
Abstract
BACKGROUND:
Physical health conditions are pervasive among individuals with serious mental illness (SMI) living in the community. And many individuals with SMI are unemployed despite their desire to work.
OBJECTIVE:
This study explored participants’ perceptions of physical and mental health conditions as barriers to employment and the impact of such conditions on job-searching activities.
METHODS:
The participants (n = 162) reported their mental and physical health status and their employment-related activities and barriers over a 12-month study period. Frequency analysis and Chi-square tests were conducted to examine the relationship between the participants’ perception on physical or mental health conditions as a barrier to employment and their conducted job-related activities.
RESULTS:
More participants reported physical health conditions than mental health conditions as a barrier to job-related activities. Participants’ perception on physical health conditions as a barrier to employment significantly decreased job-related activities, while mental health conditions did not. In addition, more participants reported long-term physical health conditions as a barrier than short-term ones. Participants identified physical problems more frequently than mental health problems for limiting their work or other activities.
CONCLUSIONS:
Integrating care of physical health conditions in mental health services should be considered for improving employment participation and outcomes.
Introduction
The benefits of employment participation among individuals with serious mental illnesses (SMI) are well documented. Employment success is correlated with increases of financial resources, self-esteem, housing stability, quality of life, and decreases in symptom distress, substance abuse, mental health service utilization and crises (Akihito et al., 2015; Bunnings et al., 2015; Burt, 2012; Dunstan et al., 2017; Kukla et al., 2012;). On the other hand, unemployment, especially long-term unemployment, can undermine access to basic needs and health care that directly jeopardize the wellbeing of these individuals. Studies have found those who experienced prolonged unemployment reported increased levels of stress about financial resources, dependence upon public assistance, lack of access to needed health care, poorer physical health, higher occurrence of sleep loss or disturbance, greater risk of cardiovascular diseases, loss of a sense of belonging and positive self-identity, and increased levels of isolation, anxiety and depression (Gonzalez et al., 2018; Hiswals et al., 2017; Julia et al., 2017; Naslund et al., 2017, Romain et al., 2017; Premji, 2017; Sumner & Gallagher, 2017; Zandara et al., 2016).
Over the past three decades, interventions such as the Individual Placement and Support (IPS) model of Supported Employment have improved employment outcomes among many individuals with SMI (Bond et al., 2008; Drake et al., 2016). However, increasing employment participation among individuals with SMI remains challenging. In 2016, results of a national survey estimated 10.4 million adults in the United States were diagnosed with SMI (Ahrnsbrak et al., 2017; SAMHSA, 2017), representing 4.2% of the total adult population. The overall rate of employment participation among this group remains extremely low, between 10% and 20% (Bertram & Howard, 2006; National Alliance on Mental Illness, 2014; Salkever et al., 2007). At least three million working-aged adults with SMI depend on Social Security benefits - 40% of all Social Security Supplemental Security Income (SSI) recipients and 28% of all Social Security Disability Insurance (SSDI) recipients. This disability group has been rapidly growing and is now the largest subgroup of disabled adults (Colpe et al., 2010; Drake et al., 2009; Mojtabai, 2011).
Individuals with SMI face many barriers to employment success, including lack of education and job training, gaps in employment, stigma of mental illness, and lack of support. Milfort et al. (2015) identified three barriers to employment among SSDI recipients with mental disorders and more than half reported poorly controlled mental illness symptoms as the biggest barrier (55%), followed by nonengagement in supported employment (44%) and poorly controlled general health issues (33%). One barrier to employment participation among this population that has not been well reported and studied is poor physical health, despite the increasing evidence that individuals with SMI are also more likely to experience physical health related diseases when compared to the general population (Brunero & Lamont, 2010; Shuel et al., 2010). Several studies have indicated an association between SMI and several adverse health outcomes, such as type 2 diabetes, metabolic syndrome, cancer, dementia, anxiety, and premature mortality (Romain et al., 2017). Taking into consideration only obesity, for example, individuals with SMI have a prevalence nearly double that of the general population (Naslund et al., 2017, Nishi et al., 2017). The high risk of poor physical health among individuals with SMI is clear and dire, particularly when taking into account that the life expectancy of individuals with SMI may be reduced by up to 25 years (Parks et al., 2006; Shuel et.al, 2010). Some studies have suggested that employment may be a key component of improving and maintaining mental health and physical health (Bunnings et al., 2017; Schmitz, 2011). However, limited data of poor physical health as a barrier to employment engagement are available. This paper provides some detailed information for drawing attention to the issue.
