
Abstract
BACKGROUND:
Multiple sclerosis (MS) symptoms often make it difficult for individuals with MS to stay at work or return to work. It is important to understand the relationship between symptom clusters and employment. Person-environment (P-E) contextual factors such as core self-evaluations (CSE) and social support have been found to be effective mediators for the relationship between disability and participation in rehabilitation research and may be able to reduce the adverse impact of MS symptom cluster on employment outcome of people with MS.
OBJECTIVE:
To evaluate the mediation effect of CSE and social support on the relationship between symptom cluster and employment in MS.
METHOD:
Quantitative descriptive research design using two simple mediation analyses. 154 persons with multiple sclerosis participated in this study.
RESULTS:
Results show that symptom cluster, CSE, and social support were significantly related to employment. Both CSE and social support were significant mediators of the relationship between symptom cluster and employment, with CSE a stronger mediator than social support.
CONCLUSIONS:
Managing MS symptoms and increasing CSE and social support will reduce the adverse impact of MS symptom cluster on employment outcome. Therefore, CSE and social support can be viewed as protective factors for maintaining employment in MS. These results provide support for the use of positive psychology interventions by vocational rehabilitation counselors working with individuals with multiple sclerosis.
Introduction
Employment is considered to be an important public health intervention for people with multiple sclerosis (MS). Individuals with MS who are employed, whether full or part-time, have better psychosocial and health outcomes than individuals who are not employed (Chiu et al., 2015). Employment, even at low levels, is associated with better health and better overall functioning for people with disabilities (Chiu et al., 2015; Hall, Kurth, & Hunt, 2013; Muller et al., 2017). Studies have shown that individuals with disabilities who have unsteady employment or who are unemployed tend to experience more mental and physical health problems, consume higher amounts of alcohol, and report lower self-esteem and overall well-being when compared to employed adults (Dutta, Gervey, Chan, Chou, & Ditchman, 2008; Krause, Carter, Pickelsimer, & Wilson, 2008; Murali & Oyebode, 2004). Work is believed to be beneficial because it increases financial security and access to high-quality heath care, which in turn improves health status, social relationship, mental health, and quality of life (Jackson, Iezzi, & Lafreniere, 1996; Reisine, Fifield, Walsh, & Forrest, 2008).
According to the National Multiple Sclerosis Society (NMSS), approximately 400,000 individuals are living with MS in the United States (NMSS, 2014). MS is a chronic illness of the central nervous system that impacts physical, psychological, and social functioning (Tortorella et al., 2014; Tesar, Baumhackl, Kopp, & Gunther, 2003; Costa, Sa, & Calheiros, 2012). Age of onset for MS is generally between 20 and 50 years (McFadden et al., 2012). MS is associated with several symptoms that can result in loss of employment, economic and social status, and social relationships (Costa, Sa, & Calheiros, 2013; Pack, Szirony, Kushner, & Bellaw, 2014; Moore et al., 2013). MS symptoms have been studied in symptom clusters because they often co-occur and may have a compounding impact on an individual (Crayton & Rossman, 2006; Motl & McAuley, 2009; Motl, Suh, & Weikert, 2010). The study of symptoms clusters considers that multiple symptoms often occur concurrently and that co-occurring symptoms can provide a more useful construct for assessment and management than a single symptom (Dodd, Miaskowski, & Paul, 2001; Kim, McGuire, Tulman, & Barsevick, 2005; Miaskowski, Dodd, & Lee, 2004). Symptom clusters are defined as “three or more concurrent symptoms (e.g., pain, fatigue, sleep insufficiency) that are related to each other” (Dodd et al., 2001, p. 465). Symptoms associated with MS include pain, stress, depression, sleep problems, cognitive impairments and fatigue (Motl & McAuley, 2009).
Due to the progressive, unpredictable, and disabling nature of MS and its associated symptoms, employment rates for individuals with MS are low (O’Connor, Cano, Thompson, & Playford., 2005). Research shows that because of symptoms associated with MS and their impact on physical functioning, mental health, and social participation (Kwiatkowski et al., 2014; Ng, Amatya, & Khan, 2013), individuals with MS have lower community participation when compared to the general population (Khan & Pallant, 2007). Given the evidence of the benefits of work and considering that symptom clusters have a significant impact on participation for persons with MS, it is important that we better understand the relationship between symptom clusters and employment.
