
Abstract
BACKGROUND:
Over the past decade, knowledge translation (KT) has emerged as a framework for turning research findings into actions which will improve outcomes for individuals with disabilities.
OBJECTIVE:
This article examines how the origins of KT in healthcare have shaped (and perhaps limited) how it has been conceptualized in the realm of disability and, more specifically, disability and employment.
CONCLUSION:
We focus on three questions. First, how have the origins of KT shaped the epistemological commitments informing its use in the realms of healthcare and disability? What features do these commitments draw attention to? What features do they render invisible? Second, the realm of disability is characterized by a more complex and disparate landscape of stakeholders than is the case in healthcare. Stakeholder groups are not simply neutral knowledge users. Each stakeholder group has a unique culture, discourse, epistemology and view of “success.” What does this mean for KT in the realm of disability? Third, the Knowledge-to-Action (K2A) Framework (Graham et al., 2006) has been widely adopted in several realms: Healthcare, education, international development and disability. Given the unique challenges of KT in the realm of disability, how might the K2A Framework need to be adapted to strengthen its effectiveness?
Keywords
Introduction
Over the past two decades, significant research attention has been directed toward disability (see, for example, Gould et al., 2015; Hoffman, 2008; Parker Harris et al., 2014) and toward disability and employment (Gewurtz, Langan, & Shand, 2016; Hallock, Jin, & Barrington, 2013a; Hallock, Jin, & Barrington, 2013b; Karpur, VanLooy, & Bruyere, 2014; Phillips, Deiches, Morrison, & Chan, 2016). Yet, individuals with disabilities continue to struggle with barriers to accessibility and equal opportunity in many areas of life (Aranda, 2015; Erickson, Lee & von Schrader, 2014; McMahon, 2012). This struggle seems most challenging in the area of employment, with several studies pointing to the continued persistence of disability discrimination despite over a quarter-century of the Americans with Disabilities Act (ADA) and other policy provisions (See, for example, Ameri, et al., 2015; Nazarov & Von Schrader, 2014; Shaw, 2013).
The research on disability is broad and deep, and many resources have been used in its generation. It offers important insights into the nature of disability discrimination in employment and what can be done to improve the employment outcomes of individuals with disabilities. Yet, the numbers remain, for the most part, unchanged. Why has this knowledge so stubbornly refused to be turned into actions? This point was driven home for the authors during a recent conversation with a disability consultant who worked with employers.
What really gets me is this: I did a training for an employer last week. When we were planning the session, they sent me a presentation they wanted me to do. I realized it was exactly the same presentation I had done for the same company one, five, ten and twenty years ago. Why do they keep paying me to come in and tell them exactly the same thing? Why aren’t they doing it instead of just learning about it? Why are they throwing the same information at an old problem?
The field of disability is, of course, not the first to struggle with turning knowledge into actions that change outcomes. In the field of healthcare, there is a long history of attempting to inform practice with evidence. But the flow from evidence to practice to outcomes has not been fast or easy. Studies show that new evidence takes about 17 years to be incorporated into practices that improve health outcomes for patients (Agency for Health Research & Quality, 2001; Field, Booth, Ilott & Gerrish, 2014). In the disability arena, the flow of evidence to practice to outcomes is even more complex, with a wider range of stakeholders, less clarity about who decision gatekeepers really are, and less consensus between stakeholder groups about what constitutes a “successful” outcome. Reaching stakeholders and decision gatekeepers who are pivotal to employment outcomes is one of the greatest challenges faced by the disability community. What is the power of knowledge translation (KT), as it is currently applied, in meeting this challenge?
The purpose of this article is to consider the emergence of KT in the sphere of disability, with specific attention to KT issues in disability and employment. Our discussion centers on three areas. First, how have the origins of KT shaped the epistemological commitments (beliefs about what constitutes valuable or useful knowledge) informing its use in the realms of healthcare and disability? What features do these commitments draw attention to? What features are rendered invisible? Second, what is the stakeholder landscape for KT in the realm of disability and employment? The different groups making up the stakeholder landscape for disability and employment each have unique cultures, levels of power and assumptions of what constitutes “legitimate” knowledge or evidence. How does this complex stakeholder landscape affect the flow of knowledge from evidence to practice to outcome? Third, how might commonly-used KT models such as the Knowledge-to-Action (K2A) model (Graham et al., 2006) need to be re-considered in light of the unique challenges and stakeholder landscape of disability and employment?
The origins, commitments and use of KT in healthcare and disability
Since ancient times, scholars have lamented the difficulty of turning knowing into doing— of turning research knowledge into actions which benefit society. KT frameworks as we know them today emerged from several sources. The concept that knowledge should inform planned change became codified during the 1960 s in Everett Rogers’ Diffusion of Innovation (DOI) Theory (Rogers, 1962). Though DOI theory was (and still is) widely applied in arenas such as international development and policy implementation, criticism of Roger’s model has been ongoing (see for example Lundblad, 2003; Lyytinen & Damsgaard, 2001). In short, these criticisms have pivoted around several points: the theory’s attention to top-down processes, the de-contextualization of innovation adoption decisions, the rendering invisible of power relationships between innovators and adopters, and the dismissive stance taken toward those who chose not to adopt— “laggards.” Interestingly, as we discuss later, the echo of these criticisms can be heard in more recent reflections on current KT models.
