic, 1997) so that items measured on 5-point Likert scales, or fewer categories, were treated as ordinal variables, to avoid biases with the estimates associated with treating such variables as continuous. Pairwise deletion was used within Mplus to respond to missing data. The sample size in the final analysis was 1,984.
Definition of Latent Factors
Definition of Latent Factors
Findings from this study help to expand our understanding of the characteristics of PLWH who use different federal employment services and the relative merits of these different employment programs on contributing to the outcomes of the NHAS. The results are reported in response to each research question.
Characteristics of PLWH who use VR, AJC or neither of these services?
The characteristics of participants who use either VR, AJCs, both, or neither of these services varies significantly across key characteristics. Results of the chi-square analyses describing the sample characteristics are presented in Table 2. A history of incarceration is significantly associated with the use of services (χ2=17.43, df = 3, p value < 0.001). Overall, participants with a history of incarceration access VR services and/or AJCs at a higher rate (45%) than do participants with no history of incarceration (34%). Deviations from the null hypothesis of independence (i.e., those with a history of incarceration choose services in the same proportion as those without such a history) indicate that those with a history of incarceration are more likely to use both services (
Chi-square analyses of association between demographic characteristics and service usel
Chi-square analyses of association between demographic characteristics and service usel
Note: [a]Standardized Pearson residuals greater than two are provided as they indicate specific significant deviations from the independence hypothesis.
Annual income is significantly associated with the use of services (χ2=36.22, df = 3, p value < 0.001); among low income participants earning less than $15,000 annually, 27% have used VR services and/or AJCs, while 40% of those with higher incomes have used such services. Significant deviations from the independence assumption show that participants with low annual incomes of less than $15,000 are less likely to use either service separately (
Homelessness and the use of services were significantly associated (χ2= 19.1, df = 3, p value < 0.001); overall, 42% of those with a history of homelessness have used one or both service whereas 32% of those without a history of homelessness have used a service. Among those who used both services, significantly more participants than expected under the null hypothesis have a history of homelessness (
Participants with a history of treatment for drug use are significantly more likely to use services (χ2= 149.4, df = 3, p value < 0.001). Overall, nearly 50% of participants with a history of drug use have accessed VR or AJC services, or both, whereas only 24% of participants without such a history have used these services. Participants who use either service separately or both simultaneously are more likely than expected to have a history of drug use (
Race has a significant association with choice of services (χ2= 73.2, df = 9, p value < 0.001). Among African Americans, 44.4% have used a service, in comparison with 35% of Latinos, 29% of those from other races, and 26% of Caucasians. Participants who use both services or AJCs alone are more likely than expected to be African American (
