
Abstract
BACKGROUND:
There is a growing interest among policymakers in improving the delivery of vocational rehabilitation programs to Social Security Disability (SSD) beneficiaries. To advance these efforts, policy makers must understand what prevents beneficiaries from returning to work.
OBJECTIVE:
This paper investigates the relationship between functional limitations and employment among SSD beneficiaries with musculoskeletal (MSK) conditions. Drawing from the ICF model of disability, we hypothesize that functional limitations mediate the pathway between the musculoskeletal condition and employment.
METHODS:
We use a nationally representative sample of SSD beneficiaries from the National Beneficiary Survey. We explore the relationships between health conditions, functional limitations, and employment in a multivariate mediation analysis.
RESULTS:
Mediation effects are statistically significant at the 5 percent level. We estimate that pain mediates over 50 percent of the direct effect of an MSK condition. Lower body, mobility, and upper body limitations mediate 22, 18, and 10 percent of the direct effect of an MSK condition, respectively.
CONCLUSIONS:
Functional limitations, in particular experiencing moderate to severe pain, mediate the relationship between the MSK condition and employment among SSD beneficiaries. Addressing these functional limitations may be of first order importance in enabling employment for the MSK population.
Introduction
Return to employment after a disabling event is seen as a primary goal of many actors in the disability system, including the person with a disability, the employer, and the various health and employment support providers. While employment after disability can have many positive effects including economic independence and improvement in overall wellbeing (Waddell & Burton, 2006), the extent and type of work that an individual is able to do depends on their functional capacity. Measuring functional capacity provides a practical way to measure how a disability manifests itself in an individual’s daily life and can provide vocational rehabilitation (VR) professionals and the individual with a disability with information to identify effective therapies, treatments, and appropriate employment opportunities (Mitchell, 2008).
Assessing functional capacity could be particularly important for understanding the employment potential of Social Security Disability Insurance and Supplemental Security Income (hereafter, SSD) beneficiaries in the United States. Prior research on the employment of SSD beneficiaries has concentrated on a variety of attributes and behaviors that make beneficiaries more or less likely to engage in paid work. Research has explored how the employment of beneficiaries varies according to demographic characteristics and geographic locations (Mamum, O’Leary, Wittenburg, & Gregory, 2011; Ben-Shalom & Mamum, 2013), participation in return to work programs (Ben-Shalom & Stapleton, 2015), the work related goals and expectations of beneficiaries (Livermore, 2011), and the specific kinds of health conditions beneficiaries report (Von Wachter, Manchester, & Song, 2011; Mann, Mamum, & Hemmeter, 2015). However, little work has analyzed the relationship between the functional limitations of beneficiaries and their work-capacity. Contemporary theories of disability, including the International Classification of Functioning, Disability and Health (ICF) model developed by the World Health Organization, suggest that functional information can provide a more direct indication of the barriers a person with disabilities experiences than other characteristics, such as the specific health condition (WHO, 2001; Brandt, Houtenville, Huyunh, Chan, & Rasch 2011).
Disability benefit programs provide income replacements to those unable to work due to a work-limiting medical impairment. There is a growing interest among policy makers in the US to improve the delivery of VR services to SSD beneficiaries. The Social Security Administration (SSA) has adopted several policy initiatives for SSD recipients to return to employment. These initiatives include the Ticket to Work program, a voluntary VR program, as well as several demonstration projects intended to assist beneficiaries in their return to employment (SSA, 2017). Special rules, moreover, allow those receiving SSD benefits to test their ability to work while still receiving payments and access to health insurance for a period of time (SSA, 2017). To advance these efforts and improve employment outcomes, policy makers need to understand what prevents SSD beneficiaries from returning to work. Information on functional limitations could help improve the design and delivery of employment services to people with disabilities receiving SSD benefits.
