
Abstract
BACKGROUND:
Adults with a history of opioid dependence may find it difficult to gain or maintain employment. Barriers to employment include a lack of education and skills, and relapse to drug use.
OBJECTIVE:
To compare the rate of employment before, during, and after participation of detoxified opioid-dependent adults (n = 117) enrolled in a therapeutic workplace intervention and to identify predictors of post-intervention employment.
METHODS:
Analyses were conducted on self-reported employment information collected using the Addiction Severity Index-Lite and direct observation while enrolled in a model workplace intervention called the therapeutic workplace.
RESULTS:
Participants were more likely to work during the intervention (67% of days available) than before (1% of days available) or after (26% of days available) the intervention. Participants also reported working more after the intervention than before. Participants who reported working 6 months after the intervention had stronger work experience and attended the therapeutic workplace more frequently during the intervention.
CONCLUSIONS:
Given the opportunity in a model workplace, unemployed detoxified opioid-dependent adults are more likely to attend a model workplace than to work in a community job.
Introduction
In 2014, among admissions to substance abuse treatment services in the United States for any substance abuse issue, admissions were more likely to be unemployed (39.2%) or not in the labor force (36.9%) than employed (23.9%) (Substance Abuse and Mental Health Services Administration [SAMHSA], 2016). Rates of admissions that were unemployed or not in the labor force increased for admissions that were specifically for heroin abuse (42.5% of admissions were unemployed, 42.5% of admissions were not in the labor force while only 15% of admissions reported being employed; SAMSA, 2016).
Individuals with a history of substance abuse face various barriers to employment (Magura, 2003; Svikis et al., 2012) including a perceived lack of support, lack of education and training (Atkinson, Lee, Dayton-Shotts, & French, 2001), continued use or relapse to drug use (Ginexi, Foss, & Scott, 2003), low levels of interpersonal skills and computer skills (Sigurdsson, Ring, O’Reilly, & Silverman, 2012), and current enrollment in methadone programs (Richardson, Wood, Montaner, & Kerr, 2012). A lack of motivation to secure employment for individuals with a history of substance abuse may also be a barrier to employment (Zanis, Coviello, Alterman, & Appling, 2001).
To assess motivation to work as a barrier to employment for people with a history of substance abuse, Sigurdsson, DeFulio, Long, & Silverman (2011) assessed the propensity to work of individuals who had histories of unemployment and who were enrolled in a methadone maintenance program. These individuals were hired and paid to attend a model workplace intervention called the therapeutic workplace (Silverman et al., 2004; Silverman et al., 2007; Silverman, DeFulio, & Sigurdsson, 2012). Participants could attend the therapeutic workplace four hours every weekday for approximately 6 months and could earn about $10 per hour in vouchers for attendance and productivity during the training program. The study compared participant employment at three separate time points: the number of days participants reported working during the 30 days prior to being enrolled in the therapeutic workplace (intake), number of days participants worked while enrolled in the model workplace (therapeutic workplace enrollment), and number of days participants reported working in the previous 30 days during the participants’ 6-month follow-up interview (i.e., 6 months following therapeutic workplace enrollment termination; 6-month follow-up). All participants were enrolled in methadone maintenance programs and some participants were exposed to a drug abstinence reinforcement contingency in which they had to provide drug-free urine samples to maintain access to the workplace and the opportunity to earn wages.
Regardless of whether or not participants were required to provide drug-free urine samples to work, participants attended the therapeutic workplace (i.e., worked) significantly more during therapeutic workplace enrollment than they reported being employed in a community job prior to enrollment in the therapeutic workplace and 6 months after enrollment in the therapeutic workplace. Participants also reported working in a community job more at 6-month follow-up than prior to enrollment in the therapeutic workplace. These results suggest that these individuals were interested in working when given the opportunity (i.e., in the therapeutic workplace training program) and that their general failure to work in community jobs did not appear to result from a lack of motivation or propensity to work.
