
Abstract
BACKGROUND:
Transition from adolescence to young adulthood (ages 18– 35 years) can be particularly difficult for people with epilepsy as they have to cope with stressors and challenges associated with independent living, postsecondary education, healthcare, social relationships, and employment.
OBJECTIVES:
To evaluate constructs based on Kumpfer’s resilience framework model as predictors of life satisfaction in young adults with epilepsy.
METHOD:
194 young adults with epilepsy participated in the present study. A hierarchical regression analysis (HRA) was conducted to answer the research questions.
RESULTS:
HRA results indicated that variables in Kumpfer’s resilience framework model significantly predicted life satisfaction of young adults with epilepsy, R2 = 0.71, f2 = 2.45, which is a very large effect size. Family support, friends support, secure attachment, core self-evaluations, and trait resilience were found to contribute significantly to the variation in life satisfaction scores after controlling for the effect of other variables in the HRA model.
CONCLUSION:
Findings of the present study strongly support the validity of Kumpfer’s (1999) resilience framework model, particularly the important roles of person-environment factors in predicting life satisfaction of young adults with epilepsy. This model approach to defining resilience can be used by rehabilitation counselors in case conceptualization, assessment, planning, and counseling.
Introduction
Transition from adolescence to young adulthood (ages 18– 35 years) is a significant milestone for individuals with or without disabilities (Arnett, 2000). In particular, the period of emerging adulthood (ages 18– 25 years) represents the years of profound change and importance— a critical time during which young people explore relationships, education, and employment opportunities that will pave the way for meaningful careers, allowing them to support themselves and to form their own families (Arnett, 2000). This transition process is particularly challenging and stressful for young adults with disabilities because the competencies required for adult life are different from the life of a teenager. Transition challenges facing emerging adults with disabilities include moving from home to independent living, school to work, and pediatric to adult health care. These challenges become more difficult to overcome if the person is not well prepared for the move from the security and protection of living at home to increased independence (Dutta et al., 2019; Wehman et al., 2014).
Epilepsy is a central nervous system (CNS) disorder in which brain activity becomes compromised, causing seizures or periods of unusual behavior, sensations, and sometimes loss of awareness (Falvo & Holland, 2018; Mayo Clinic, 2019). In 2015, 1.2% (3.4 million) of the United States population had active epilepsy (Centers for Disease Control and Prevention [CDC], 2015). In addition, epilepsy is a frequently misunderstood and highly stigmatized disorder (Herrmann et al., 2016). The impact of epilepsy stigma and discrimination on the individual can be extensive, with psychosocial and physical consequences (Wilde & Haslam, 1996). For example, the prevalence of depression and anxiety and the unemployment rate are significantly higher for people with epilepsy compared to people without epilepsy (Feist et al., 2013; Herrmann et al., 2016; Holland et al., 2013; Kwon & Park, 2014). The transition-related challenges faced by young people with epilepsy are amplified by this stigma and additional negative factors. Helping young adults with epilepsy develop character strengths, hope, optimism, self-efficacy, and coping resources will help equip them to manage the psychological, social, and cultural demands of adult life.
Recently, positive psychology has received considerable attention in professional psychology and counseling. This is because the focus of counselors and psychologists on psychopathology traditionally is to help clients improve their mental health conditions (Seligman & Csikszentmihalyi, 2000). This “fix-what’s-wrong” approach underestimates the human potential and people’s innate psychological needs and motivation to live their lives with dignity, to improve themselves, to be happy and healthy, and to thrive (Chou et al., 2013; Seligman, 1998). Conversely, positive psychologists seek to understand the positive aspects of human nature and the extent to which these positive human traits can buffer against life challenges and mental health issues (Seligman & Csikszentmihalyi, 2000). Instead of concentrating on maladaptive behaviors, the goals of positive psychology are to identify and enhance character strengths (e.g., hope, resilience, optimism, self-efficacy, and flexible coping) that make life worth living and allow individuals and communities to flourish and thrive (Chou et al., 2013; Froh, 2004; Seligman & Csikszentmihalyi, 2000; Umucu et al., 2018). The rehabilitation counseling philosophy shares this emphasis on personal assets and strengths, which provides a solid foundation for integrating positive psychology into the professional practice of rehabilitation counseling (Chou et al., 2013).