In this study, we build upon prior research to investigate the relationship between the functional limitations of SSD beneficiaries and their employment outcomes. We hypothesize that functional limitations mediate the association between health conditions and employment outcomes. To explore this process, we limit our analysis to SSD beneficiaries with musculoskeletal (MSK) conditions. The number of SSD beneficiaries with MSK conditions program has more than quadrupled since 1981 (Anand & Ben Shalom, 2017). Beneficiaries with MSK conditions further report some of the lowest employment rates among SSD beneficiaries with just 8.7 percent employed in 2011 (Mann et al., 2015). Reducing inflow rates from individuals with MSK is thus a major focus of reintegration efforts and policy makers have a considerable interest in understanding the underlying processes leading to the low employment outcomes among this population. Focusing our analysis on beneficiaries with MSK conditions further provides an ideal case study for investigating our hypothesis. In what follows, we first develop a theoretical model of how functional limitations influence employment outcomes of SSD beneficiaries with MSK conditions and provide our research hypotheses. We then present our data and methods. This is followed with a discussion of the results and with an analysis of barriers to employment. We conclude with a discussion of policy and practice implications.
The ICF framework
The ICF is a framework that provides a common conceptual basis for defining health and disability across countries and has been described as a “paradigm shift” in the measurement of disability (Kostanjsek, 2011). The ICF views disability as a dynamic interaction between an individual’s health and the environmental factors that limit an individual’s ability to achieve their desired level of participation in society (WHO, 2001). We apply three key ICF concepts of functioning in this paper in the context of an MSK disorder or disease (see, WHO, 2001; Stapleton, Protik, & Stone, 2008). The first concept is an impairment, which is defined as problems of body structure and function. Impairments include sensory impairments (i.e. difficulty hearing or seeing or experiencing pain), mental impairments (i.e. difficulty learning and concentration), and physical impairments (i.e. difficulty bending and walking). The second concept is activity limitations, which refer to difficulty achieving daily activities, such as dressing, bathing, and using the toilet. The third concept refers to participation restrictions, which is defined as problems experiencing involvement in life situations, such as engaging in paid work or in domestic life. Though all three concepts are viewed under the broader umbrella of functioning in the ICF model, for this paper we refer to the first two concepts (impairments and activity restrictions) as functional limitations. And, because we are focused on the role of employment, we will refer to the third concept (participation restrictions) as work-disability.
The ICF model does not view these categories as necessarily progressing from one to the other (i.e. from a health condition to functional limitations to work-disability). A work-disability could result, for example, not from a functional limitation but from the experience of discrimination in a social context (i.e. an individual with HIV who has no functional limitations but is discriminated against at work). Yet, with this caveat in mind, we suspect that for many who experience health conditions it is the functional limitation, and not necessarily the health condition, that leads to work-disability or the inability to work. Some with MSK disorders, for example, will be more likely to experience functional limitations than others, and this variation may be attributed to their individual condition, as well as to the accommodations available to them in the working environments.
Functional limitations and the employment of SSD beneficiaries
Prior research indicates that SSD beneficiaries of younger age, with low-mortality health conditions, and/or who receive benefits later in the determination process are more likely to maintain an ability to work (von Wachter et al., 2011; Maestas et al., 2013; Mann et al., 2015). But little is known about the relationship between the functional limitations of beneficiaries and their employment outcomes. This information could help to account for the wide spectrum of employment ability that exists across SSD beneficiaries. Mann and colleagues (2015) provide a detailed examination of the employment and earnings of beneficiaries from twenty-five health conditions and show that specific impairment groups, such as those with intellectual disabilities or HIV/AIDS, were the most likely to be employed, while individuals with affective disorders, schizoaffective disorders, and MSK disorders were the least likely to be employed. They ultimately call for research that can illuminate “the underlying causes of different earnings patterns across impairment types,” (Mann et al., 2015:32). In this paper, we investigate whether health conditions lead to diverse functional limitations and examine the extent to which accounting for these functional limitations may explain why most SSD beneficiaries with MSK conditions are unlikely to work.