The current analysis extends upon Sigurdsson et al. (2011) by assessing the propensity to work among a different population of therapeutic workplace participants, detoxified opioid-dependent adults who are not interested in enrolling in opiate agonist pharmacotherapy. A major difference between the individuals in the current analysis and the individuals in the Sigurdsson et al. study is that the individuals in the current analysis did not want to enroll in opiate agonist treatment (e.g., methadone maintenance). Participants in this study also completed an opioid detoxification prior to initiating naltrexone treatment, demonstrating a substantial motivation to become opioid free. In marked contrast, all participants in the study conducted by Sigurdsson et al. were enrolled in methadone treatment, and did not need to abstain from opioids to begin treatment. The two populations are very different and may also differ in their employment outcomes. Therefore the current analysis was conducted to assess the propensity to work of opioid-dependent individuals who were not interested in opioid antagonist treatment, who completed an opioid detoxification, and who initiated naltrexone treatment. The results of the current analysis will serve to extend the propensity to work literature by assessing this distinct opioid-dependent population.
We assessed the propensity to work among individuals who participated in one of three studies designed to evaluate the effectiveness of the therapeutic workplace-training program in promoting adherence to an opioid antagonist, naltrexone, in opioid-dependent adults who had recently completed an opioid detoxification program (DeFulio et al., 2012; Dunn et al., 2013; Everly et al., 2011). Participants in these studies were invited to attend the therapeutic workplace four hours every weekday for at least 26 weeks. Similar to Sigurdsson et al., 2011, we compared rates of self-reported employment before and after participation in the therapeutic workplace to attendance in the therapeutic workplace to assess participants’ propensity to work when given the opportunity, and compared to their rates of employment in community jobs. We also assessed factors that were associated with post-intervention employment.
Method
Naltrexone adherence studies
Participants for the current analysis participated in one of three studies assessing the effect of contingent access to the therapeutic workplace on adherence to three naltrexone formulations: oral naltrexone (Dunn et al., 2013), a depot injection of Depotrex® given once every three weeks (Everly et al., 2011), and depot injection of Vivitrol® given once every four weeks (DeFulio et al., 2012). After the study was completed, Vivitrol® was approved by the FDA for the treatment of opioid dependence.
Dunn et al. (2013) assessed the effects of the therapeutic workplace intervention on adherence to oral naltrexone. Results indicated that participants in the experimental group were significantly more likely (72% compared to 21%) to provide a urine sample that tested positive for naltrexone than control group participants. However urine samples positive for cocaine and/or opiates did not differ significantly between the two groups.
Everly et al. (2011) assessed the effects of the therapeutic workplace intervention on adherence to receiving extended-release naltrexone injections. Results indicated that participants in the experimental group received significantly more depot injections than the control group (81% compared to 42%). However urine samples positive for cocaine and/or opiates did not differ significantly between the two groups.
DeFulio et al. (2012) assessed the effects of the therapeutic workplace intervention on adherence to receiving extended-release naltrexone injections. Results indicated that participants in the experimental group received all of their depot injections significantly more than the control group (74% compared to 26%). However urine samples positive for cocaine and/or opiates did not differ significantly between the two groups.
The procedures for the three studies are described in detail elsewhere (DeFulio et al., 2012; Dunn et al., 2013; Everly et al., 2011). Only procedures specific to the current analyses are described below.
Participants and setting
Employment data from participants enrolled in three randomized control studies were included in the analysis. Participants’ data were excluded if information from their 6-month follow-up assessment were incomplete. Of the 140 randomized participants in the three studies, 117 participants’ employment data were complete. Twenty-three randomized participants had incomplete or missing 6-month follow-up data and were removed. Overall, 83% of randomized participants had complete data.