Resilience is one of the most extensively investigated constructs in positive psychology (Joyce et al., 2018). In its simplest terms, resilience is defined as a person’s ability to “bounce back” quickly from adversity (Dyer & McGuinness, 1996). Luthar, Cicchetti, and Becker (2000) defined resilience as the maintenance of positive adaptation by individuals despite experiences of significant adversity. However, many related person-environment contextual factors also contribute to resilience, including individual characteristics, support from family and friends, and the availability of additional resources and opportunities (Catalano et al., 2011; Tansey et al., 2017). In general, research has demonstrated resilience as a protective factor against depression and a facilitator for life satisfaction (Ring et al., 2016). A systematic review and meta-analysis conducted by Joyce and colleagues (2018) indicated that resilience interventions based on a combination of cognitive-behavioral therapy and mindfulness techniques have a positive impact on individual resilience. As a result, resilience has begun to receive attention in rehabilitation counseling research. There is emerging evidence to support the relationship between resilience and psychosocial adjustment and quality of life, especially in individuals with traumatic disabilities and CNS disorders including epilepsy (Catalano et al. 2011; Fujikawa et al., 2013; McAllister et al., 2015; Ring et al., 2016; Tansey et al, 2017; Tansey et al., 2016). Conversely, negative life experiences such as disability-related symptoms, functional limitations, perceived social stigma, and lack of support or resources can raise the burden and stress of living with a disability, thus adversely affecting people’s health and well-being and their ability to bounce back from adversity. Stigma related to a disability such as epilepsy can often cause as much if not more suffering than physical manifestations of the disorder, affecting how individuals respond to their chronic health conditions and disabilities (Amoroso et al., 2006). Identifying positive human traits such as resilience and positive environmental contextual factors such as social support, particularly in young adults with epilepsy, can increase generalized self-efficacy, self-esteem, locus of control, and positive affect, leading to a better quality of life.
Specifically, resilience has been investigated in rehabilitation counseling and psychology research among individuals with spinal cord injuries, where resilience has been found to be a protective factor against depression (Catalano et al., 2011; Tansey et al., 2016; Tansey et al., 2017) and positively associated with spirituality and satisfaction with life (Quale & Schanke, 2010; White et al., 2010). Research related to fibromyalgia also demonstrated that resilient persons with fibromyalgia have higher positive affect and lower fibromyalgia symptom burden, leading to better quality of life (McAllister et al., 2015). Research findings also indicate that resilience is not merely a personality trait (Catalano et al., 2011; Kumpfer, 1999) but a complex concept that includes positive person and environment contextual factors, and these factors interact to help individuals bounce back quickly from adversity. Kumpfer’s (1999) seminal work on the resilience framework model and resilience-related protective factors has created a paradigm shift through which we conceptualize resilience. This paradigm shift to focus on positive person-environment factors has contributed to the increased awareness of the effect of resilience on psychosocial adjustment of people with chronic health conditions and disabilities in the rehabilitation counseling literature (e.g., Catalano et al., 2011; Chou et al., 2009; Fujikawa et al., 2013). Helping young adults with epilepsy develop resilience based on Kumpfer’s resilience framework model could help them develop other character strengths and coping resources.