A key issue of DOI theory, however, was its lack of operational specificity and its over-generalized definition of “innovation.” For this and other reasons, models that more concisely targeted the movement of knowledge from researchers to users rapidly emerged across several arenas: such as organizational development, business, policy studies and education. But it was in the field of healthcare where KT first became systematically codified and applied. In 2000, the Canadian Institutes of Health Research (CIHR) defined KT for the Canadian context as “ ... a dynamic and iterative process that includes synthesis, dissemination, exchange and ethically-sound application of knowledge to improve the health of Canadians, provide more effective health services and products and strengthen the health care system” (CIHR, 2000).
Though KT was born in the world of healthcare, it was rapidly embraced by the National Institute for Disability, Independent Living, and Rehabilitation Research (NIDILRR) (Rogers & Marin, 2009). In 2005, NIDILRR put forth a definition of KT as “ ... the collaborative and systematic review, assessment, identification, aggregation, and practical application of high-quality disability and rehabilitation research by key stakeholders (i.e., consumers, researchers, practitioners, and policymakers) for the purpose of improving the lives of individuals with disabilities” (NIDRR, 2005). KT also became a key feature of NIDILRR’s Long Range Plan (U.S. Department of Education, 2006).
Clearly, KT has been embraced by agencies funding disability research and by disability policy makers. NIDILRR’s 2005 definition of KT has been frequently cited by authors both within and outside the disability community and has been positioned as one of the two main definitions of KT in use today (see, for example, Straus, Tetroe & Graham, 2013). Also, NIDILRR’s 2007 publication Knowledge translation: Introduction to models, strategies, and measures (Sudsawad, 2007) is considered a landmark article, providing a valuable overview of KT applications both within and outside the disability field. The NIDILRR definition of KT was put forward to spearhead a more collaborative, interactive form of KT that could embrace the complexity of the disability sphere. It would seem the field of disability should be poised to play a key role in the development of new KT insights, frameworks and models. Issues within the field of disability represent a unique set of challenges for KT— challenges which could advance the field of KT generally. Is this call being answered within the field of disability?
Table 1 shows the number of publications per decade yielded by taking the mean number of search results across three databases: PubMed, ProQuest and Google Scholar. The searches for each database were fully equivalent, but varied search terms by topic: KT (only), KT + healthcare and KT + disability/ies. This shows an explosion of attention to KT over the past 35 years. This explosion, however, has mostly occurred within the field of healthcare.
Mean number of KT articles published by decade using equivalent searches across ProQuest, PubMed and Google Scholar. Search conducted Sept 17, 2016
Mean number of KT articles published by decade using equivalent searches across ProQuest, PubMed and Google Scholar. Search conducted Sept 17, 2016
Clearly, KT in the field of disability has yet to be given the widespread attention that has characterized its application in healthcare. Further, with some exceptions, attention has mainly been driven to end-use products of KT (such as informational briefs or website development) rather than to the complexities of its processes. In other words, KT has been interpreted as a one-way dissemination from researcher to audience, and, with some exceptions, has largely not been applied to describing knowledge users or knowledge-use decisions. For example, we conducted a brief examination of 44 randomly selected disability-focused articles published in peer reviewed journals during 2015 and up to August, 2016 reporting original research. An examination of the discussion and conclusion sections of these articles yielded this list of suggestions for the application of findings. (Note: each article could describe more than one suggestion.):
Engage in further research: 44 General–Building awareness: 42 Training stakeholders–New content-areas: 37 Training extended to new groups of stakeholders: 25 Create online tools or website: 30 Enhance stakeholder competence— general: 24 Training of stakeholders–Additional training: 34 Create communities of practice: 6 Provide online platforms for partnerships: 7 Build collaborations: 12 Engage professional communities: 3
Though we must recognize that researchers alone cannot be responsible for translating findings into practice, we must also recognize that these suggestions for actions will not be enough. These suggestions for actions might make sense, but they are not KT. Researchers take care to demonstrate the validity of their findings, yet they alone cannot be held responsible for “impact validity” (Massy & Barreras, 2013). Something more needs to happen.
These researcher suggestions for further actions tend (with some exceptions) to focus on approaches which are essentially passive and individualistic, based in the assumption that providing individuals with information (in the form of websites, training, briefs, webinars, presentations, or conferences) will lead to those changes needed to improve employment outcomes. Unfortunately, these passive, individualistic approaches are not supported by the research on organizational change, diversity and inclusion. Effective approaches have been found to be those that address the relational level— those seeking to change not individuals, but the larger organizational culture, climate, incentives, accountabilities, expectations and processes that make up the fabric of lived experience in the workplace (Green & Kalev, 2007; Nishii & Bruyere, 2014; Rudstam, Gower, & Cook, 2012). Impacting the relational level calls for a different type of KT based on two-way, consultative frameworks capable of encompassing context, unique stakeholder cultures and the emergent nature of organizational change. “Spray and pray” approaches, characterized by one-way communication where information is broadcast to a generalized audience, are unlikely to be effective, even when they are based on validated evidence, have been vetted by experts and edited for plain language.