Figure 1 illustrates the structural equation model that was used to assess relationships among job confidence, health perception, reduced stigma, VR use, AJC use, and the two outcomes of reduced health-risk behaviors and increased access to mental health and medical care. An initial confirmatory factor analysis assessed the adequacy of the measurement model between the latent variables and their measured variables. All factor loadings were significant (p < 0.001).
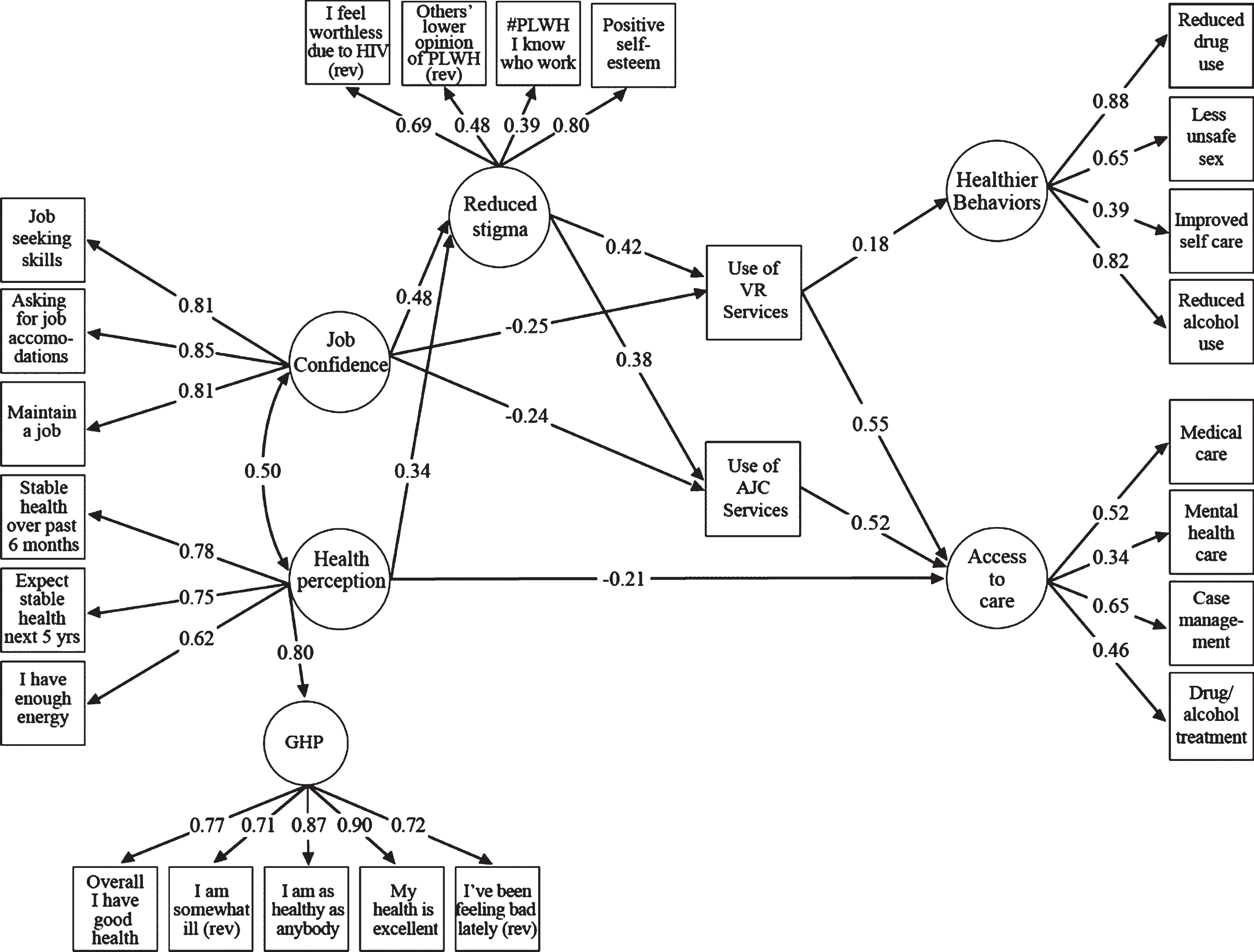
The structural equation model linking health perception (a need factor) and job confidence, through reduced stigma, to the use of VR (enabling factors) and the outcomes of healthier behavior, access to care and job support services.
The fit of the final structural equation model was good (root mean square error of approximation = 0.063, with 90% upper bound of 0.061, Comparative Fit Index = 0.95, Tucker Lewis Index = 0.94). Standardized effects intervals are reported in Table 3 and for each research question below. The path coefficients from the exogenous variables toward the use of VR and toward the use of AJCs are probit estimates (b*) whereas path coefficients that terminate at the continuous endogenous outcomes measures are standardized least squares regression coefficients (b). Unstandardized probit coefficients were used to calculate the probability of VR use.
Impact of VR use and AJC use on access to reduced health-risks and medical care
[a]Estimates are significant at the 0.001 level.
Job confidence has a negative direct effect on the use of both VR services (b* = –0.25, p value < 0.001) and AJC services (b* = –0.24, p value < 0.001) while reduced stigma has a positive direct effect on VR services (b* = 0.42, p value < 0.001) and on AJC services (b* = 0.38, p value < 0.001). The slightly larger, in magnitude, effects of job confidence and of reduced stigma on the use of VR than on the use of AJC is seen in the probability of service usage (Table 4). An individual with high job confidence (one SD above the factor mean) is 4 percentage points (pVR = 0.18, pAJC = 0.14) more likely to use VR services than AJC services. An individual reporting reduced HIV stigma (one SD above the factor mean) is 8 percentage points (pVR = 0.40, pAJC = 0.32) more likely to use VR services than AJC services.
Effect of job confidence, health perspective, and stigma on the probability of service use
Note: [a]At the mean values of the latent variables, the probability of using VR services is 0.24 and the probability of using AJC services is 0.19.
Both job confidence and health perception have significant indirect positive effects on the use of VR services and of AJC services through the latent factor of reduced stigma. Each latent factor has a significant positive direct effect on the latent factor of reduced stigma (p values < 0.001). That is, an increase in job confidence or in health perception is associated with reduced HIV stigma. The indirect effect of job confidence, through reduced stigma, on VR service usage is b* = 0.20 and on AJC services is b* = 0.18 (both p values < 0.001). Greater job confidence and reduced HIV stigma are associated with higher probability of service use. The indirect effect of health perception, through reduced stigma, on VR service usage is b* = 0.14 and on AJC service usage is b* = 0.13 (both p values < 0.001). That is, health perception is not directly associated with either service, but when mediated by a reduction in HIV stigma, greater health perception is associated with a greater probability of using VR or AJC services (Table 4).