Kumpfer’s resilience framework model
Kumpfer (1999) postulated that there are six major predictors of resilience comprising four domains of influence and two transactional time points (i.e., the convergence between the environment and the individual, as well as the individual and the outcome choice). These predictors of resilience are stressors or challenges (e.g., the daily stressors of living with epilepsy), the external environmental context, internal self-characteristics, person-environment interactional processes, resilience processes, and positive outcomes (Kumpfer, 1999). For example, dealing with the challenges and demands associated with transition from adolescence to adulthood can be extremely stressful for young adults with epilepsy. Stress can cause instability in the person (e.g., anxiety and depression) and the environment (e.g., social isolation). However, people react differently to stressful situations, depending on their interpretation of the circumstances as threatening or aversive. For people who are resilient, confronting challenges in everyday life helps them develop hope, meaning of life, generalized self-efficacy, psychosocial resources, and the ability to cope with new stressors. It also helps them to enjoy personal growth from the experience. Contextual factors in the environment (e.g., family, community, culture, school, and peer group) can be both risk and protective factors. For example, social support from friends is a protective factor and social isolation is a risk factor. A supportive environment serves as a buffer from the daily hassles and demands of living with epilepsy. The positive person factors include spiritual, cognitive, social-behavioral, physical, and emotional self-efficacy that enables people to function successfully in everyday life (Kumpfer, 1999). These positive person-environment factors interact to protect the individual from damaging effects of stress and to overcome adversity and challenges in life with an intended outcome of increased life satisfaction. Figure 1 provides a graphical depiction of Kumpfer’s resilience framework model.
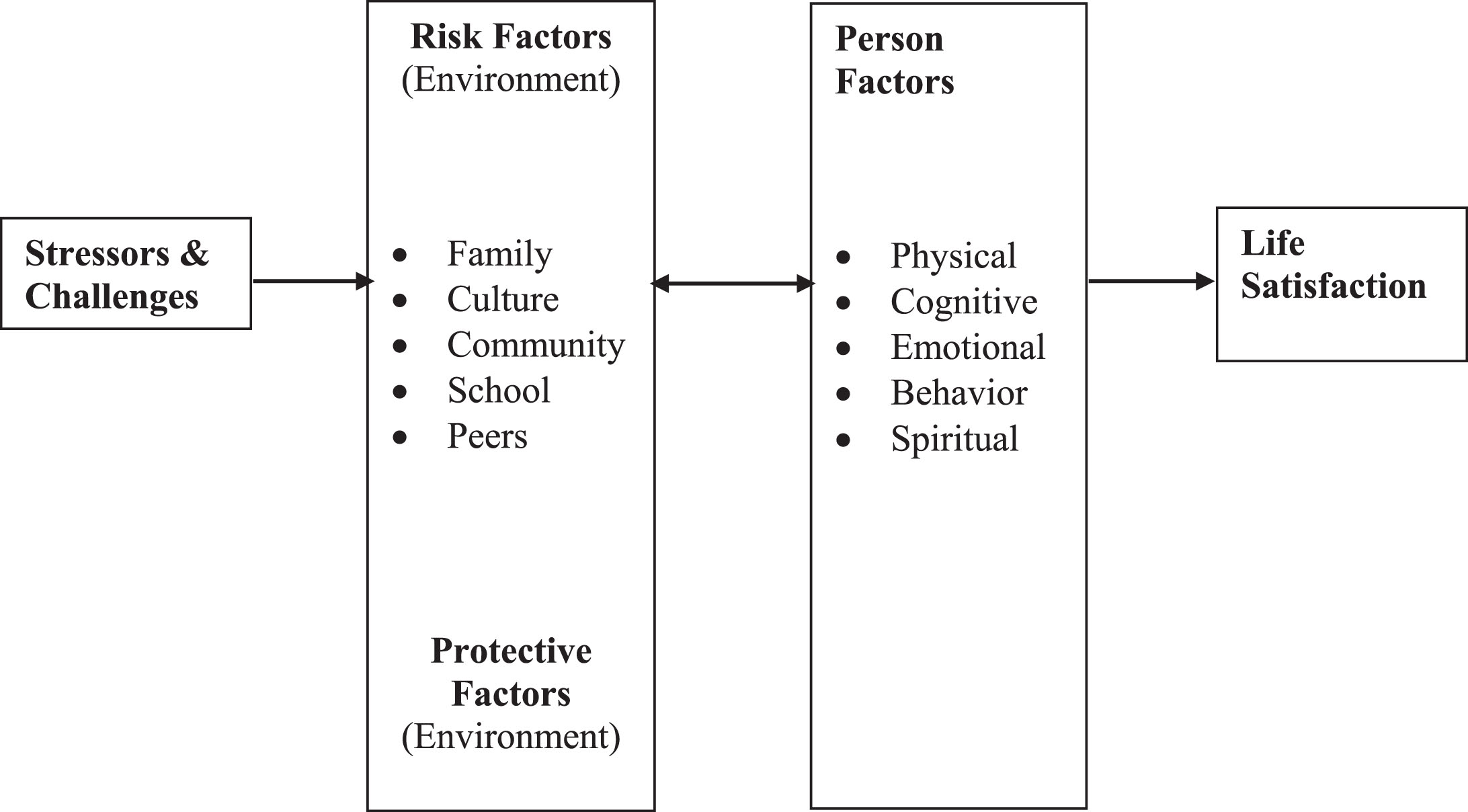
A graphical depiction of Kumfer’s Resilience Framework Model.