Method
Participants and procedures
This study is part of a three-year study that examines the impact on employment outcomes for individuals with SMI in Supportive Housing (SH) programs. The institutional review board (IRB) at the institution of the authors approved the study procedure. The main purpose of the study was to test employment outcome differences between two staff training models. However, no significant differences were found between the two models, and both models yielded low employment rates. Consequently, barriers to obtaining employment among the participants were explored. Participants reported a variety of barriers including lack of education, employment history, and transportation, as well as physical and mental health concerns. Among them, physical health conditions were by far the most consistently reported barrier. In this paper, we focus on the exploratory findings about physical health conditions as a barrier to employment related activities and role limitations that study participants reported over a 12-month period. The study protocol was approved by the University Institutional Review Board.
There were a total of 162 study participants recruited from 11 Supported Housing (SH) Programs serving individuals with SMI in two states of the northeast region. The SH programs varied in size, ranging from serving under 100 to about 300 individuals. The programs also varied in settings including urban, suburban and rural areas.
Over a 12-month study period, a participant met with a member of the research team three times in person. These were at intake, 6-months, and 12-months. During the three interviews, information about participant’s physical health was obtained each time. A monthly telephone follow-up survey took place in between the three in-person meetings. During the monthly telephone follow-up survey, a research team member collected the participant’s employment related activities during the month, such as the number of job applications submitted, number of job interviews completed, and whether obtained a job or not during the month. Additionally, the participant was asked to identify the barrier(s) to pursuing employment activities.
Table 1 describes the demographics of the participants. The average age of the sample was 50.72 (SD = 9.52). Close to half of the participants were in their fifties (n = 74, 45.68%). There were similar numbers of men and women in the study, and five participants (3.09%) identified themselves as either intersex or transgender. Many participants identified as Black/African American (n = 90, 55.56%) or as White (n = 57, 35.19%). Almost half of the participants have a high school diploma (n = 74, 45.68%), and 44 (27.16%) either had some college education or graduated from college. Roughly 60% (n = 96, 59.26%) of participants were not employed during the last five years. Regarding reported primary psychiatric diagnosis, 38% self-reported having Schizophrenia or Schizoaffective disorder, 29% had Bipolar Disorder, and 25% had Major Depressive Disorder. Additionally, 61 participants reported more than one psychiatric diagnosis. The Brief Psychiatric Rating Scale (BPRS) was used to measure the severity of psychiatric symptoms, with a Likert scale, from 1 (Not present) to 7 (Extremely severe). The average score of the BPRS at intake was 1.43 (SD = 0.36), 1.41 (SD = 0.32) at 6-months, and 1.42 (SD = 0.40) at 12-months. The symptom level of 6-months and 12-months was not statistically different from that of intake (t (121) = 0.79, p = 0.45, t (123) = 0.14, p = 0.89). Thus, it appeared that the participants experienced very mild psychiatric symptoms over the 12-month study period.
Demographics of the participants
Demographics of the participants
Self-perceived role limitation due to physical health and emotional health
Information of perceived health was collected using several items of the Short Form (SF-36) Health Survey during the intake, 6-month and 12-month interviews. SF-36 is a widely used self-report survey instrument for health-related quality of life. It assesses subjective health, which are conceptually subsumed in the areas of “physical” and “emotional” health. In its context, the term “emotional health” is exchangeable for mental health. For this study, we surveyed four items of the Role Limitation due to Physical Health and three items of the Role Limitation due to Emotional Problems subscales. An example of the physical health items is “As a result of your physical health, have you cut down the amount of time you spent on work or other activities during the past 4 weeks?”, and one example of the emotional health items is “As a result of emotional problems, I did not do work or other activities as carefully as usual.” The answer keys are “yes” or “no.”