Participants were recruited from detoxification centers in Baltimore, MD and reported being unemployed. A complete list of eligibility criteria for each study can be found elsewhere (DeFulio et al., 2012; Dunn et al., 2013; Everly et al., 2011). Participants were invited to attend the therapeutic workplace training program for an induction period during which they were required to take oral naltrexone to gain access to the workplace. Participants who completed the induction period were invited to attend the therapeutic workplace training program for 26 weeks. The therapeutic workplace training program intervention attempts to address the interrelated issues of drug abuse and poverty through contingency management procedures. Specifically, access to work in a model work environment, and thus the opportunity for remuneration, are contingent upon meeting one or more specified criteria (e.g., providing a urine sample, maintaining drug abstinence, adhering to medication). The intervention has two phases, a training phase and an employment phase (Silverman, 2004). Participants in the current analysis were enrolled in the six-month training phase then discharged. This is because the primary purpose of the main studies was to evaluate the effects of contingencies on natlrexone adherence. Studies establishing the importance and effectiveness of the employment phase were conducted earlier (Aklin et al., 2014; DeFulio et al., 2009).
Participants were able to attend the workplace 5 days a week for 4 hours a day and earn approximately $10 per hour; $8 per hour in base pay for attendance and $2 per hour in productivity pay. Over 26 weeks following the induction period, participants could earn a total of $5,200 in vouchers. To earn vouchers, participants could attend the workplace and engage in typing and keypad training, and complete math training.
After completing the induction period, participants in all three studies were randomly assigned to contingency and prescription groups. Participants in the prescription groups were offered prescriptions for naltrexone but did not have to take the medication in order to work. Participants in the contingency groups had to take scheduled doses of oral (Dunn et al., 2013) or extended-release injections (DeFulio et al., 2012; Everly et al., 2011) of naltrexone to gain access to the model workplace and to maintain maximum base pay. If a participant in the contingency group failed to take a scheduled dose of naltrexone, the participant was not allowed to work and the participant’s base pay was reset from $8 per hour to $1 per hour. Once the participant took the scheduled dose of naltrexone again, the participant’s base pay was increased by $1 per hour every day that the participant took the scheduled dose of naltrexone and worked for at least 5 minutes in the therapeutic workplace. Prior to study discharge, participants were offered referrals to employment services in the community.
Measures
Employment at intake and 6-month follow-up
Employment data collected at intake and 6-month follow-up assessment were obtained via the Addiction Severity Index Lite (ASI-Lite Version; McLellan et al., 1985). Information collected with the ASI-Lite Employment section included education completed, duration of longest job, type of job, employment patterns in the previous three years, and money earned from employment in the past 30 days. Employment data were obtained from participant’s answer to the question, “How many days were you paid for working in the past 30 days?” Data are reported as the percentage of the month worked. Days available to work were capped at 20 days (i.e., 20 days worked in a month was recorded as 100% of month worked). This was done in order facilitate comparison with days worked at the therapeutic workplace (see below), which was also capped at 20 days per month.
Therapeutic workplace attendance
Similar to Sigurdsson et al. (2011), days worked while enrolled at the therapeutic workplace was determined by adding the total number of days that a participant was recorded as attending the workplace for more than 15 minutes. Attendance data were collected for the first 120 available workdays following a participant’s random assignment to study condition.
The percentage of days worked during the intervention was determined by dividing the number of days a participant worked in the therapeutic workplace for more than 15 minutes by 120. This yielded the percentage worked during the 6-month intervention. For example, if a participant had worked for more than 15 minutes on 78 days in the therapeutic workplace, they were recorded as working for 65%. If a participant did not attend the therapeutic workplace for any reason including attrition or finding an actual job, their attendance data were still determined using this formula.
Employment-related demographics
Data from the ASI-Lite and the Wide Range Achievement test were collected to assess for potential differences between participants who did and did not report working at all during the 6-month follow-up assessment. Data from the ASI-Lite included age, if the participants reported receiving any vocational training in their lifetime, whether participants reported working at least one continuous year in their lifetime, whether participants reported being usually (more than half of the time) employed in the past 3 years, whether participants reported having graduated high school or earned a GED, whether participants reported ever being convicted of a crime in their lifetime, the number of convictions participants reported in their lifetime, and whether participants reported being incarcerated for at least 1 year of their lifetime. Participants’ standard scores on reading, spelling, and math from the Wide Range Achievement Test (WRAT-3 or WRAT-4; Wilkinson, 1993) were also collected.