Kumpfer’s resilience framework model identifies significant internal and external factors that contribute to the development of resilience and the ability to cope with adverse life events. The combination of the individual, environmental, and situational factors influences the ways in which an individual will perceive, interpret, and respond to adverse events. Presumably, people who are more resilient will be able to cope well and achieve better life outcomes (Catalano et al., 2011). The purpose of the present study was to evaluate constructs based on Kumpfer’s resilience framework model as predictors of life satisfaction for young adults with epilepsy (see Fig. 2).
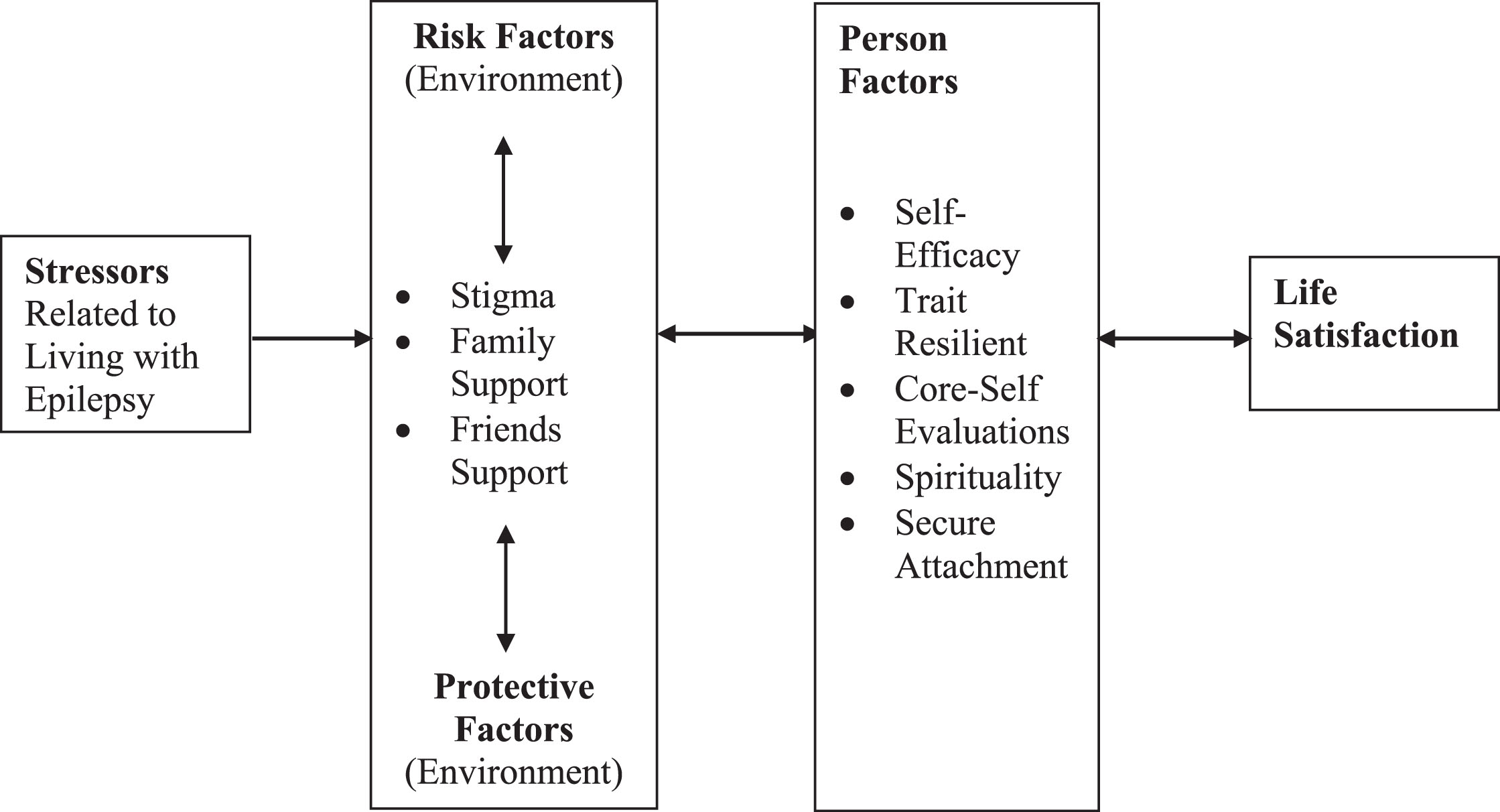
A graphical depiction of the Modified Kumfer’s Resilience Framework Model for emerging adults with epilepsy.