Rehabilitation researchers and scholars have long recognized the need to consider contextual and environmental factors in the development of effective practice (Chan, Taryvdas, Blalock, Strauser, & Atkins, 2009; Wright, 1983). Recent research on the World Health Organization’s (WHO) International Classification of Functioning (ICF) as a model for vocational rehabilitation (VR) demonstrates the importance of person-environment (P-E) contextual factors in mediating the effect of impairments on participation (Chan et al., 2009). The positive human traits factors of core self-evaluations (CSE) and social support are considered effective P-E contextual factors in ICF research (Smedema, Chan, & Phillips, 2014; Smedema, Chan, et al., 2015; Smedema, Pfaller, et al., 2015; Wilson et al., 2013).
Core self-evaluations
Core self-evaluations (CSE) is a positive human trait construct that has received considerable attention as a positive person (P) variable in ICF research. It is defined as the overall, fundamental perception that people have about their worth and capability as human beings (Judge, Locke, Durham, & Kluger, 1998). The CSE construct was first developed as part of a theoretical framework to explain dispositional influences on job satisfaction (Judge, Locke, & Durham, 1997) and then extended to explain life satisfaction (Judge, Bono, Erez, & Locke, 2005). CSE is a higher order construct comprised of four lower-order traits: self-esteem, self-efficacy, locus of control, and emotional stability (Judge et al., 1998). Self-esteem is defined as a global appraisal of one’s self-worth (Rosenberg, 1965). Self-efficacy is defined as one’s belief in his or her ability to produce desired outcomes when performing specific activities and pursuing goals (Bandura, 1977). Emotional stability is defined as the tendency to feel calm and secure (Eysenck, 1990). The final CSE trait is locus of control, which is defined as one’s belief that he or she has personal control over events in life, rather than believing that events are controlled by others or fate (Rotter, 1966).
Judge et al. (2005) noted that individuals’ fundamental evaluations of themselves impact all their beliefs about their lives. Judge et al. (1998) notes that people who consider themselves to be good or competent will react differently to obstacles in life than individuals who believe they are incompetent. Correspondingly, people with MS who consider themselves to be competent and worthy might cope more adaptively to the symptoms associated with their condition and, believing themselves to be capable of working, put more effort into pursuing employment. Conversely, people with MS who feel they are incompetent or lacking value may succumb to their symptoms, concluding that any attempt they make at pursuing employment will result in failure. Therefore, individuals with high CSE may have higher levels of employment than those with low CSE. There have not been any studies of the relationship between CSE and employment for individuals with MS. However, Smedema, Chan, and Phillips (2014) performed a study analyzing the relationship between CSE and participation for individuals with spinal cord injury and found that CSE contributes to life satisfaction and participation, including work participation. The study also found that CSE has a unique role in increasing motivation to pursue goals, which also predicts participation and life satisfaction. Research has also shown that CSE contributes to life satisfaction for college students with disabilities because they are better able to cope with stress, maintain a positive mood, and build social supports (Smedema et al., 2015).
Social support
Social support is a positive environment (E) construct that performs a vital role in an individual’s health and well-being (Chronister, Johnson, & Berven, 2006; Chronister, Chou, Frain, & Cardoso, 2008; Wilson et al., 2013). Social support is defined as the social network in which an individual interacts, maintains contact, and shares with others (Costa et al., 2012). Social contacts are among the most important resources for promoting resilience in coping because they function as a buffer to mediate the impacts of stress (Martin & Martin, 2002). The benefits of strong social support for individuals with MS include reduced medical impairments, mortality, and increased quality of life, and community participation (Schwartz & Frohner, 2005; Yamout et al., 2013). Social support is also a facilitator to well-being and improved daily functioning for individuals with MS (Hamed, Tariah, & Hawamdeh, 2012). Although there is a paucity of studies regarding the relationship between social support and employment for individuals with MS, it is likely that having strong social support and the related benefits would increase the likelihood of employment for individuals with MS.
Purpose of the study
To iterate, the positive effect of employment is well documented in the literature. However, the employment rate of people with MS is notoriously low. It is hypothesized that positive P-E factors could reduce the adverse effect of MS cluster symptom on employment. CSE and social support have been found to be effective P-E contextual factors for predicting community integration and participation in several disability groups (e.g., people with SCI and college students with disabilities). The purpose of the present study is to evaluate CSE and social support as P-E mediators for the relationship between symptom cluster and employment for persons with MS.