Since KT was conceptualized two decades ago, a burgeoning academic conversation has continued around the challenges and dilemmas of KT as it is currently applied. This conversation has originated from many different disciplines: philosophy of science, medicine, political science, organizational development, sociology, psychology and education, to name a few. Though this conversation has mostly taken place within the healthcare arena, it has drawn from and impacted KT in other areas as well. It is outside the scope of this article to provide a comprehensive discussion of this debate. However, it is useful to outline some major themes that have recently emerged to further the discussion of KT within the field of disability and as it applies to employment.
Epistemological commitments: Questioning how evidence is legitimized
At the heart of all KT approaches is the notion of evidence-based practice (EBP). That knowledge informing practice should be based on the best-available evidence is not unique to KT (Claridge & Fabian, 2005). What is somewhat unique to KT, however, is the positioning of evidence within a larger process and the codification of a hierarchy of the legitimacy of different types of evidence (Borgerson, 2009; Goldenberg, 2009). This hierarchy positions randomized clinical trials (RCTs) and, to a lesser extent, quasi-experimental approaches as the gold standard against which all other evidence should be judged. The hierarchy of evidence has emerged mainly from the development of KT in the field of medicine, gestated by such groups as the Campbell Collaboration and the Cochrane Collaboration. Prince, (2015, p. 15) describes this hierarchy of evidence in the field of healthcare as follows:
Typically, stories or narratives from individuals or families are at the low end of the dominant hierarchy of credible evidence, followed by the opinions of stakeholder groups, evidence from a qualitative study, then evidence from a well-designed quantitative analysis, perhaps followed by a precise control trial or cohort study, and then a randomized controlled trial, culminating with a meta-analysis of all applicable evidence-based studies on a topic, group or program.
During the past two decades, there has been an energetic conversation about the automatic assumptions underlying what constitutes legitimate evidence, both within (Archibald, 2015; Scriven, 2008) and outside the scholarship of KT (Goldenberg, 2009). A core idea of this debate is that evidence is never neutral, even when presented as highly legitimized findings, such as those obtained from RCTs or quasi-experimental methods. Though the hierarchy of evidence gives the appearance of objectivity, certain voices, experiences, and events are privileged while others are rendered invisible. Hence, the term politics of evidence has been put forth to highlight how the hierarchy of evidence is rooted within and sustains a particular power structure (Archibald, 2015; Parkhurst, 2016; Foucault, 2003).
In the disability sphere, the hierarchy of evidence has been adopted and modified in several arenas, such as the Strength of Evidence scale put forth by the Center for Knowledge Translation for Disability and Rehabilitation Research (KTDRR, 2013). Yet, the debate about the hierarchy and politics of evidence has been far less lively in the field of disability than in other fields, such as healthcare, education, and organizational development.
How has the adoption of the hierarchy of evidence put forth in the healthcare sphere impacted how KT is construed in the field of disability? When answering questions such as the effectiveness of a treatment, the value of the hierarchy of evidence and the value of RCT in the healthcare arena is self evident. In healthcare, there is a clearer consensus around what a successful outcome looks like, how it can be measured and who decision gatekeepers are. In the world of disability, however, this hierarchy of evidence becomes more problematic. The use of evidence in the world of disability is more variable, complex, and specific to each stakeholder who “touches” it as it (hopefully) flows into practice. Finally, most important to the disability and employment issue, the types of evidence and the voices which might be most needed to show if/how employment outcomes come about tend to be those positioned at the bottom of this hierarchy.
The politics of evidence— use of evidence in decision-making
For the past sixty years, authors such as Hannah Arendt, Michel Foucalt and Henry Mayer have discussed how power differences have a far more complex and pervasive relationship to empirical evidence than is recognized. More recently, many authors have pointed out that the valuing of evidence is not simply a rational, academic act. It is a political act, with political commitments and consequences (see for example, Archibald, 2015; Parkhurst, 2017; Prince, 2015; Rogers, 2009). The discussion of the politics of evidence has manifested in the field of KT in three ways.
First, the term bounded rationality has been extensively used over the past three decades to question an overly rational, clean and linear view of organizational or government decision-making (see, for example, Arthur, 1994; Gigerenzer & Selten, 2001; Simon, 1978). How is evidence actually sought and used in the messiness of everyday policy-making and organization-level decision making? In real life, rational knowledge-use decisions are inevitably bound or limited by a complex set of factors: the time available to make the decision, the information on hand, limitations in understanding the information, and the decision-makers’ motivations (obvious or hidden). In the arena of disability and employment, we know very little about how bounded rationalities constrain how employer-stakeholders make decisions about acting upon knowledge as these decisions unfold in everyday life. Commonly used “needs analysis” methods (with their reliance on narrow, researcher-defined categories of inquiry, one-way communication and the failure to see knowledge-use decisions unfolding in context), cannot scrutinize bounded rationalities or capture how they are unique to each stakeholder group.