Methods
Data
We draw on the National Beneficiary Survey (NBS). The NBS provides a nationally representative sample of SSD beneficiaries. The survey was designed to collect information to evaluate the SSA’s Ticket to Work program and thus collects a wealth of information on SSD beneficiaries to complement administrative records, including data on the health, human capital, employment behaviors, awareness of services, barriers to work, and functional limitations of beneficiaries. The NBS has so-far collected five cross-sectional national surveys (2004, 2005, 2006, 2010 and 2015) of SSD beneficiaries age 18 to full retirement, with additional survey rounds planned in the future. For all survey waves, the NBS uses a multistage sampling design. Data provided from the SSA on the number of eligible beneficiaries in each county formed the primary sampling units, which consisted of one or more counties. Computer-assisted telephone interviewing and computer assisted personal interviewing were used for those who prefer or require an in-person survey. Further information about the public-use data files used in this analysis can be found in Wright et al. (2012) and additional information on the imputation and weighting procedures can be found in Grau et al. (2012). We pull together data across the five survey waves and create an analytic sample of SSD recipients that consists of 20,252 beneficiaries. We present descriptive statistics on beneficiaries’ demographic characteristics and employment and provide descriptive data on the reported reasons for not working provided by beneficiaries with MSK conditions and compare them with those beneficiaries without these conditions. Throughout the analysis we utilize survey weights to maintain the representative nature of the sample.
Definition of functional limitations and other variables
The outcome variable in our analyses consists of whether a respondent is currently working. Current rules allow SSD benefit recipients to work under specified amounts without losing access to medical or benefits. For additional details on the work rules regarding benefit recipients, which vary for SSI and DI beneficiaries, see SSA (2018). We thus follow past research which uses employment as a general indicator of a beneficiary’s potential work-capacity (Mann et al., 2015). The primary health conditions of interest are MSK conditions. We identify a variety of questions relating to functional limitations in the NBS that could serve as potential mediators of the relationship between MSK conditions and employment. We first mapped all the questions concerning functional limitations in the NBS into the three main categories of impairments in the ICF as described above (e.g., sensory impairment, physical impairments and mental impairments). We focus our analyses here primarily on physical impairments, which included difficulty walking a quarter mile at all, unable to lift 10 pounds at all, unable to stoop at all, unable to climb 10 steps at all, cannot move between seated positions, cannot raise arm, and difficulties with manual dexterity. Then, we collapsed these limitations into three categories which included mobility limitations (comprised of difficulty walking and unable to climb steps), lower body limitations (unable to stoop and unable to move between seated positions), and upper body limitations (unable to lift 10 points, cannot raise arm, issues with manual dexterity). We additionally consider one key sensory impairment of whether an individual has experienced moderate to severe pain over the last 4 weeks. We also include baseline characteristics of beneficiary demographics. These include age, sex, and whether the respondent reports an income above of the federal poverty line or 200% above the federal poverty line, and type of SSD benefit received (SSI, SSDI, or concurrent). We also include a variable for education (high school degree) and a variable for racial and ethnic status (non-white).
Statistical analysis
The objective of this analysis is to examine the process in which functional limitation variables may mediate the relationship between the MSK condition and employment outcomes among SSD beneficiaries. Figure 1 provides the diagram used in our analysis based on ICF notions of disability. This model anticipates that, after controlling for the personal characteristics of beneficiaries, having an MSK condition will reduce the likelihood of employment among SSD beneficiaries, as shown in previous literature and demonstrated in the C pathway. The main hypothesis of this study is that functional limitations will mediate the pathway between the MSK condition and employment outcomes via the A and B pathways.