Methods
Participants
One hundred and fifty-four prime working-age adults with MS participated in the present study. Participants were recruited from two regional chapters of the National Multiple Sclerosis Society (NMSS) including the Greater Washington D.C./Maryland Chapter in Washington D.C. and the Wisconsin Chapter in Hartland, Wisconsin. Inclusion criteria required individuals to be (a) diagnosed with multiple sclerosis, (b) between the ages of 25 and 54 (prime working-age), and (c) currently living in the community. The mean age of the participants was 41.03 years (SD = 8.04). Most of the participants were women (87%), married (53%), and white (83%). Participants in the current study were relatively well-educated with 88% having some college education, two- or four-year college degrees, or graduate degrees. Fifty-nine percent of the participants were employed either part-time or full-time. The average age of MS diagnosis was 32.28 years old (SD = 8.56), with the majority of participants (86%) experiencing relapsing-remitting multiple sclerosis (RRMS). A detailed description of participant characteristics is presented in Table 1.
Participant Demographic Characteristics and MS Characteristic (N = 154)
Participant Demographic Characteristics and MS Characteristic (N = 154)
Core self-evaluations
The Core Self-Evaluations Scale (CSES) developed by Judge, Erez, Bono, and Thoresen (2003) was used to assess CSE. The CSES is a 12-item measure (e.g., “I am confident I get the success I deserve in life”) and each item is rated on a 5-point Likert-type scale (1 = strongly disagree to 5 = strongly agree). CSE scores were calculated by summing the 12 CSES items, with higher scores indicating greater levels of CSE. The Cronbach’s alpha coefficient for CSES in the present study was computed to be 0.88.
Symptom cluster
Symptom cluster included separate measures of pain, stress, sleep difficulty, depression and fatigue. Pain was measured using a four-item version of the Numeric Pain Scale (NPS; Castarlenas, Jensen, von Baeyer, & Miro, 2017; Childs, Piva, & Fritz, 2005), which captures present levels of pain intensity (e.g., “How would you rate your pain right now?”) and past week pain (e.g., “How would you rate your worst level of pain during the last week?”). Each item is rated on a 11-point Likert-type scale, ranging from 0 (no pain) to 10 (worst imaginable pain). Pain scores are computed by averaging the four items, with higher scores indicating greater levels of pain. The Cronbach’s alpha coefficient for NPS in the present study was computed to be 0.94. Stress was measured by an abbreviated version of the Perceived Stress Questionnaire (PSQ; Levenstein et al., 1993). It is composed of 9 items (e.g., “During the past month, have you felt under pressure from deadlines?”) and each item is rated on a 4-point Likert type scale (1 = almost never to 5 = usually). Stress scores were calculated by averaging the nine items with higher scores indicating greater levels of stress. The Cronbach’s alpha coefficient for PSQ in the present study was computed to be 0.88.
Sleep difficulty was measured using an abbreviated version of the Medical Outcomes Study-Sleep Scale (MOS-Sleep; Stewart, & Ware, 1989). The MOS-Sleep Scale is comprised of four items (e.g., “How often during the past 4 weeks did you feel that your sleep was not quiet [moving restlessly, feeling tense, speaking, etc., while sleeping?”]), with each item rated on a 6-point Likert type scale (1 = none of the time to 6 = all of the time). Sleep difficulty scores were computed by averaging all four items, with higher scores indicating greater levels of sleep difficulty. The Cronbach’s alpha coefficient for MOS-Sleep in the present study was computed to be 0.63. Depression was measured using the Patient Health Questionnaire-4 (PHQ-4: Kroenke, Spitzer, Williams, & Lowe, 2009). The PHQ-4 is a 4-item measure (e.g., “Over the last 2 weeks, how often have you been bothered by feeling nervous, anxious or on edge?”), with each item is rated on a 4-point Likert type scale (0 = not at all to 3 = nearly everyday). Depression scores were calculated by summing the items, with higher scores indicating greater levels of depression. The Cronbach’s alpha coefficient for PHQ-4 in the present study was computed to be 0.90. Fatigue was measured using the abbreviated version of the Modified Fatigue Impact Scale (MFIS; Larson, 2013). The brief MFIS is a five-item measure (e.g., “Because of my fatigue during the past four weeks I have been less alert”), with each item rated on a 5-point Likert scale (0 = never to 4 = always). Fatigue scores were computed by averaging the MFIS items with higher scores indicating greater levels of fatigue. The Cronbach’s alpha coefficient for MFIS in the present study was computed to be 0.91. Exploratory factor analysis was computed for the symptom cluster variables with a one-factor solution and the participants’ factor scores were used to generate symptom cluster scores for the participants.