Second, the hegemony of evidence and the techno-rational approach has been debated extensively (see for example Archibald, 2015; Foucalt, 1997, Holms, Murray, Perron & Rail, 2006; Kinsella, 2007; Parkhurst, 2017; Salter & Kothari, 2016; Schon, 1987). The techno-rational approach to evidence appeals to stakeholders for obvious reasons–it yields knowledge which appears to be generalizable across time, place, and organization, and thus provides the assuredness needed to answer for public accountability. Yet, this approach, with its emphasis on program fidelity and adherence to a pre-defined sequence of events, has rendered invisible the very features of KT efforts we most need to pay attention to: the messiness of real life knowledge-use decisions, the situated (context-dependent) nature of these decisions, the power differences between actors as knowledge-use decisions unfold, and the negotiation of knowledge in an actual organizational culture and climate. Further, the techno-rational approach and its insistence on a strict view of program fidelity may tempt us to clean up the messiness too soon. This view has constrained the use of an iterative, emergent program design while privileging approaches which may move too quickly to a false consensus that fails to admit the full range of voices involved in using knowledge to bring about outcomes.
Third, the debate around the hegemony of evidence focuses not so much on the application of scientific findings, but rather on how research questions are formulated. Heisenberg stated, “What we observe is not nature itself, but nature exposed to our method of questioning” (as quoted by Archibald, 2015). Who has a voice in formulating these questions? Who is consulted? Who is not seen as being “qualified” to pose research questions? And, most importantly, who benefits and who loses from this formulation? For the most part, in fields such as healthcare, the formulation of the research question and the value of evidence is straightforward: Does a medical intervention improve patient outcomes? But in the field of disability, different stakeholder groups have widely disparate (and sometimes directly contradictory) views on what constitutes a successful outcome. Hence, the definition of what constitutes “useful” knowledge in the field of disability and employment is more likely to be unique to each stakeholder group.
These three criticisms of EBP (as well as other issues not discussed here) have been extensively debated for the past fifty years. Yet, with some exceptions (see, for example, Archibald, 2015; Lane & Rogers, 2011; Prince, 2015; Rogers, 2009), the lively reflexivity around KT and evidence that has been present in other fields (such as healthcare, education, economics and international development) has largely been absent from the debate around KT in the field of disability. This, despite the significant effort and resources expended to disseminate knowledge to stakeholders in the hopes of changing their decisions around employing people with disabilities.
De-contextualization and the need for deep descriptions of situated actions
Perhaps the most important criticism in the debate around KT is that of the need for a more nuanced and complex understanding of the real-life situations in which knowledge use decisions are made— the need for an anthropology of knowledge that can be applied to disability and employment (El-Jardali & Fadlallah, 2015; Granek & Nakash, 2016; Kitto, Sargeant, & Reeves, 2012; Lillehagen, Vøllestad, & Heggen, 2013).
These criticisms stem from questioning the very concept of knowledge. The concept of knowledge implicitly assumed in KT models is that of knowledge as an object existing more-or-less in a vacuum, apart from human consciousness or intentions. Since Berger & Luckman’s hallmark 1967 work, The Social Construction of Reality, many authors have questioned this neutral-object view of knowledge in favor of one that sees knowledge as a social construction, negotiated in a particular time and place— in a particular context. Authors such as Michel Foucalt (1997) have furthered these arguments by surfacing the subtlety of this socially mediated meaning-making and its role in maintaining unequal power relations in democratic societies. Foucalt’s phrase, the de-valuing of local knowledge, highlights how the techno-rational view of knowledge underlying the hierarchy of evidence has rendered invisible the fluid, socially negotiated meaning of knowledge— the on-the-ground situations within which decisions about acting upon knowledge are made. In other words, the real stuff of KT.
In the field of healthcare, several authors have called for a more nuanced understanding of context and situated action when applying KT models (See for example, Ferlie & Shortell, 2001; Kitto, Sargeant, & Reeves, 2012; Thomas, Menon, Boruff, Roriguez, & Ahmed, 2014). Other studies of KT in healthcare have described and examined the real-life context of unfolding KT efforts (Granek & Nakash, 2016; Lillehagen, Vøllestad, & Heggen, 2013). For these reasons, Thomas, Menon, Boruff, Roriguez, & Ahmed (2014), have called for the application of social constructivist theory to KT processes. The appeal of social constructivist theory in KT is rooted in its ability to draw attention to context— to the fluid, emergent process of negotiating situated action. Knowledge-uptake decisions are inevitably socially mediated and negotiated in-context. Without deeper descriptions of this process, our understanding of how KT works (or not) is shallow.
Though several authors in the field of healthcare have called for a deeper description of the embedding of knowledge use decisions in context, this call has largely not been put forth in the field of disability. Notable exceptions to this do exist, such as Lane & Roger’s (2011) study of knowledge value mapping (KVM), Rogers & Martin’s (2009) application of KVM to KT for accessible currency, Prince’s (2016) deeply analytic discussion of knowledge and power in the disability field, Archibald’s (2015) provocative discussion of the implicit assumptions and challenges of KT in the field of disability and Nishii & Bruyere’s (2014) case study research on organizational climate and disability inclusiveness.