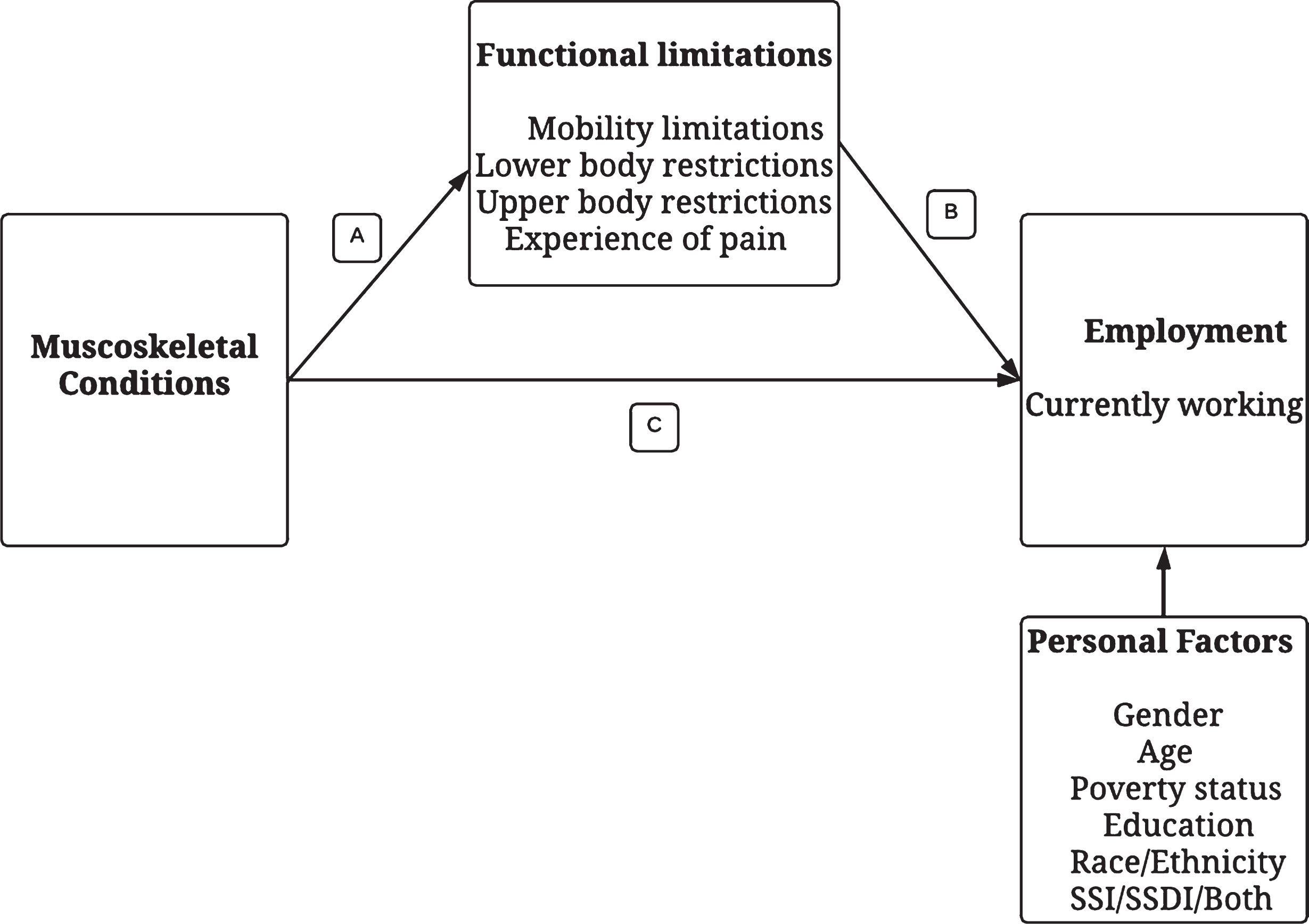
ICF based model of the relationship between MSK condition, functional limitations, and employment outcomes.
We begin by exploring the mediation hypothesis using logistic regression. We first test the association between reporting an MSK condition and employment, adjusting for the personal characteristics described above, and wave specific fixed effects to control for systematic variation in responses across survey waves or over time. We then compare the change in the magnitude of the coefficient for MSK conditions when adding the mediating factors into the model. We first add mobility limitations, then lower body limitations, upper body limitations, and finally experiencing moderate to severe pain.
We next explore the results using a formal mediation analysis technique for nonlinear models that is implemented with the Stata command medeff (Hicks & Tingley, 2011). The command operates in two phases. First, it runs two regression models: one that explores the relationship between the single mediator variable (a specific functional limitation) and the primary independent variable (MSK condition), and a second regression exploring the relationship between the outcome variable (whether the respondent is working) and both the independent variable and mediating variable. Both regressions are adjusted with the same set of covariates. Random samples of the data are drawn and this exercise is repeated one thousand times within a Monte-Carlo simulation. The resulting estimates are then aggregated to obtain 95 percent confidence intervals around an estimate of the average direct effect (pathway C in Fig. 1), the average indirect effect (pathway A-B in Fig. 1), and the percent mediated (ratio of indirect/total effect) (Imai, Keele, Tingley, 2010; Garawi et al., 2015). If the direct effect is found to be zero after accounting for the mediator, then this suggests a total mediation effect. If the mediator variable is significant and the direct effect is reduced but still significantly different from zero, this implies a partial mediation effect. This approach has been used to study, among other things, the relationship between self-efficacy on employment (Umucu et al., 2016), the relationship between stressful work on health (Hoven et al., 2015, Reinhardt et al., 2013), and the relationship between lower body impairments and participation in life activities (Beauchamp et al., 2016).