Drug use
Drug use data were collected to assess for differences between individuals who reported working and did not report working at the 6-month follow-up assessment. Use of opiates and cocaine was determined by urine samples that were provided during the 6-month follow-up and from self-reported use in the previous 30 days collected in the ASI-Lite.
Analytic method
Kruskal-Wallis and Mann-Whitney U tests were used to compare the percentage of days worked at intake, during the intervention, and at follow-up across the three trials and between the prescription and contingency groups, respectively. These analyses showed no significant differences at any time point. Therefore, all subsequent analyses were collapsed across trials and groups.
The percentage of days worked was compared between intake, during the intervention, and at 6-month follow-up using Friedman’s ANOVA with post-hoc tests. To determine whether education, work, and legal demographics collected at intake for each trial were associated with work after the intervention, we used chi-square and Mann-Whitney U tests. The same approach was used to examine whether percentage of days worked during the intervention was associated with reporting working during the 6-month follow-up assessment. This approach was also used to determine if urinalysis results and self-reported use of opioids and cocaine at the 6-month follow-up assessment were associated with reporting working during the 6-month follow-up assessment. All comparisons were made between participants who worked at least one day at follow-up and those who did not. Analyses were conducted on all 117 participants, except where noted.
Results
Education, work, and legal demographics collected at intake are shown in Table 1. Roughly 40% of participants had not completed high school or earned a GED, over two-thirds had not received vocational training, and performance in core skills areas (math, reading, and spelling) was poor. Nearly all participants had held a job continuously for at least one year during their lifetime, typically in semi-skilled or unskilled positions, but most had been unemployed for most of the past three years. Most participants had legal histories with multiple convictions and incarcerations, often lasting more than one year.
Education, work, and legal demographics for all participants (N = 117)
Education, work, and legal demographics for all participants (N = 117)
Grade level equivalence was estimated using the WRAT. All other data are from the Employment and Legal sections of the ASI-Lite. aCalculated only for those who reported ever receiving any vocational training (N = 37). bCalculated only for those who reported work history (N = 116).
Figure 1 shows that the percentage of days worked before, during, and after the intervention were significantly different (χ2[2] = 142.49, p < 0.001). Compared to the 30 days prior to intake (M = 1.15 [9.41]), participants worked a significantly greater percentage of days during the therapeutic workplace intervention (M [SD] = 67.36 [25.57]; z = – 9.31, p < 0.001) and during the 30 days prior to the 6-month follow-up (M [SD] = 26.71 [41.87]; z = –5.50, p < 0.001). Percentage of days worked during the 30 days prior to the 6-month follow-up was significantly lower than during the therapeutic workplace intervention (z = –7.39, p < 0.001).