Job-related activities and barriers
Participants were asked the questions regarding job-related activities and barriers for job-related activities during phone interviews every month except for the 6th and 12th months when there was a comprehensive in-person interview with a different set of questions. During the monthly phone follow up, participants were asked to report employment status and job-related activities. Questions included how many job applications were submitted, how many interviews were completed, and how many job offers were received during the last month. A new dichotomous variable “job related activity” was created. It would be coded “yes” if a participant answered “one or more” to any one of above three questions of job application, interview and job offers. Additionally, participants were asked the following question to identify any barrier experienced to pursuing job-related activities: “What barriers, if any, did you experience during the past month that got in the way of looking for, applying for, interviewing, or beginning a job?” Their answers were then coded into 49 categories such as transportation problem, lack of childcare, physical health problem, and mental health problem. Physical or mental health barriers were then coded either as short-term or long-term problem. Examples of short-term health problem were having a bad cold last month, or shoulder and back injuries from a car accident. Examples of long-term health problem were experiencing lot of pain in knee and leg, or having diabetes. Examples of long-term mental health problem were being depression for years and having no energy to look for a job, or too anxious when thinking about looking for a job. Examples of short-term mental health problem were new medication making me too sleepy to function, or feeling sad over my aunt’s passing.
Data analysis
Frequency analysis was conducted for the perceived role limitations due to physical and mental health issues that were asked at intake, 6-month, and 12-month interviews. Chi-square tests were conducted for monthly responses to examine the association between identified physical or mental health issues as a barrier to job-related activities and job-related activities during that month.
Results
Physical and mental health issues as a barrier to job-related activities
In each of the 10 monthly follow-ups, 10.7% to 26.1% of the participants reported their long-term physical health problems as a barrier to job-related activities, and 2.1% to 9.3% reported a short-term physical health issue as a barrier. Regarding mental health issues, 0% to 1.5% reported long-term illness as a barrier, and 3.5% to 11.6% reported a short-term illness as a barrier. Figure 1 provides detailed information.