However, KT, at the time of this writing, remains under-theorized in understanding how contexts unique to each stakeholder group shape their sense of “useful” knowledge and how knowledge use decisions are situated actions. Because of this under-theorization, we are faced with a black box when attempting to understand how situated actions unfold as organizations make decisions that impact the employment outcomes of individuals with disabilities. This under-theorization is fueled in part by a hierarchy of evidence which de-values the types of research that are most powerful in describing context and situated action: participatory action research, key event analysis, case study or ethnographic participant-observation. Similarly, the near sole reliance on survey research within the field of disability has resulted in an impoverished communication with action agents and knowledge users that does not admit a full description of context, the social construction of the meaning of knowledge, and the negotiated decision to act upon it.
For KT in the field of disability and employment, this means a shift away from passive KT tools (such as briefs, conference presentations, websites or webinars) and toward consulting approaches capable of actively engaging key change agents in two-way conversations. Designing and implementing these KT approaches effectively calls for a deeper understanding of context and of situated decision-making. This deep description of context and situated action has largely not been admitted in the current KT models and methods employed in the disability sphere.
The imperative of KT in the disability sphere: A deeper consideration of stakeholder worlds
Intended merely as a heuristic tool, Fig. 1 provides a profile of the KT “valence” of five major stakeholder groups who participate in the KT process for disability and employment. By “valence,” we mean the unique cultures, processes and motivations that shape each stakeholder’s potential participation in a KT process designed to enhance the employment of people with disabilities.
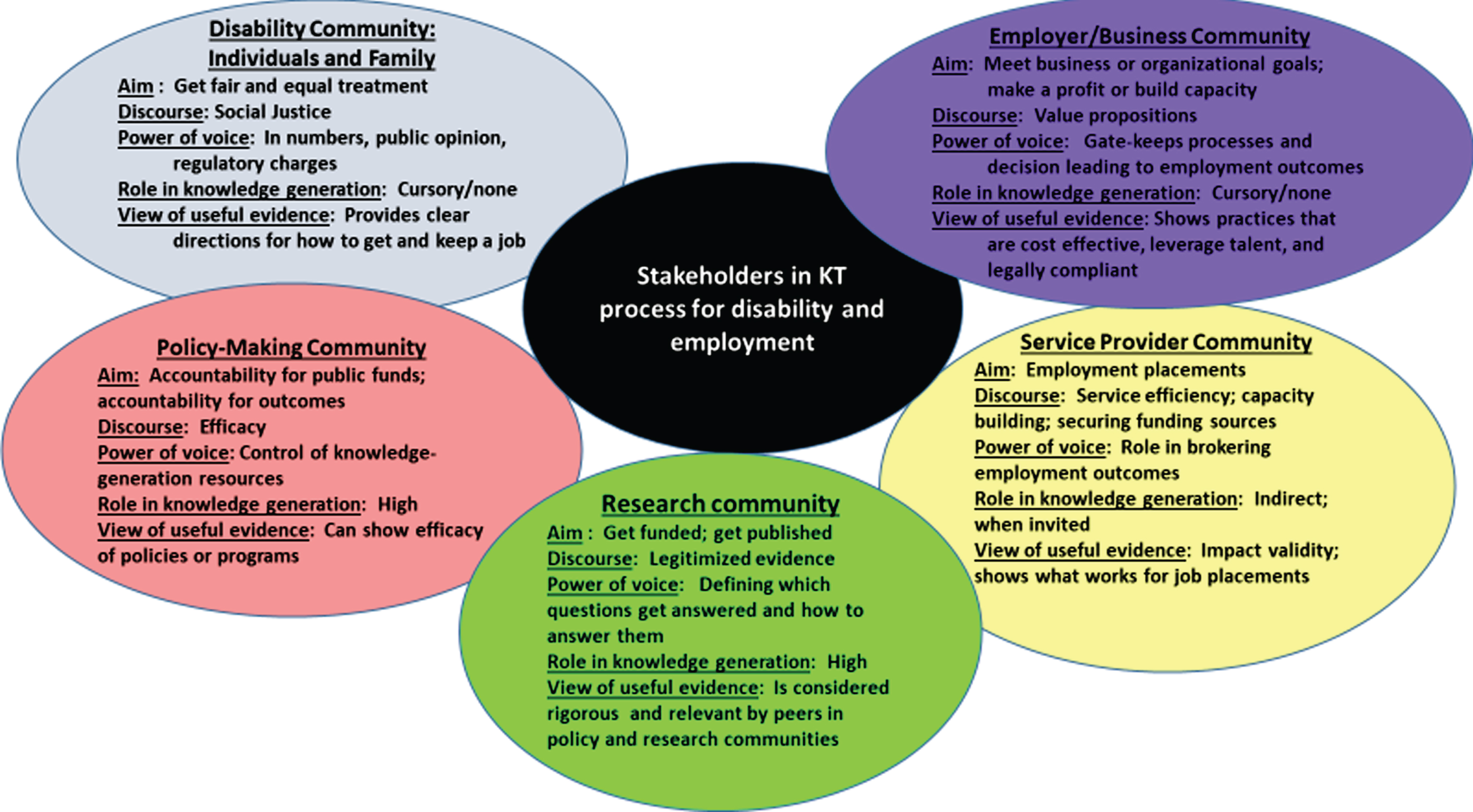
Stakeholder valence diagram: KT in disability and employment.