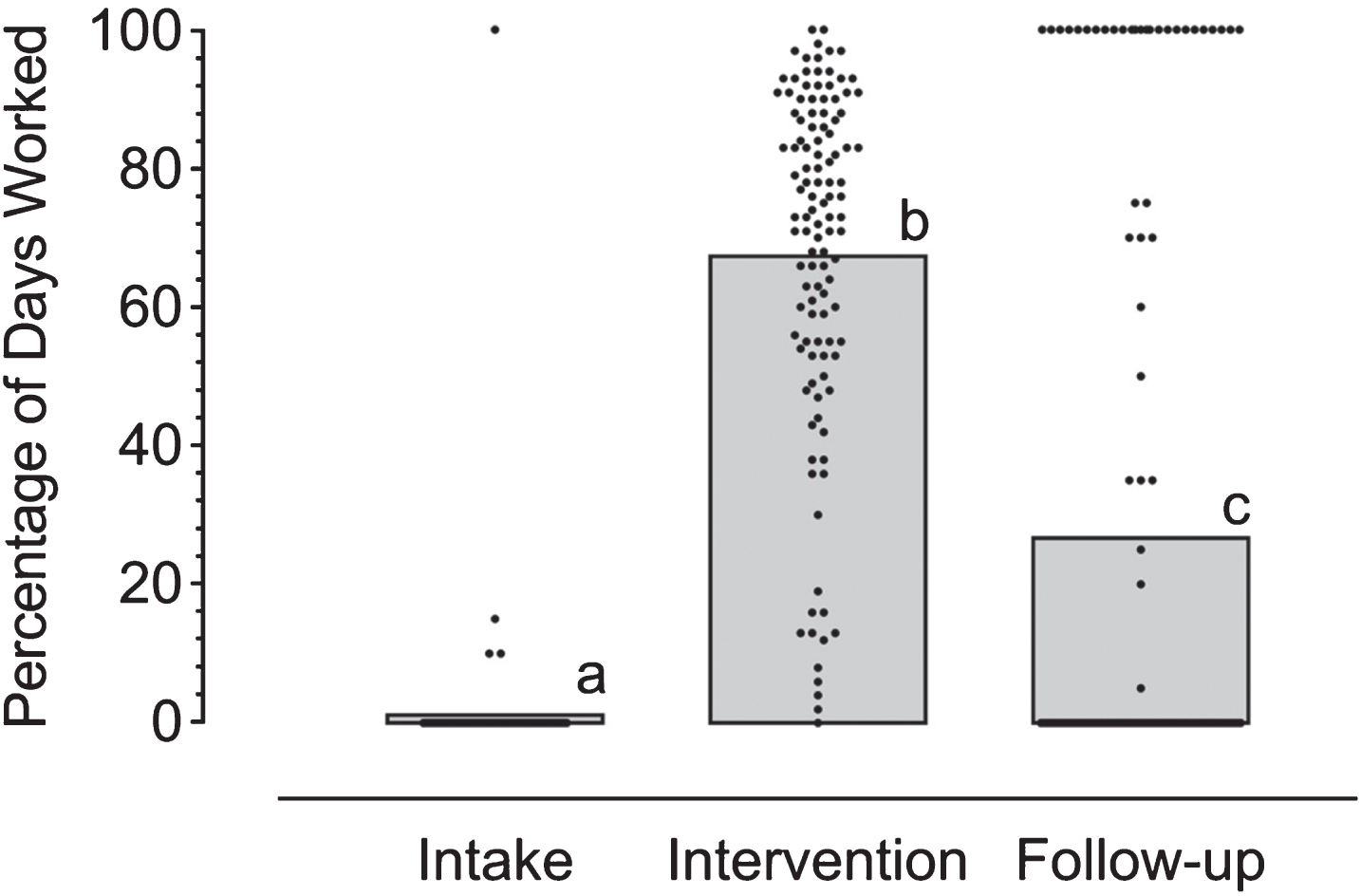
Percentage of days that participants worked during the 30 days prior to intake (Intake), during the 26 weeks in the therapeutic workplace (Intervention), and during the 30 days prior to the 6-month follow-up assessment (Follow-up). Percentage of days worked are shown for each participant at each time point. Dots represent individual participants, and bars represent the mean for all participants within a time point. Many participants reported working 0 days at Intake (N = 113) and 0 days at Follow-up (N = 79), so that dots at 0 days for those time points overlap. Means with different letters were significantly different from one another (p < 0.001).
No education or legal demographics measured at intake were associated with working at least one day in the prior 30 days before the 6-month follow-up (see Table 2). However, several employment demographics were associated with working at follow-up. Participants with strong employment histories prior to intake were more likely to report working at the follow-up. Specifically, participants who reported working at follow-up had longer durations of holding a job, were more likely to have held a job for at least one year, and were more likely to report their typical employment pattern in the past three years as employed. Self-reported drug use and urinalysis results collected at the 6-month follow-up were not associated with working at follow up.