Specifically, the current study included seizure severity for the “stressors and challenges” construct. Living with epilepsy and its related symptoms are the sources of daily hassles and stressors. Rehabilitation counseling researchers have also long recognized the need to consider person-environment contextual factors in the development of effective rehabilitation counseling interventions (Chan et al., 2009, 2019; Wright, 1983). As a result, social stigma and family and friend support, which are risk/protective factors commonly used to predict community participation and life satisfaction of people with chronic health conditions and disabilities, serve as the environmental constructs in this study. A high level of social support is a protective factor and social isolation is a risk factor. Similarly, a high level of perceived epilepsy stigma is a risk factor and a low level of perceived stigma is a protective factor. The person constructs included epilepsy self-efficacy, core self-evaluations, resilient personality, attachment, and spirituality. The resilience outcome was defined by life satisfaction. The following research questions were addressed in the current study:
Participants
One hundred ninety-four (194) persons with epilepsy between the ages of 18 and 35 from several chapters of the Epilepsy Foundation of America participated in the present study. The inclusion criteria were: (a) a diagnosis of epilepsy; (b) age between 18 and 35 years; (c) not living in a residential facility, such as a nursing home; (d) having had a diagnosis of epilepsy for at least six months; and (e) no diagnosis of co-existing intellectual disability. The age of the participants ranged from 18 to 35 years (M = 27.0, SD = 4.4). The majority of the participants were male (59.3%), Caucasian (74.5%), and single (56.7%). Regarding employment status, 35.2% of the participants were employed full-time, 33.7% were employed part-time, 20.7% worked as volunteers, 5.7% were unemployed but actively looking for employment, and 3.6% were students. Reports indicated that 34.5% of participants completed high school, 25.8% participated in post-secondary education (no degree), 14.9% completed an associate’s degree or vocational school, and 22.2% completed college. Approximately 35% of the participants received cash benefits from the Social Security Administration, either supplemental Security Income (SSI, 21.1%) or Social Security Disability Insurance (SSDI, 13.9%). Detailed information for the demographic variables is presented in Table 1.
Demographic characteristics of participants in this study (N = 194)
Demographic characteristics of participants in this study (N = 194)
Stressors and challenges
In the present study, the “stressors/challenges” construct was assessed using the Liverpool Seizure Severity Scale (LSSS; Baker et al., 1998). The LSSS is composed of 20 items and nine clinical features or symptoms of seizures reported over the previous four-week period. Each item is rated on a 4-point Likert scale (0 = Never; 1 = Sometimes; 2 = Usually; 3 = Always). Seizure length is rated from 0 = <1 minute to 3 = > 5 minutes and recovery time is rated from 0 = <1 minute to 5 = > 1 hour; total scores range from 0 to 27, with higher scores indicating greater severity of seizures (Baker et al., 1998). Baker and colleagues (1998) reported an internal consistency reliability coefficient (Cronbach’s alpha) of 0.79 in a sample of patients with epilepsy. In the present study, the Cronbach’s alpha was also computed to be 0.79.