Demographic and employment characteristics of SSD beneficiaries with MSK conditions
Table 1 provides the employment rates by the primary health conditions reported in the NBS. We see that SSD beneficiaries with primary MSK conditions have the lowest reported employment rates, with just 5 percent currently working, compared to 9 percent of individuals with a primary mental condition, 14 percent among individuals with a primary sensory condition, and 20 percent among individuals with a primary cognitive condition. Table 2 compares the demographic and health characteristics by primary reported condition. The table shows that those with MSK conditions are more likely to be female, of older age, married, without a high-school degree, and they are less likely to be in poverty. Those with MSK conditions are also significantly more likely to report functional limitations of mobility, lower and upper body, and moderate to severe pain.
Employment Rates by Primary Condition Reported in NBS
Employment Rates by Primary Condition Reported in NBS
Notes: Data from all five rounds of the National Beneficiary Survey. Statistics calculated with respondent weights, rescaled to maintain the proportion of respondents in each wave of the survey.
Characteristics by Primary Reported Condition
Notes: Data from all five rounds of the National Beneficiary Survey. Statistics calculated with respondent weights, rescaled to maintain the proportion of respondents in each wave of the survey. P-values test equality of means between respondents with and without musculoskeletal impairments as a primary condition.
In Table 3, we provide the reported reasons for not working provided by beneficiaries with MSK conditions compared to beneficiaries without these conditions. Given that beneficiaries have already been found incapable of substantial gainful activity, it is not surprising that nearly all report their physical condition as the primary barrier to their work. It is of interest, however, that those with MSK conditions report fewer environmental barriers to employment (i.e. transportation, accessibility, discrimination) than those without MSK conditions. These results could indicate that interventions specifically targeted at stabilizing and improving beneficiaries’ physical health could be of first order importance to improving employment outcomes. Strategies designed to eliminate environmental barriers may be more effective after first mitigating the impacts of beneficiaries’ physical conditions on daily life and functioning. This underlies the importance of understanding the process in which an MSK condition translates into lower employment outcomes, as explored in the mediation analysis.
Reported Reasons why Not Working, by Primary Reported Condition
Reported Reasons why Not Working, by Primary Reported Condition
Notes: Data from all five rounds of the National Beneficiary Survey. Statistics calculated with respondent weights, rescaled to maintain the proportion of respondents in each wave of the survey. P-values test equality of means between respondents with and without musculoskeletal impairments as a primary condition.
The logistic regression results are presented in Tables 4 and 5. Table 4 first examines the relationship between having a primary MSK condition and each of the four main functional limitations examined here. Each column indicates that there is a positive and significant relationship between having a primary MSK condition and reporting each of the functional limitations. The relationship is strongest for experiencing moderate to severe pain, with an average marginal effect of 0.312. These positive and significant correlations are an important first validation check to assess the extent to which the functional limitations could serve as potential mediators of the effect of an MSK condition.
Correlation between Musculoskeletal Primary Condition and Physical Functional Limitations
Correlation between Musculoskeletal Primary Condition and Physical Functional Limitations
Notes: Coefficients shown are average marginal effects from a logistic regression model where the dependent variable is an indicator for having the functional limitation reported in the column header. All models control for the demographic characteristics reported in Table 2 and include wave specific dummies. Coefficients are not included here for the sake of brevity. Full results available on request. Data included from all five rounds of the National Beneficiary Survey. Regressions conducted with respondent weights. Robust standard errors in parentheses. **p < 0.01, *p < 0.05, +p < 0.1.