Social support
The Interpersonal Support Evaluation List (ISEL-12) developed by Cohen, Mermelstein, Kamarck, and Hoberman (1985) was used to assess perceived social support. The ISEL is a 12-item measure (e.g., “If I wanted to go on a trip for a day [for example, to the country or mountains], I would have a hard time finding someone to go with me.”), with items rated on a 4-point Likert scale (0 = definitely false to 3 = definitely true). Social support scores were computed by averaging the items with higher scores indicating greater levels of perceived social support. The Cronbach’s alpha coefficient for ISEL-12 in the present study was computed to be 0.86.
Procedures
Participants were recruited by advertisements through monthly electronic newsletters and through a single round of direct email solicitation sent by NMSS chapters to their members. Participants who completed the online survey received a US$15 gift card upon completion of the study. The University of Wisconsin-Madison Institutional Review Board (IRB) approved this study.
Data analysis
The Statistical Package for the Social Sciences (SPSS) version 24.0 was used to compute descriptive statistics. The SPSS INDIRECT macro written by Preacher and Hayes (2008) was used to compute the mediation analysis.
Results
Correlation analysis
Multiple sclerosis symptom cluster was found to be negatively associated with CSE (r = –0.70, p < 0.001) and employment status (r = –0.23, p < 0.01). Core self-evaluations was positively related to employment status (r = 0.31, p < 0.001). Symptom cluster was negatively associated with social support (r = –0.26, p < 0.01) and employment status (r = –0.29, p < 0.001).
Mediation analysis
Two simple mediation analyses were computed to evaluate the relationship between MS symptom cluster and employment status using CSE and social support as mediators.
Core self-evaluations
The following are the equations for symptom cluster and employment with CSE as the mediator:
Total effect (c) = Direct effect (c′) + Indirect effect (a × b)
Because employment status is a dichotomous variable, coefficients in Equations 1 and 3 were estimated in INDIRECT using logistic regression, whereas ordinary least-squares (OLS) regression was used for the coefficients in Equation 2. A graphical representation of the simple mediation model for CSE and information for the unstandardized path coefficients (a, b, c, and c′) are presented in Fig. 1.
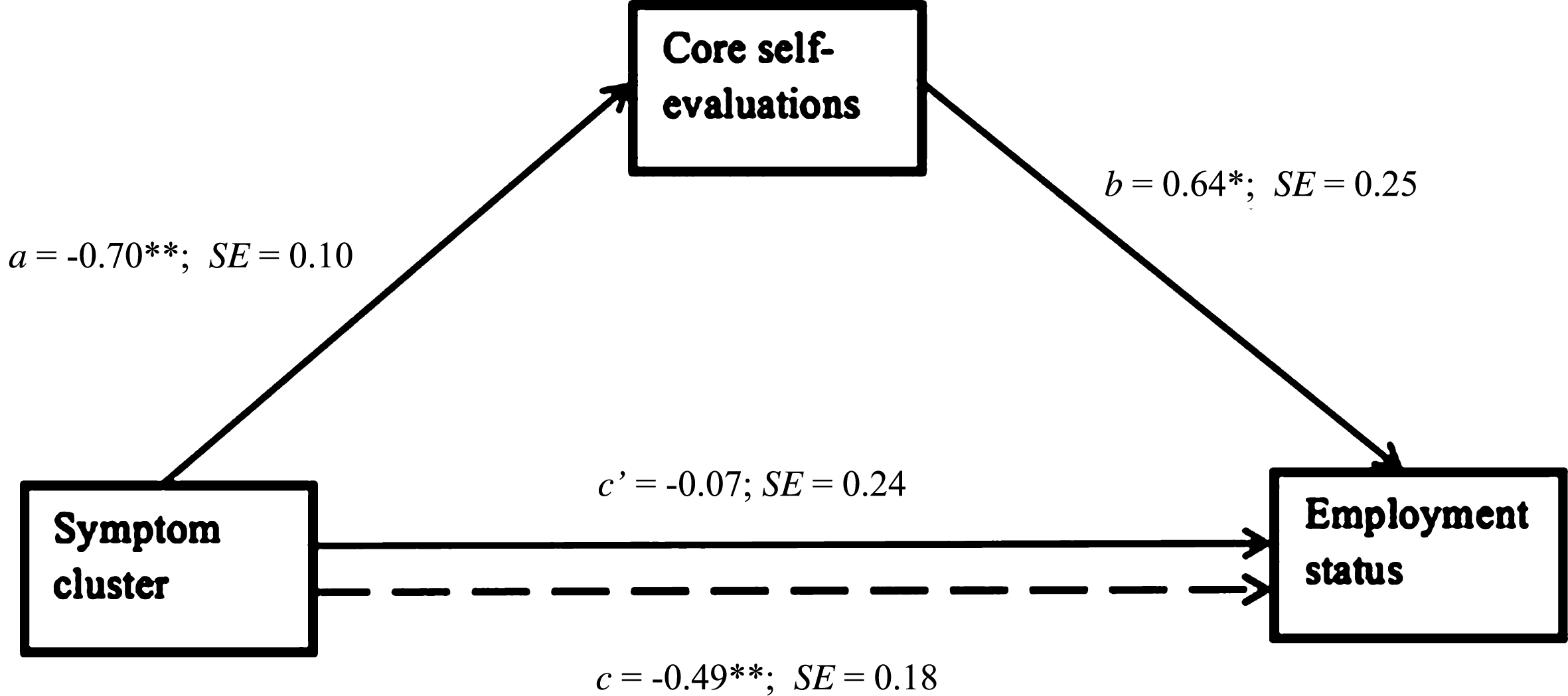
Path Coefficients for Simple Mediation Analysis on Employment Status (N = 154). Note. Dotted line denotes the effect of MS symptom on employment status when CSE is not included as a mediator. b, c and c’ are unstandardized logistic regression coefficients, a is an unstandardized ordinary least squares (OLS) regression coefficient. *p < 0.05, **p < 0.01, ***p < 0.001.