Environmental factors
Two environmental factors, perceived social support and perceived social stigma, were assessed in the current study. These two factors were measured by the Multidimensional Scale of Perceived Social Support (Zimet et al., 1988), and the Epilepsy Stigma Scale (DiIorio et al., 2004).
Perceived social support
The 12-item Multidimensional Scale of Perceived Social Support (MSPSS) was used to measure three sources of support: family, friend, and significant other (Zimet et al., 1988). Each item is rated on a 7 point Likert scale (1 = Very strongly disagree; 2 = Disagree; 3 = Disagree somewhat; 4 = Neither agree nor disagree; 5 = Agree somewhat; 6 = Agree; 7 = Very strongly agree). Total and subscale scores range from 1 to 7 with a higher score indicating greater perceived social support. Kazarian and McCabe (1991) reported a Cronbach’s alpha coefficient of 0.88 for the total scale and 0.87, 0.85, and 0.91 for the family, friend, and significant other subscales, respectively. In the present study, to reduce the length of the survey, only family and friend support were included in the regression model. Cronbach’s alpha coefficients in the present study were 0.92 for family support and 0.83 for friend support.
Perceived stigma
The 5-item Epilepsy Stigma Scale (ESS) was used to measure perceived epilepsy stigma (DiIorio et al., 2004). Each item is rated on a 7-point Likert scale (1 = Strongly disagree; 2 = Disagree; 3 = Disagree somewhat; 4 = Neither agree nor disagree; 5 = Agree somewhat; 6 = Agree; 7 = Strongly agree), with item responses summed to yield a total score, and higher scores indicate greater perceptions of stigma toward a person with a seizure condition (Reisinger & DiIorio, 2009). The ESS has been found to have Cronbach’s alpha internal consistency reliability estimates between 0.89 and 0.91 in various studies of adults with epilepsy (e.g., DiIorio et al., 2004; Reisinger & DiIorio, 2009; Whatley et al., 2010). The Cronbach’s alpha coefficient in the present study was computed to be 0.90.
Person factors
In the present study, six person factors including self-efficacy, secure attachment, spirituality, core self-evaluations, and trait resilience were assessed. These factors were measured by the Epilepsy Self-Efficacy Scale (DiIorio & Yeager, 2003), the Adult Attachment Scale-Revised (Collins, 1996), the World Health Organization (WHO) Spirituality, Religion, and Personal Beliefs Scale (WHO, 1996), the Core Self-Evaluations Scale (Judge et al., 2003), and the 10-item Connor-Davidson Resilience Scale (Campbell-Sills & Stein, 2007).
Self-efficacy
The 18-item version of the Epilepsy Self-Efficacy Scale (ESES-2000) was used to assess self-efficacy of the daily management of epilepsy (DeIorio & Yeager, 2003). Each item is rated on an 11-point Likert scale (0 = I cannot do it all; 5 = Moderately sure I can do; 10 = I am sure I can do it; Sung, 2012). Total scores range from 0 to 180 with higher scores corresponding to higher levels of confidence in one’s ability to manage epilepsy. The Cronbach’s alpha estimates have been reported to range from 0.89 to 0.94 (DiIorio et al., 2003, 2004; DiIorio & Yeager, 2003), and the Cronbach’s alpha coefficient for the present sample was 0.90.
Attachment scale
The 18-item version of the Adult Attachment Scale (AAS) was used to assess the extent to which people are comfortable with closeness and intimacy (close), depend on others when needed (depend), and anxiety about being rejected (Collins, 1996; Collins & Read, 1990). Each item is rated on a 5-point Likert scale (1 = Not at all characteristic of me and 5 = Very characteristic of me). Collins (1996) reported Cronbach’s alpha coefficients for the three subscales to be 0.77 (close), 0.78 (depend), and 0.85 (anxiety). In the present study, the focus was on secure attachment, so only the Depend subscale was included as a predictor in the regression model. The Cronbach’s alpha coefficient for the Depend scale within the present sample was 0.54.