Impact of Functional Criteria on the Probability of Working (Dependent variable = 1 if respondent is working)
Notes: Coefficients shown are average marginal effects from a logistic regression model where the dependent variable is an indicator for whether the survey respondent is currently working. Data included from all five rounds of the National Beneficiary Survey. Regressions conducted with respondent weights. Robust standard errors in parentheses. **p < 0.01, *p < 0.05, +p < 0.1.
Next, Table 5 examines the relationship between the MSK condition and employment, and then sequentially adds each of the potential mediating factors one by one. All baseline characteristics are statistically significant predictors of work status among SSD beneficiaries in the baseline model. The magnitude and significance of the coefficients implies that beneficiaries who have lower household incomes, lower education, are non-white and those who receive SSI are all to less likely to work. Younger beneficiaries have a higher propensity to work than older beneficiaries, and individuals who are overweight also have a higher propensity to work. The significance of majority of these coefficients persists as we add each potential mediator to the logistic regression. The coefficient on having a primary MSK condition is negative and significant in the baseline model, reflecting that MSK beneficiaries are less likely to be working than SSD beneficiaries with other primary conditions, even after conditioning on the personal factors described here. We further observe that each functional limitation has a negative and significant coefficient when added to the model. With the exception of the inclusion of moderate to severe pain, the MSK coefficient remains negative and significant even when the functional limitation is included in the model, implying a likely partial mediation of the effect of having an MSK condition.
In Table 6, we explore these results further with the formal mediation analysis. The average indirect or mediation effects are shown to be statistically significant at the 5 percent level for each of the functional limitation questions. Experiencing moderate to severe pain has the largest mediation effect, with the model estimating that pain mediates approximately 58 percent of the direct effect of the MSK condition. Furthermore, the direct effect of the MSK is no longer statistically significant at the 5 percent level in the mediation analysis with pain and the confidence interval on the percent mediated includes 100 percent, implying a full mediation effect. The mobility limitation, upper and lower body limitations also have mediating effect. Indeed, we estimate that 22 percent of the relationship between having an MSK condition and employment is attributable to having a lower body limitation and that 18 percent of the relationship is attributable to having mobility limitations. On the other hand, just 10 percent of the relationship is mediated by upper body limitations. As shown in the informal analysis, the direct effect of MSK condition on employment remains significant in these models despite the addition of the mediating variables.
Mediation Effect
Mediation Effect
Notes: Data from all five rounds of the National Beneficiary Survey. Statistics calculated using medeff command in Stata (Hicks and Tingley, 2011) with respondent weights rescaled to maintain the proportion of respondents in each wave of the survey.
The objective of our analysis was to test the hypothesis as to whether functional limitations mediate the relationship between health conditions and employment. We focused our analysis specifically on SSD beneficiaries with MSK conditions, as these individuals have some of the lowest employment rates among beneficiaries and are thus the focus of much policy attention. Our descriptive analysis has demonstrated that SSD beneficiaries with MSK conditions have low employment rates and are more likely to report physical barriers and less likely to report environmental barriers to work than other beneficiaries. We provide evidence to suggest that the relationship between MSK conditions and employment is mediated by functional limitations. In other words, a significant share of the low employment rates of the MSK population can be attributed to their functional limitations.
In focusing on the role of functional limitations, this research can offer practical insights for vocational rehabilitation practitioners on how best to intervene, both in individual and environmental contexts, by providing appropriate accommodations or other forms of services and supports that can assist beneficiaries in returning to work. The fact that a smaller share of MSK beneficiaries report environmental barriers to work suggests that addressing functional limitations and physical health is likely of first order importance in enabling employment in this population. Vocational rehabilitation services designed to reduce the impact of these limitations may thus be particularly important to improve employment outcomes among MSK beneficiaries. Rehabilitation practitioners may also benefit from gathering additional information on the functional limitations experienced by their clients. This information could be used to design programs and services to better meet the needs of their clients.
Our finding that moderate to severe pain has a fully mediating effect on the impact of the MSK conditions, suggests that this is a natural place to focus attention. VR providers and health providers should prioritize effective pain management strategies for clients who indicate that pain is a problem. While pain can be challenging to measure and manage, recent evidence suggests that some of the most effective strategies likely involve a holistic combination of education with physical, psychological and, in some cases, pharmacological interventions (Foster et al., 2018). Employers can also play a role in mitigating the impact of these functional barriers to work by providing employees flexibility in terms of their work environment, hours, special equipment, and other accommodation when needed.