Comparisons of education, work, and legal demographics collected at intake and time worked during the intervention by whether participants reported working at least one day during the 30 days prior to the 6-month follow-up
aCalculated only for those who reported ever receiving any vocational training (N = 37). bCalculated only for those who reported being incarcerated in their lifetime (N = 93). cCalculated only for those who reported usual employment (N = 78). dCalculated only for those who had a reading grade equivalent (N = 37). eCalculated only for those who had a spelling grade equivalent (N = 37). fCalculated only for those who had a math grade equivalent (N = 37). gCalculated only for those who had a math grade equivalent (N = 78).
The percentage of days worked during the 26-week therapeutic workplace intervention was associated with whether participants reported at least one day of work during the 30 days prior to the 6-month follow-up. Participants who reported working at least one day at follow-up worked significantly more during the intervention than those who did not report working at follow-up (see Fig. 2).
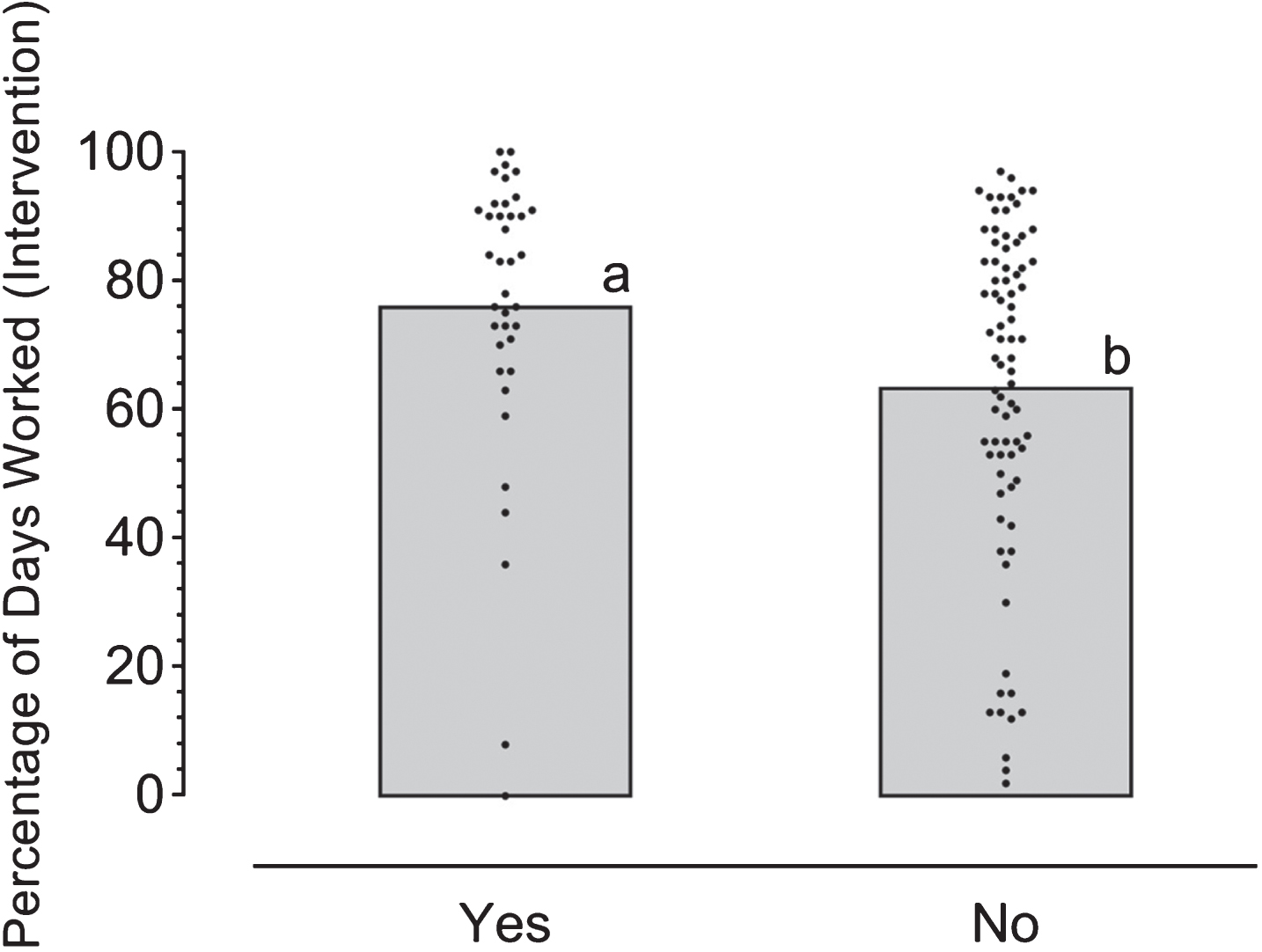
Percentage of days worked during the intervention by whether participants reported working at least one day during the 30-day period before the 6-month follow-up. Percentage of days worked are shown for each participant. Dots represent individual participants, and bars represent the mean for all participants within the category. Means with different letters were significantly different from one another (p = 0.004).