We have identified five components of this valence for each stakeholder group who plays a role in the employment outcomes of individuals with disabilities. Aim refers to the unique motivation for each stakeholder group. What is this group ultimately trying to achieve? What is their notion of success? Discourse refers to the orientation, stemming from their aim, that informs how this stakeholder group talks to each other— their shared sense of “what matters”? Power of voice refers to this stakeholder’s power in shaping or gatekeeping employment outcomes for people with disabilities. Role in knowledge generation refers to this stakeholder’s role in determining which questions drive knowledge generation research. Whose questions get answered? Whose do not? When determining what knowledge is needed, who is consulted? View of useful evidence refers to this stakeholder’s definition of what constitutes “legitimate” or useful evidence.
The diagram given in Fig. 1 is admittedly an over-simplification and downplays important differences within each stakeholder group. Yet, several themes come to the surface. The first is that KT in the field of disability is infinitely more complex, nuanced, divergent and convoluted than it is in healthcare. In the field of healthcare, knowledge generators (researchers) and knowledge users (healthcare practitioners), for the most part, share culture, levels of power and discourse and have consensus around what constitutes valuable evidence and a successful outcome. In the arena of disability and employment, the culture, discourse and power differences between stakeholder groups on the chain between knowledge generation, knowledge use and successful outcome is more pronounced and divergent. These stakeholders often do not share even basic aims, communication channels, views of the legitimacy of evidence, or of what counts as “useful” knowledge. Further, different stakeholders often do not share a sense of what successful outcomes look like. This makes KT fundamentally different in the sphere of disability and employment than in healthcare.
Those who are powerful gatekeepers of employment outcomes are not necessarily those who are most powerful in shaping which questions will drive knowledge generation and how these questions are answered. This gap between who shapes employment outcomes and who shapes evidence legitimacy might be one of the most challenging dilemmas facing KT in the world of disability and employment.
Originally put forth in 2006 (Graham et al., 2006), the Knowledge-to-Action Model (K2A) has been used extensively in the field of healthcare and other fields, such as human services, education and organization development (Davison, Ndumbe-Eyoh, & Clement, 2015; Field, Booth, Ilott, & Gerrish, 2014). The K2A echoes a three-step KT process that has formed the architecture of KT models since their inception. The K2A model is given in Fig. 2 below. First, during the inquiry cycle, the “knowledge funnel” coalesces and synthesizes evidence around a stakeholder’s problem. Second, the action cycle is based on planned action theory (Tiffany et al., 1994) and begins with adapting knowledge to local issues, addressing barriers to knowledge use and creating interventions. Finally, the third step of the action cycle focuses on monitoring outcomes and evaluating sustained knowledge use.
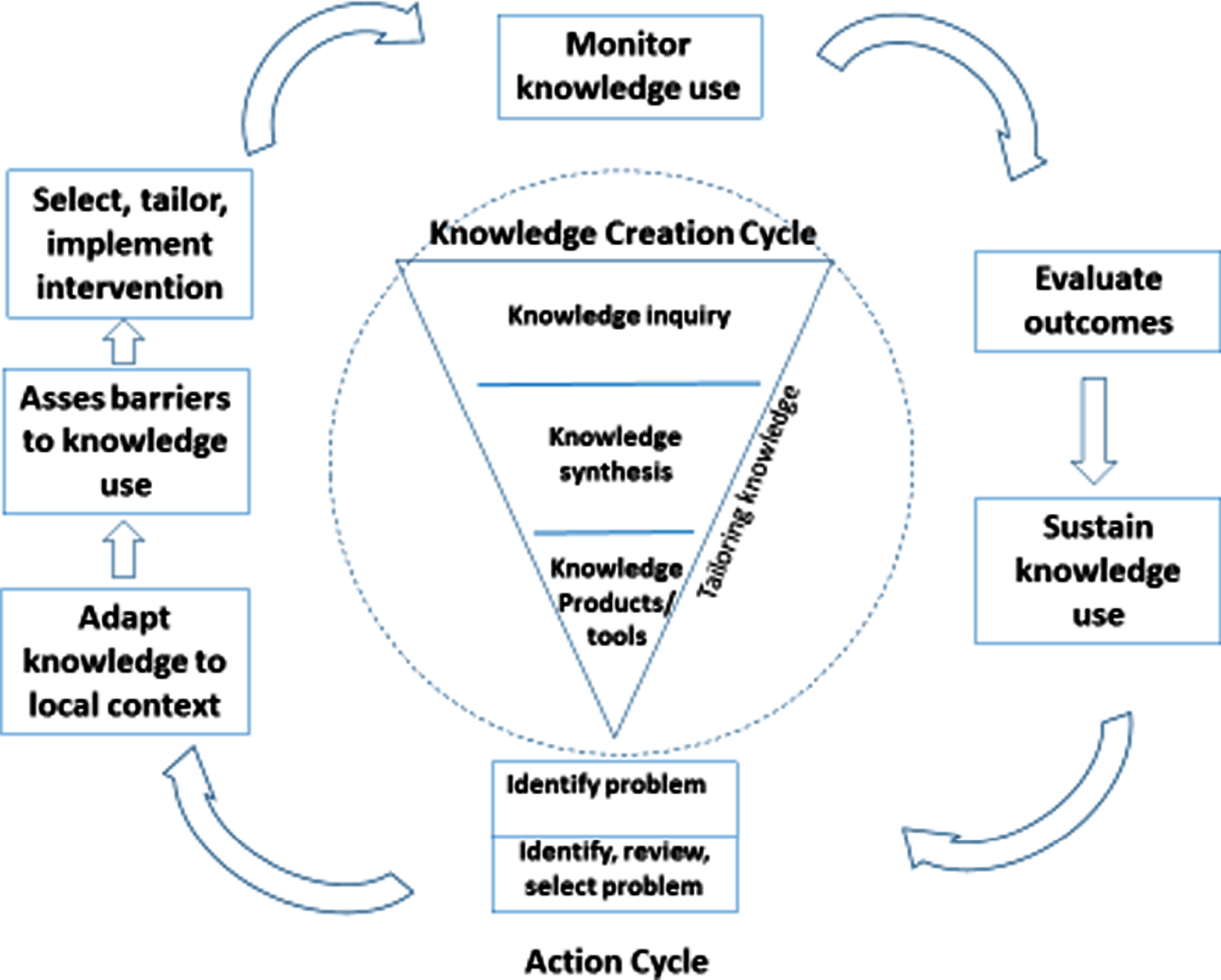
Knowledge to Action Framework. Adapted from “Lost In Knowledge Translation: Time for a Map?” by I. Graham, J. Logan, M.B. Harrison, S.E. Straus, J. Tetroe, and W. Caswel, 2006, Journal of Continuing Education in the Health Professions, 26 (1), 13-24.
Several reasons likely gave rise to the widespread use of the K2A model. It is simple to use, comprehensive, and includes the adaptation of knowledge to local issues, features which make it more generalizable outside of the healthcare arena. Given its widespread use, it is worth discussing how the K2A model might need to be adapted to the unique imperatives of KT in the disability and employment sphere. In what follows, we discuss points around applying this model given the unique imperatives of KT in the disability and employment sphere. These comments refer to the general K2A model and to its three stages: 1. The inquiry cycle (knowledge funnel), 2. The first part of the action cycle–intervention design and implementation, and 3. The second part of the action cycle— evaluation and sustaining. We begin with some general points that refer to the K2A framework as a whole before turning to a discussion of the three steps of the model.