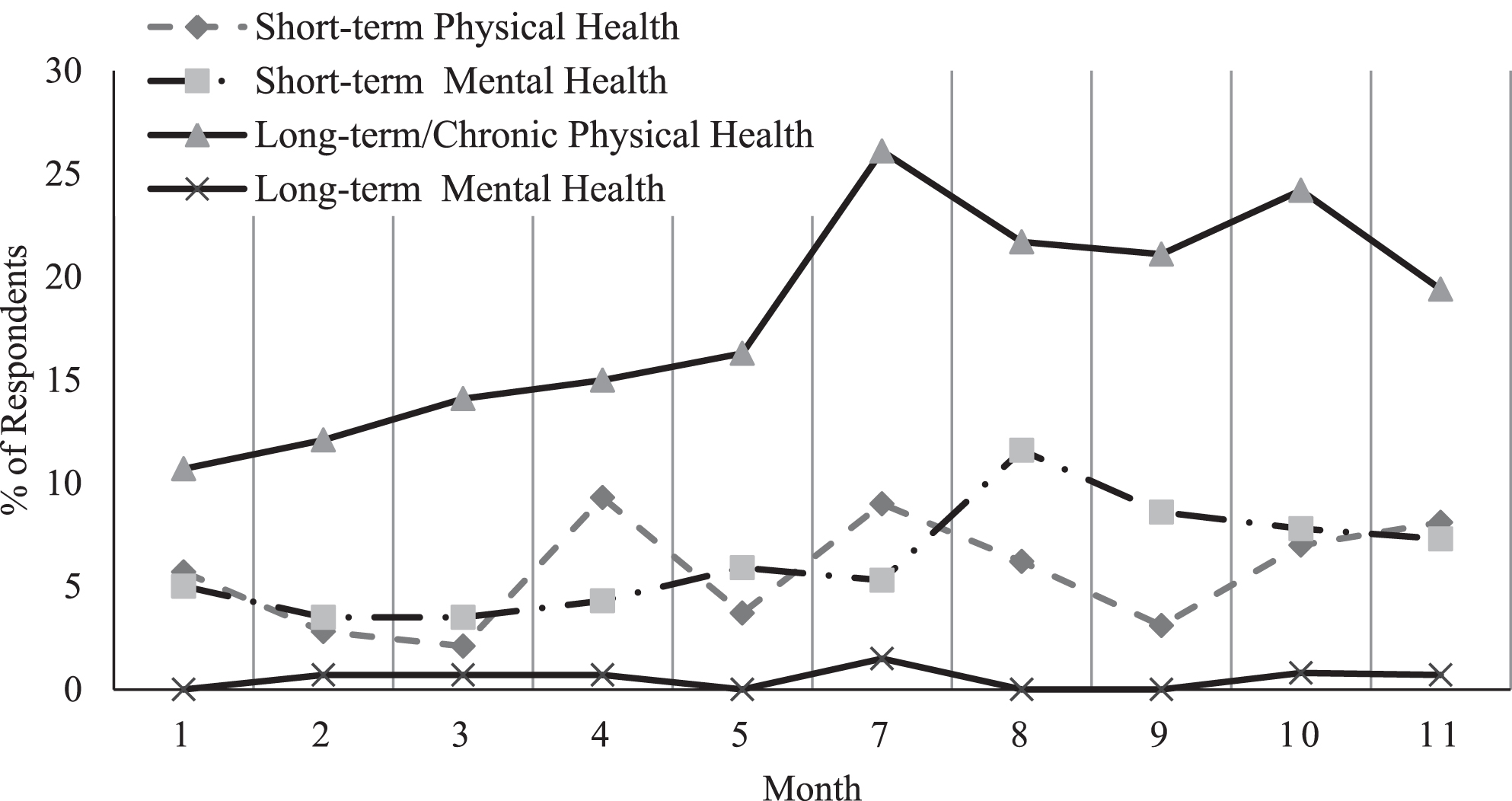
Physical Health Condition as a Barrier to Job-related Activities.
Chi-square tests were performed, 10 for long-term physical health conditions and 10 for short-term physical health conditions. Before performing chi-square tests, tables were examined to determine whether any expected value in each cell was less than five. For the tests with expected cells less than five, Fisher’s Exact test was performed instead. The chi-square test results of 4th, 8th, 10th, and 11th month rejected the independence model between the two dichotomous variables, indicating that participants who identified long-term physical health conditions as a barrier were significantly less likely to have done job-related activities in these four months. Meanwhile, the participants who identified short-term physical health issues as a barrier were significantly less likely to have done job-related activities in the 4th month only. These results are presented in Table 2. Continuity was corrected with Yates’s correction, to reduce an error in approximation of Pearson’s chi-square statics to the continuous chi-square distribution when the table indicates discrete probability of binomial frequencies. The p-value of the 10th month result of long-term physical health condition was slightly over 0.05 when using Yates’s correction Participants’ perceptions of whether their mental health conditions was a barrier to employment were all independent of their job-related activities, suggesting no relationship between the perception of mental health conditions as a barrier and the extent of job-related activities.
Relationship of physical health conditions as a barrier and job-related activities
Note.+p < 0.10, *p < 0.05, **p < 0.001. Long-terma indicates chi-square test results between job-related activities and long-term/chronic physical health conditions as a barrier. Short-termb indicates Fisher’s Exact test result of short-term physical health conditions.
Table 3 demonstrates the frequency of role limitations due to physical and emotional/ mental health conditions at intake, 6-months, and 12-months of the study. The main finding is that reported role limitations due to physical health did not decrease over a 12-month period, while limitations due to mental health decreased over time. Thus, it suggests physical health problems had longer duration and lasting limitations on work and other activities among the participants.