Both the use of VR services (b = 0.55) and the use of AJC services (b = 0.52) have a significant positive effect on access to health care (both p values < 0.001). However, only the use of VR services has a significant direct effect on a reduction of health risk behaviors (b = 0.18, p value < 0.001).
Reduced stigma does not have a significant direct effect on either outcome. However, the indirect effect of reduced stigma through the use of VR services has a positive effect on both access to medical care (b = 0.23, p < 0.001) and a reduction in health risk behaviors (b = 0.07, p < 0.001). In addition, the indirect effect of reduced stigma through the use of AJC services has a positive effect on access to care (b = 0.20, p < 0.001) but not on a reduction in health risk behaviors.
Discussion
The two main goals of this study were to gain a better understanding of (a) how the characteristics of PLWH with different patterns of use of federal employment programs differ and (b) how use of VR compared to use of AJC with respect to contributing to the goals of the National HIV/AIDS Strategy related to access to care and reducing health risk behaviors. The findings from this study indicate that the sample as a whole faces significant barriers to employment related to high rates of experiences of homelessness, incarceration, poverty and drug use.
Interestingly, the extent to which these barriers are experienced often differs among those who use employment services (VR and/or AJC) and those who do not use either of these services. Although use of VR is associated with a reduction in health-risk behaviors, an important outcome associated with reduced onward HIV transmission, no such relationship was found with respect to use of AJC services. However, use of VR or AJC services was associated with increased access to care, indicating that both of these federal employment programs play an important role in achieving goals of the NHAS. Overall, use of VR services had a stronger effect than use of AJC services. These results support our hypothesis that VR service use would have a stronger association with public health outcomes than use of AJC services. This discussion will consider the findings associated with each of the key research questions within the broader context of research and practice in this area.
Characteristics of PLWH who use VR, AJC or neither of these services
As noted above, the study participants reported a number of significant challenges that could pose barriers to employment and the need for employment supports. One significant barrier is having a history of incarceration. Because people with a criminal history often face greater barriers to employment than those without a criminal history, it is noteworthy that only 45% of participants who have a history of incarceration reported use of federal employment services, which suggests that these services are underutilized by this group. That these participants are more likely to use neither service may be related to the stigma of having a criminal history (Van Olphen, Eliason, Freudenberg & Barnes, 2009) and the fact that many PLWH may not be aware of the special training and programs that exist to help people with HIV obtain employment (Conyers, 2011). Given the specific challenges that people with disabilities who have a criminal history face, the Rehabilitation Services Administration’s 35th Institute on Rehabilitation Issues (McGuire-Kuletz, Tomlinson & Siblo, 2009) report was devoted to vocational rehabilitation and corrections. This report indicates that people with disabilities who have a criminal history often lack confidence in bureaucracies (which they perceive to have let them down) and recommends that VR professionals need to collaborate and cross train with other human service and corrections professionals to improve outcomes for people with disabilities who have a criminal record.
Poverty is another key barrier to use of employment services, so it is not surprising that only 27% of participants whose income is less than $15,000 dollars per year use federal employment services. Fear of losing income benefits is widely recognized as a barrier to use of employment service for PLWH who receive social security disability benefits (Conyers, 2004; Conyers & Datti, 2008). In recognition of the need to better serve individuals from low income areas, the Rehabilitation Services Administration has developed a cooperative agreement to develop and support a Technical Assistance Center to increase services to individuals with disabilities from targeted low income communities (Office of Special Education and Rehabilitation Services, 2015). Although AJC are free and open to the public to use, research examining the challenges to employment for disadvantaged urban women indicates that health problems and depression often reduce labor market participation (Haney, 2013). This suggests that the additional physical and emotional toll of having HIV may further limit participation in federal employment services among PLWH. The finding that participants earning $15,000 or less are slightly more likely to use VR than AJC may be associated with the access to additional resources that VR counselors can provide to help eligible consumers overcome financial barriers to employment.