Detoxified opioid-dependent adults attended the therapeutic workplace significantly more than they reported working in the 30 days before enrolling in the study and the 30 days before the 6-month follow-up assessment. Participants attended the workplace 67% of the days available while enrolled in the therapeutic workplace, but they only reported working 1% of the days before intake into the therapeutic workplace and 26% of the days available at the 6-month follow-up assessment. Participants worked regardless of group assignment (prescription or contingency). This suggests some detoxified opioid-dependent individuals may have a propensity to work (i.e., attend a model workplace) even if there are additional requirements contingent on their workplace access (i.e., naltrexone adherence). These results are similar to Sigurdsson et al. (2011) in that, like individuals enrolled in methadone maintenance, most detoxified opioid-dependent adults will work if given the opportunity.
The proportion of days that participants worked at the six-month follow-up time point was significantly and substantially greater than the proportion of days that participants worked prior to the intervention. However considering an inclusion criterion of the therapeutic workplace intervention was to be unemployed in the previous 30 days, these results should be interpreted cautiously. Twenty-one percent of all participants reported working full time (i.e., at least 20 days in the month prior) at the 6-month follow up assessment.
Demographic data obtained prior to therapeutic workplace enrollment suggest that participants were more likely to have a job at follow-up if they reported a stronger work history (i.e., reported working at least one year of their life and reported working more than not working in the previous 3 years). These results could be used to shape vocational training that occurs during or following opioid dependence treatment, specifically for individuals with minimal work experience. Although little can be done to improve an individual’s work history, these individuals could be identified and receive increased training if needed. It may be that certain employers value work history more than other factors of employee history (e.g., education completed or legal history). However more research is needed to understand employer’s hiring patterns before that can be determined.
While the increase in workplace attendance results during the therapeutic workplace intervention are encouraging, a limitation should be noted about the use of different measurement procedures for employment data. Employment data for intake and 6-month follow-up were obtained via participant self-report, whereas employment in the therapeutic workplace was measured by attendance.
Understanding barriers to employment that opioid-dependent adults face can help enhance opioid treatment and vocational training programs. These results suggest that, given the opportunity, unemployed detoxified opioid dependent adults will work. We do not know why this population achieves low levels of employment in community jobs; however, the data from this study suggests that they have a relatively high propensity to work when given the opportunity.
Author note
Brandon M. Ring and Anthony DeFulio are now affiliated with Western Michigan University; Sigurdur Oli Sigurdsson is now affiliated with the Icelandic Centre for Research.
Conflict of interest
None to report.
Footnotes
Acknowledgments
The authors would like to thank Heather M. McGee, Ph.D. for her comments on an earlier version of this manuscript. The research was supported by grants R01DA019497, R01 DA019386, R01 DA037314, and T32DA07209 from the National Institute on Drug Abuse. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Drug Abuse or the National Institutes of Health.