As can be observed in Fig. 1, the odds of being employed were lower among individuals with higher levels of MS symptoms (Total effect: c = –0.49, p < 0.01). Symptom cluster was negatively associated with CSE (path a = –0.70, p < 0.01). Finally, CSE was positively associated with the odds of being employed (path b = 0.64, p < 0.05) after controlling for the effect of symptom cluster. The direct effect of symptom cluster (c′= –0.07) on employment status was not statistically significant after controlling for the effect of CSE, indicating CSE fully mediated the relationship between symptom cluster and employment status. The indirect effect of symptom cluster on employment through CSE was evaluated using bootstrapping (Preacher & Hayes, 2008; Hayes, 2009). This indirect effect is considered significant if the bias-corrected bootstrap confidence interval (CI) for the product of path a and path b does not include zero. Using the Preacher and Hayes (2009) INDIRECT procedure with 5,000 bootstrap samples revealed a significant indirect effect of MS symptoms on employment through CSE (point estimate = –0.45, 95% CI: –0.81 to –0.08).
The equations for symptom cluster and employment with social support as the mediator are as follows:
A graphical representation of the simple mediation model for social support and information regarding the unstandardized path coefficients (a, b, c, and c’) are presented in Fig. 2.

Path Coefficients for Simple Mediation Analysis on Employment Status (N = 154). Note. Dotted line denotes the effect of MS symptom on employment status when social support is not included as a mediator. b, c and c’ are unstandardized logistic regression coefficients, a is an unstandardized ordinary least squares (OLS) regression coefficient. *p < 0.05, **p < 0.01, p*** < 0.001.
As can be observed in Fig. 2, the odds of being employed were lower among individuals who have higher levels of MS symptoms (Total effect: c = –0.49, p < 0.01). Symptom cluster was negatively associated with social support (path a = –0.27, p < 0.01). Finally, social support was positively associated with the odds of employment (path b = 0.53, p < 0.01). The direct effect of symptom cluster (c′= –0.37, p < 0.05) was still statistically significant but reduced after controlling for the effect of social support. Using the INDIRECT procedure with 5,000 bootstrap samples revealed a significant indirect effect of MS symptom cluster on employment through perceived social support (point estimate = –0.14, 95% CI: –0.31 to –0.04). The results indicated that perceived social support partially mediates the relationship between symptom cluster and employment status.
Work has received considerable attention in recent years as a public health intervention for people with disabilities including people with MS (Chiu et al., 2015; Hall, Kurth, & Hunt, 2013; Muller et al., 2017). Factors such as unemployment, income inequality and poverty can cause considerable levels of psychological distress, resulting in high prevalence of secondary health conditions among people with disabilities. Conversely, employment, even at low levels, has been associated with better health and health behaviors as well as lower healthcare expenditures (Hall et al., 2013). Research has indicated that staying at work for as long as possible and returning to work when possible helps people with disabilities including people with MS maintain better health and well-being (Hall et al., 2013). It is well-documented that pain, stress, sleep problems, fatigue and depression are common occurrence among people with MS and these symptoms significantly affect their stay-at-work and return-to-work outcomes. Therefore, identifying psychosocial factors that promote employment for people with MS is warranted.