Majorities of participants who used AJC (60%), VR (56%), or both services (65%) reported a history of homelessness, and just under half of those who used neither service also reported a history of homelessness. To address the employment needs of PLWH who also have unstable housing, the U.S. Department of Labor, U.S. Department of Housing and Urban Development and the National Working Positive Coalition collaborated to develop a “Getting to Work” training curriculum designed to help housing providers become more informed of the employment needs and challenges of PLWH and the federal employment services designed to assist them with exploring employment (Department of Housing and Urban Development, 2014). The U.S. Department of Labor Office of Disability Employment Policy has also developed resources for all human services professionals to access to learn more about the services, models and research designed to address the employment needs of PLWH (ODEP, 2016a), including a list of HIV housing and other services providers who provide employment services (ODEP, 2016b). These efforts may help to improve services to PLWH who have unstable housing and to increase the numbers of these individuals who are able to benefit from federal employment services.
The finding that almost 50% of participants who have a history of drug use used federal employment services reflects the high rates of comorbidity of HIV and substance use (Meyer, Springer & Altice, 2011; National Institute on Drug Abuse, 2016) and the need for ongoing support for rehabilitation counselors to receive training in substance abuse through initiative such as the Rehabilitation Research and Training Center on Substance Abuse Disability and Employment (Boonshoft School of Medicine, 2015). Despite these efforts, some evidence suggests that VR counselors need additional training in this critically important subject area (Sprong, Melvin, Dallas & Koch, 2014). That participants who did not use any federal employment services were more likely not to have a history of substance abuse may reflect that they had fewer barriers to employment and were in less need than those who had a history of substance abuse. With respect to VR, participants who did not have comorbid substance abuse and HIV may not have significant enough functional limitations to meet the eligibility criteria to be considered a person with a disability. Finally, the finding that participants who use federal employment programs are more likely to be African American underscores the importance of multicultural training for rehabilitation counselors, which is heavily emphasized in the ethical code for Certified Rehabilitation Counselors (Commission on Rehabilitation Counselor Certification, 2012).
The relationship among factors that contribute to VR Use and AJC Use and their effect on reduced health-risk behaviors and access to care
Our findings that both general health perception and job confidence have a positive indirect effect on both VR use as well as on AJC use through the reduced stigma is consistent with previous findings investigating the impact of these enabling factors on VR use within the context of Andersen’s Model of Health Care Utilization (Conyers & Boomer, 2014). In light of previous research that provided support for the health and public health benefits of a range of employment services and interventions for PLWH (Nachega et al., 2015; Richardson et al., 2010, 2013; Rueda et al., 2011, 2012), we hypothesized that use of AJC would also have some individual and public health impact. The results from this study suggest that the effects of general health perception and job confidence have a slightly stronger effect on VR use than on AJC use. In contrast to use of AJC services, the fact that the VR application process entails providing evidence of both (a) having a disability that presents a significant barrier to employment and (b) having a vocational goal may impact this outcome (DOL, 2016; RSA, 2016). For one, participants who used AJC may not have had significant health concerns, thereby reducing a need to consider health perception. Additionally, since AJC use does not require a lengthy application process including determining eligibility related to review of disability status, the effort entailed to participate in these services is less intensive than seeking VR services and may not require as much job confidence to initiate the process. Moreover, because the VR applicant is required to present a vocational goal at the time of application, the level of job confidence or self-efficacy to seek services may need to be stronger than that needed to use the resources of an AJC.
The finding that reduced stigma has a greater effect on seeking assistance through VR services than through AJC services could also be associated with the requirement that PLWH may have to disclose their HIV status as a condition of receipt of service. Since HIV is often a hidden disability, one may not have to contend with the implications of disclosure of HIV status prior to receiving AJC services. However, the fear associated with the potential of HIV disclosure and associated stigma could be more profound when applying for VR compared to applying for AJC services. Having a positive experience with disclosure to rehabilitation counselors who are trained to be sensitive to disability stigma while also gaining access to skills and resources that could enhance vocational identity with an associated shift from a sick role to a work role can further contribute to higher levels of reduced stigma among participants who used VR services (Conyers, 2004).
The separate effects of VR use and AJC use on access to health care and HIV prevention
Interestingly, this study found that, in contrast to VR use, AJC service use was not associated with reduction in health-risk behaviors. This outcome may be associated with two other key differences in these service systems. For one, use of VR services typically are far more intensive than those provided at AJC and can include funding to refer consumers to other services, including mental health, that will help reduce barriers to employment (RSA, 2016). Furthermore, VR services tend to place a greater emphasis on hiring master’s-level vocational rehabilitation counselors who have more extensive training in counseling skills, knowledge of disability, multicultural training, and psychosocial aspects of disability. This combination of access to enhanced resources and trained professionals may lead to improved outcomes for these participants. However, because these variables were not specifically addressed in this study, more research is needed in this area.