It is worth noting that information on the functional limitations is already collected for many SSD beneficiaries by the SSA. SSD applicants at the later stages of the disability determination process, must complete a Residual Functional Capacity (RFC) assessment that assesses their functional limitations, such as being able to walk without stopping, carry weights greater than 10 pounds, as well as the ability to get along with coworkers or interact appropriately. The eligibility of approximately 50 percent of all applicant decisions are decided in the last two stages of the determination process where the RFC assessment is considered (Hu et al., 2001, SSA, 2015; Chen and Van der Klaauw, 2008, Wixon & Strand, 2013). The information from the RFC is currently used exclusively for eligibility determination purposes. However, this functional information could also be useful information for vocational rehabilitation providers, and at targeting other return to work interventions more effectively.
Limitations
Our analysis provides evidence of a statistically significant mediation effect of several functional limitations for a representative sample of SSD beneficiaries. However, we present our findings as a descriptive analysis for several reasons. First, functional limitations are not randomly assigned within the population of SSD beneficiaries with MSK conditions and even after controlling for personal characteristics, we cannot account for all of the differences between those with a particular functional limitation and those without. For example, some underlying comorbidities may increase the propensity of experiencing a functional limitation and could affect employment, but not all comorbidities can be captured in the data. Secondly, other factors, such as an individual’s occupation or employment environment prior to disability, are not measured in the NBS. The safety and physicality of the work environment varies between sectors and individuals in some occupations or sectors could be more likely to experience a functional limitation due to the nature of their work (Mäntyniemi et al., 2012). Moreover, some employers are likely to provide more flexibility in work hours and accommodations than others. Third, while we believe that the functional limitations measured here do have an indirect impact on employment, we lack fully comprehensive measures of all potential functional limitations. Other research has shown that psychological health and self-efficacy could have an important impact on employment (Umucu et al., 2016), and these measures are not included in our analysis. Furthermore, the measures we do have are self-reported by surveyed beneficiaries, and may be subject to measurement error.
Finally, we acknowledge that our results may not be generalizable beyond this population of SSD beneficiaries. While this group is of considerable policy importance, they likely do not reflect the entire population of individuals with MSK conditions who may face challenges in working. In particular, SSD beneficiaries have been out of the labor force for a longer period of time and may have experienced some depreciation of their relevant skills (Autor et al., 2015), or may have more significant chronic conditions than the overall population. Future research should use alternative data sources to extend our approach to the overall population of individuals with MSK conditions to explore the potential for intervention at an earlier stage in the development of an individual’s condition.
Conclusion
Prior research on the employment of SSD beneficiaries had yet to analyze the relationship between the functional limitations of beneficiaries and their work-capacity. In this paper, we hypothesized that functional limitations mediate the association between health conditions of beneficiaries and their likelihood of employment. We focused our study on beneficiaries with MSK conditions, as this population has some of the lowest employment rates and has grown as a share of all beneficiaries. We thus proposed that a study of our hypothesis as it relates to those MSK conditions can provide a useful case study for the overall hypothesis.
Our results indicate that functional limitations do mediate the relationship. We find evidence of a significant mediation effect, with our estimates implying that moderate to severe pain mediates approximately 50 percent of the direct effect of an MSK condition on employment; and that lower body, mobility, and upper body limitations mediate 18, 15, and 7 percent of the direct effect of an MSK condition, respectively. Beneficiaries with MSK conditions also report fewer environmental barriers to employment than those without MSK conditions and are significantly more likely to report that their physical condition prevents them from working. These results suggest that addressing functional limitations may be of first order importance in enabling employment for the MSK population.
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Acknowledgments
We would like to acknowledge the support of the Disability Research Consortium Summer Fellowship Program at the Mathematica Center for Studying Disability Policy, and are grateful for helpful comments from Gina Livermore, David Mann, Yonatan Ben-Shalom, David Stapleton, and Jody Schimmel Hyde.