Increased need for an emergent, iterative approach to the K2A framework
Graham et al. (2006) stressed that the steps of the K2A model are not necessarily linear and can (and often should) be iterative, fluid and permeable. In practice, however, these dynamic aspects of applying the K2A framework have tended to be dropped in favor of a more step-wise, linear approach (Archibald, 2015). This might be due to KT practitioners’ felt need for program fidelity when their efforts are reported to funding agencies, the ease in managing projects, or the wish to avoid the increased costs of changing tools or designs as the project unfolds.
Applying a social constructivist viewpoint to defining knowledge
We discussed earlier the call within the healthcare arena for a more constructivist view of knowledge (Thomas, Menon, Boruff, Roriguez, & Ahmed, 2014) and the K2A framework (Greenhalgh & Wieringa, 2011). However, there has been little attention to the need for a social constructivist theory of KT within the field of disability and employment. The widely disparate cultures and discourses among stakeholders involved in the disability field calls for a more nuanced and complex insight into how stakeholders’ decisions about acting upon knowledge are constructed in situation- and organization-specific contexts. This insight is far more important to consider for KT efforts in disability employment than for KT in other arenas. As discussed below, this affects all three steps of the K2A framework.
Enriching communication with stakeholders
Throughout the K2A framework, there is a need to re-think how the voice of stakeholders is captured and shaped at every step of the process. Though surveys make sense for some questions, the sole reliance on the survey as a means of communicating with stakeholders has resulted in a weakening of the K2A framework. Surveys are faster and less costly to administer and give the appearance of providing objective findings. Yet, survey findings (based on narrow, researcher-defined categories of inquiry, one-way communication and a selective aggregation of stakeholder voice) inevitably create an impoverished understanding of stakeholder voice. With the greater complexity and need for nuanced descriptions of context, surveys will not be enough to fuel truly effective KT efforts in the field of disability and employment.
The inquiry cycle
More involvement of stakeholders in setting research questions
Within the field of healthcare, there has been a trend toward integrated KT— KT which includes the voice of end-use stakeholders not just at the later parts of the cycle, but at the very beginning when research questions are formulated (Forin, Couture, Bouhali, Leclerc, & Stewart, 2016). As KT has been applied in disability, the voice of intended knowledge-users is usually introduced later in the KT process, such as determining knowledge channels, the packaging of knowledge or the rates of uptake of knowledge. In the realm of disability (as opposed to healthcare), the greater disparities in the culture, discourse and aims of knowledge-generators and knowledge-users enhances the need for integrated KT. Regardless of how well evidence has been validated, vetted or packaged, it is only useful if it addresses the right question. And in the realm of disability, there is less consensus around what the right question is. For example, our own recent inquiry into what types of knowledge were pivotal for employers to change their organizational practices around disability inclusiveness resulted in very different questions than those typically posed by academic researchers (Rudstam, 2014). Though no one stakeholder group should fully control the research agenda, there is a need to more cogently address pivotal questions— those questions which are most powerful in changing employer practices that can potentially change outcomes.