In recent year, there is a trend to move away of focusing on pathology but to focus on elevating positive human strengths and promoting positive supportive communities. Within the ICF framework, the disability-employment relationship is mediated by person-environment (P-E) contextual factors (Chan et al., 2009).
In this study, we first confirmed the relationships among MS symptom cluster, CSE, social support, and employment. MS symptom cluster, CSE, and social support were all significant predictors of employment. Second, we tested CSE and social support, respectively, as P-E mediators for the relationship between MS symptoms cluster and employment. Both of the tested models accounted for significant variance in employment, with CSE fully mediating the relationship between symptom cluster and employment and social support partially mediating the same relationship. In other words, the presence of CSE rendered the symptom cluster-employment relationship nonsignificant, while social support could reduce the total effect of the symptom cluster-employment relationship but the direct effect remains statistically significant.
These findings suggest that both CSE and social support play an important role in the employment of people with MS, with CSE acting as a stronger mediator than social support. Together, increasing both CSE and social support will reduce the adverse impact of MS symptom cluster on employment outcome. Therefore, CSE and social support can be viewed as protective factors for maintaining employment in MS.
Implications for rehabilitation practice
The findings of this study have important implications to rehabilitation practice. First, our finding that symptom cluster directly influences employment suggests that health promotion interventions can be utilized to reduce the negative influence of MS symptoms on employment outcomes. For instance, engaging in regular exercise and physical activities could help people with MS alleviate depressive symptoms, restore function, improve health self-management, promote wellness, and increase community participation including employment (White & Dressendorfer, 2004). Perhaps more importantly for rehabilitation counseling, our findings show that much can be done to address employment of clients with MS regardless of symptom severity.
The adverse impact of MS symptom cluster on employment outcome can be reduced and even eliminated by client CSE. It has been argued that CSE can be improved through the use of positive psychology interventions (Smedema, 2014). Judge and Kammeyer-Muller (2011) discussed the potential malleability of CSE despite its stable, trait-like construct nature. They indicated for instance that CSE could be increased through the use of positive feedback. Core self-evaluation for individuals with MS may be improved by focusing on psychosocial interventions on positive personality traits. Specifically, methods for enhancing self-esteem, generalized self-efficacy, internal locus of control, and emotional stability. For instance, self-esteem can be increased by developing coping strategies (Smedema, Catelano, & Ebener, 2010).
Social support has been associated with happiness and well-being (Charlifue, 1999; Schulz & Decker, 1985; Wilson et al., 2013). However, it is well documented that the distress causing by disability reduce perceived social support (Elliott, Herrick, Witty, Godshall, & Spruell, 1992). Social support can potentially be increased by training clients on making clear and active requests for help to natural supports and to better communicate social support needs, including providing suggestions on how help could be provided (Rini & Dunkel-Schetter, 2010). Further, effectively providing social support requires providers to acknowledge and encourage a sense of competence and skill in the receiver (Elliott et al., 1992). The use of natural supports has been found to increase social relationship of people with disabilities in the workplace (Mank, Cioffi, & Yovanoff, 1997).
Limitations
Several limitations inherent this study should be considered when interpreting the study findings. This study used a cross-sectional convenience sample of individuals who provided anonymous responses to an online, self-report survey. Self-report measures are susceptible to social desirability bias and response bias. Participants were recruited online through the National MS Society. It is possible that individuals who participate in this organization differ from the broader population of people with MS. Participants were predominantly White and well-educated, reflecting higher socioeconomic status and an underrepresentation of individuals with other racial/ethnic background. These limitations might reduce the generalizability of the findings.
Conclusion
This study examined CSE and social support as P-E mediators for the relationship between MS symptoms cluster and employment. Findings provide increased understanding of the intermediary roles of CSE and social support in explaining how to reduce the effect of MS symptom cluster on employment outcomes of people with MS. Specifically, MS symptoms can be improved through health promotion interventions, and evidence suggests that both CSE and social support can be enhanced with psychosocial interventions (Smedema, 2014). Thus, this study provides an alternative way to improve employment outcome of people with MS.
Conflict of interest
None to report.
Footnotes
Acknowledgments
The contents of this article were developed with support from the Rehabilitation Research and Training Center (RRTC) on Employment of People with Physical Disabilities. The RRTC was funded by the National Institute on Disability, Independent Living and Rehabilitation Research Grant H133B13001 to Virginia Commonwealth University.