Implications for Policy and Practice
As the demographic and health pictures of PLWH continue to evolve, several implications arise regarding the need for vocational services, the type of services individuals will be eligible for and the impact of these services on individual and public health outcomes. With effective treatment, many PLWH are able to thrive with fewer functional limitations than ever before. For many, this outcome may pose a significant challenge to being found eligible for vocational rehabilitation services. Although many PLWH still contend with significant internalized and social stigma, which can pose a tremendous barrier to employment, they may have a more difficult time meeting the functional limitation requirements for VR eligibility. As the demographics of HIV have changed over the years, so has the progression of rehabilitation legislation culminating in the most recent 2014 reauthorization of the Workforce Innovation and Opportunity Act (WIOA). This reauthorization created a significant shift of focus in vocational rehabilitation services, placing much greater emphasis on youth in transition, leading many to wonder about the implications for having limited remaining resources to address the needs of adults with chronic illnesses. With stagnant funding of VR services, the Order of Selection waiting lists will likely increase across the country and make it even more difficult for PLWH to demonstrate the level of functional limitation to be prioritized for receipt of services, possibly leaving them to seek other vocational services such as the AJC. Given the findings that AJC do not have the same level of impact as VR services, this could be a setback to the gains fostered by interagency coordination to end the AIDS epidemic.
In addition to the shift of focus and funding resulting from passage of the WIOA, this legislation has also weakened the definition and standards of a qualified rehabilitation personnel with less of an emphasis on counseling or requirement for master’s-level education. It is hard to know what impact these changes will have on the VR service system and the potential ongoing contributions that these services can contribute to the goals of the NHAS.
Fortunately, the updated NHAS elevated the role of the Rehabilitation Services Administration (RSA) by inviting a representative from RSA to participate on the federal inter-agency planning committee. Hopefully, these efforts will help to foster continued education and training in this area to support successful linkage and positive employment outcomes. The U.S. Department of Labor has played a significant role in the implementation of the NHAS as noted by its collaboration with the U.S. Department of Housing and Urban Development and the National Working Positive Coalition to develop online training modules related to HIV and Employment to foster awareness of the emerging needs of PLWH and how to best address their vocational development needs. With leadership from both of these federal employment services on the NHAS planning committee, ongoing consideration can be devoted to training staff at both agencies and working together to address the emerging and unmet employment needs of PLWH.
Given the limitations of federal agencies to meet all of the vocational needs of PLWH, it will also be important to support a variety of non-federal employment services across the country as a number of studies document the effectiveness of these programs, some of which collaborate with their federal partners. As PLWH contend with the trauma of an HIV diagnosis, many may benefit from a range of prevocational services to help these individuals to be better able to successfully link to both VR and AJC services, including services to help reduce HIV stigma. Given the exploratory nature of this study, ongoing research is needed in this area, including more in-depth measures of level of engagement and participation in these services. Longitudinal research is needed to better assess the impact of change over time.
Limitations
There are a number of limitations to this study as this line of research is still in its early stages and has to adapt to the ongoing issues and challenges facing this emergent disability group. One limitation is that participation in the study was voluntary, so those who chose to participate may be different from those who declined to participate and the findings may not generalize to all PLWH. To counter this limitation, efforts were made to ensure diverse inclusion of PLWH representing key populations most impacted by HIV. A second limitation was the cross sectional design. Additional longitudinal research is needed using an experimental design with random assignment to better assess the impact of VR and AJC on HIV health and prevention outcomes over time. A longitudinal design could also provide an opportunity to track service use over time, including measures of type and length of services provided. This would help enhance our understanding of the mechanisms that most impact access to care and reduced health-risk behaviors. Another limitation of the study was that the majority of participants were recruited from ASO, indicating that they already had some connection to HIV care. Also, the survey responses were based upon self-reports, which poses a risk of response bias given the sensitive nature of some of the questions relating to personal health, stigma, sexual activity, and financial issues.
Conclusion
This study examined the patterns of use of two essential federal employment services, VR and AJC, by PLWH. Overall, the sample faced significant barriers to employment, which underscores the need for these services. Given that the extent of employment barriers differed among those who used these services, it is critical to provide a range of service models to meet the diverse employment needs of this population. The finding that use VR and/or AJC contribute to increasing access to care supports the inclusion of state/federal vocational rehabilitation and U.S. Department of Labor employment services as key partners in achieving the goals of the National HIV/AIDS Strategy. In addition to increasing access to care, use of vocational rehabilitation services also contributed to the reduction in health-risk behaviors, underscoring the importance of providing more intensive services with providers with a strong background and training in rehabilitation counseling.
Conflict of interest
None to report.