Variation within stakeholder groups
Another key difference between the application of K2A in healthcare vs. disability is the wider variation of roles and agents within each stakeholder group. With this variation comes the need to ask questions. Who is the knowledge-user? Who is the real decision-maker? Who is the real gatekeeper of outcomes? Our own prior research in developing an intervention to reach employers resulted in the recognition of face-to-face leaders (managers) as powerful decision-makers gatekeeping disability inclusiveness outcomes (Rudstam, Gower, & Cook, 2013). Yet, most outreach to employers is directed toward a different level of decision-maker: human resource practitioners or business leaders. Within each of the stakeholder groups identified in Fig. 1, there are multiple decision makers who broker knowledge in different ways. So, the question must be posed: Who is most critical to reach, given the practice changes that are most needed for bringing about better employment outcomes for individuals with disabilities?
Re-thinking the epistemological commitments underlying the hierarchy of evidence
By posing RCT and quasi-experimental approaches as the gold standard of evidence, the inquiry cycle of the K2A framework might dismiss the very types of evidence most needed to create powerful change— evidence based on deep descriptions of situated actions and case studies allowing for the intact description of cause-effect links.
The development of tools
The last step in the inquiry cycle involves developing KT tools/products. There is a need to question the trend in disability and employment KT efforts to create passive-use tools/products (websites, webinars, briefs or conference presentations) which then tend to become the focus of the KT effort. In this sense, there is a greater need in the disability and employment sphere to give equal attention to the later parts of the K2A model as is given to the earlier inquiry and product development steps.
The action cycle
Re-thinking barriers
The second step of the action cycle involves identifying barriers. In the field of healthcare, local constraints would tend to be issues such as the cost or time needed to implement an EBP. However, in the disability and employment sphere, as illustrated in Fig. 1, barriers can be rooted more pervasively in fundamentally different (or even contradictory) aims of the stakeholders involved in the K2A effort. These barriers require more attention and communication to overcome. Prior research in disability and employment, such as Erickson, Von Schrader, Bruyere & VanLooy (2013), Nishii & Bruyere (2014); and Von Schrader, Malzer & Bruyere (2013), can be brought to bear at this step to create a typology of barriers unique to KT in disability and employment.
Allowing for the emergent, unpredictable nature of KT implementations
Rogers (2009) has pointed out that the least predictable KT interventions tend to be those that are most effective. In disability and employment, with its greater complexity and variability in stakeholder cultures, discourses and processes, implementation is more complex and often more chaotic. A too-rigid implementation of the K2A framework during the action cycle could shut down the very phenomenon that are most important to its success: a chance for stakeholders to negotiate and re-negotiate their expectations of the process, the recognition of unexpected outcomes, or the need to re-define who the stakeholder really is.
Re-thinking outcomes
In the disability and employment sphere, outcomes are more difficult to agree upon and to capture than is the case in healthcare. Each of the five stakeholder groups described in Fig. 1 has a somewhat different notion of what a successful outcome looks like. The earlier steps in the action cycle need to include a focus on involving the end-use stakeholder in determining what “success” looks like and how it can be measured. Similarly, what is needed to measure outcomes or “success” can be different for each stakeholder group. While policy-makers, understandably, need to measure outcomes in terms of increased hiring, accommodation and sustaining of employment for people with disabilities, employers often balk at providing this data. Hence, there is a need to create and negotiate indicators which are acceptable for both policy-makers, researchers, individuals with disabilities and employers.
Conclusion
The title of this article invokes the image of a muddy river that is alive with varied and chaotic currents— a metaphor depicting a journey from the generation of knowledge to the integration of knowledge into daily practice and, finally, to outcomes. In keeping with this metaphor, we have tried to show that this river can be navigated in the sphere of disability and employment. But, for us, the currents are tricky and the journey is much longer. Boats designed for a river that flows in a straighter path with fewer currents will need to be re-fitted with a deeper keel and greater agility.
Knowledge translation and the K2A framework can be valuable in improving the employment outcomes of individuals with disabilities, but only if its cycles and steps are adapted to the greater complexity of the knowing— doing— outcomes chain within the arena of disability and employment. This adaptation will involve not only changing the steps of the model, but also achieving deeper descriptions of and richer conversations around the underlying assumptions of this framework and how these assumptions play out in the disability and employment sphere. Though we have not provided definitive answers to these dilemmas, it is our hope that we have raised more questions to broaden the conversation.
Conflict of interest
None to report.
Footnotes
Acknowledgments
The contents of this journal article were developed under a grant from the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR grant number 90DP0088). NIDILRR is a Center within the Administration for Community Living (ACL), Department of Health and Human Services (HHS). The contents of this article do not necessarily represent the policy of NIDILRR, ACL, HHS, and you should not assume endorsement by the Federal Government.