Participants’ self-perceived role limitations due to physical and emotional/mental
health
Participants’ self-perceived role limitations due to physical and emotional/mental health
The study participants consistently reported greater role limitations due to their physical health problems than mental health issues over the 12-month study period despite after employment intervention was integrated into the Supported Housing program. Of physical health problems, long-term conditions including diabetes, chronic pain, and obesity were reported more frequently than short-term physical health problems such as having a cold, or injures from accidents. Furthermore, participants perceived that physical health conditions negatively affected their job-related activities such as job searching, submitting applications, and interviewing. More seriously, their perceptions of long-term physical health conditions as barriers were actually significantly associated with fewer job-related activities.
Unaddressed long-term physical health problems among people with SMI unquestionably contribute to the overall higher rate of physical health related diseases and premature mortality as compared to the general population (Brunero & Lamont, 2009; Romain et al., 2017; Shuel et al., 2010). Furthermore, physical health problems severely diminish their opportunities for engaging in employment activities in which they have the potential of gaining resources for and access to quality health care. The lack of employment participation also deprives these individuals of the benefits from being employed including increased financial resources, self-worth, community integration, and quality of life.
The study findings also provide more evidences for the urgent needs for integrated mental health and physical health care for the population with SMI, especially for long-term, chronic conditions. There have been some studies in recent years showed promising outcomes when integrated care was provided (Mangurian et al., 2017; Mcginty et al., 2018). On the other hand, there is still serious disparity in healthcare provision between those with SMI and the general population. Studies found unequal quality of healthcare provision contributed to excess mortality. People with SMI are less likely to receive cancer screening during routine medical checkups (Carney & Jones, 2006; Lawrence & Kisely, 2010; Xiong et al., 2008). Individuals with schizophrenia have lower rates of surgical interventions such as stenting and bypass grafting for cardiovascular diseases (Druss et al., 2001; Laursen et al., 2008). Other studies found long-term health problems are very common in people with SMI, but are usually under-recognized and under-treated (Dixon et al., 1999; McIntyre et al., 2007). Considering that when physical health problems are unaddressed, other services including employment programs might not be effective, the need for integrated care exists for people with SMI for their successful recovery and rehabilitation.
There are a few limitations of the findings. Role limitations and physical and mental health data were self-reported without corroboration from health care records or providers. The study was conducted at 11 different sites where inconsistencies of program structures and elements might have influenced the study findings. The study also includes many older participants who might have lower motivation for employment participation and usually have more physical health problems. Two different staff training models of employment services at these study sites might have affected the association between limitations due to health conditions and job-related activities. Also, alcohol or drug use can affect their physical health or job-related activities, but the data were not collected by big enough sample that catches substance use to the meaningful analysis results. Bigger sample is recommended in the future studies. Side effect of psychiatric medication also shows as physical health concerns such as weight gain (Correll et al., 2015) and they can be explored as a barrier for employment in future studies.
In sum, poor physical health among individuals with SMI is a serious, persistent, and pervasive barrier to employment participation in this population. For optimum improvement, this must be addressed with the integration of care of mental health, vocational and medical services. Without addressing physical health problems, individuals with SMI will not only continue experiencing more health problems and diseases, but fewer opportunities of employment participation to improve their quality of life.
Conflict of interest
None to report.
Footnotes
Acknowledgments
This article reports partial findings of the study “Evaluating the Impact of Employment Services in Supportive Housing”, supported by National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR Grant# 90IF0088). The findings and interpretation of the data expressed in the article do not necessary represent the views of NIDILRR, but are the sole responsibility of the authors. The authors declare that they have no conflict of interest.
The authors would like to thank many of our Department colleagues who made various contributions to the study, including Ann Murphy, Joni Dolce, George Brice, Francine Bates, Brittany Stone, Bill Waynor, and two research assistants, John Beninato and Silvia Baker.