Spirituality
The 32-item World Health Organization Quality of Life Spirituality, Religion, and Personal Beliefs Scale (WHOQOL-SRPB) was used to assess spirituality (The WHOQOL Group, 2002). It is composed of eight factors: (a) spiritual connection; (b) meaning of life; (c) awe, wholeness/integration; (d) spiritual strength; (e) inner peace; (f) hope; and (g) faith (Boero et al., 2005). Each item is rated on a 5-point Likert scale (1 = Not at all; 2 = A little; 3 = A moderate amount; 4 = Very much; 5 = An extreme amount), with higher scores indicating higher spirituality. A Cronbach’s alpha coefficient greater than 0.70 was reported in previous research (Giovagnoli et al., 2006), the Cronbach’s alpha coefficient found for the sample in the present study was 0.91.
Core self-evaluations
The 12-item Core Self-Evaluations Scale (CSES) was used to assess core self-evaluations, a higher order personality trait consisting of self-esteem, generalized self-efficacy, emotional stability, and internal locus of control (Judge et al., 2003). Each item is rated on a 5-point Likert scale (1 = Strongly disagree; 2 = Disagree; 3 = Neutral; 4 = Agree; 5 = Strongly agree). Previous research indicates strong internal consistency estimates greater than 0.80, along with test-retest reliability of 0.81 (Judge et al., 2003). The Cronbach’s alpha coefficient for the present study was estimated to be 0.84.
Trait resilience
The 10-item version of the Connor-Davidson Resilience Scale (CD-RISC-10) was used to assess resilience and the personal qualities that enable individuals to thrive when faced with adversity, with higher scores indicating higher resilience capacity. Each item is rated on a 5-point Likert scale (0 = Not true at all; 1 = Rarely true; 2 = Sometimes true; 3 = Often true; 4 = True nearly all of the time). Previous research reports a strong internal consistency estimate of 0.95 for the CD-RISC-10 (Campbell-Sills & Stein, 2007), and the current study computed the Cronbach’s alpha coefficient at 0.82.
Life Satisfaction
In the current study, life satisfaction served as the outcome variable, which was measured using the Satisfaction with Life Scale (SWLS; Diener et al., 1985). The SWLS is a 5-item scale designed to measure global cognitive judgments of one’s life satisfaction. Each item is rated on a 7-point Likert scale (1 = Strongly disagree to 7 = Strongly agree) with a total score ranging from 5 to 35. Higher scores indicate higher levels of life satisfaction (Corrigan et al., 1998; Pavot & Diener, 1993). A Cronbach’s alpha of 0.87 and a test-retest reliability of 0.82 were reported by Diener and colleagues (1985). In the present study, a Cronbach’s alpha of 0.95 was estimated.
Data analysis
A hierarchical regression analysis (HRA) was used to measure the incremental variance accounted for by each predictor set in the resilience framework model. HRA is a flexible strategy for matching analysis to theory (Hoyt et al., 2008). It is appropriate for hypothesis testing when hypotheses can be formulated in terms of added or incremental Y (outcome variable) variance accounted for by one set of predictors over and above what was explained by predictors entered at earlier steps in the model. In the current study, the order of entry of sets of predictors into the regression model was determined by Kumpfer’s resilience model in order to address the research questions. An a priori power analysis was conducted for the total R2 value (H0: R2 = 0) for the HRA with nine predictor variables, power equal to 0.80, and an alpha level of 0.05. Results from this analysis using G*Power (Faul et al., 2007), a software tool for a general power analysis, indicated that a sample size of 176 would be needed to detect a medium effect size (f2 = 0.15), alpha = 0.01, power = 0.80, and 13 predictors (Cohen, 1988).
Results
Hierarchical regression analysis
A hierarchical regression analysis (HRA) was conducted with life satisfaction as the dependent variable and four sets of resilience framework model predictors entered in sequential steps. Step 1 included demographic covariates (gender, race, marital status, and educational attainment). Step 2 included stressors and challenges (seizure severity). Step 3 included environment factors affecting resilience (social stigma, and social support from family, friends, and significant others), and step 4 included person factors affecting resilience (core self-evaluations, resilient personality, spirituality, and attachment). The correlations between the life satisfaction and the resilience framework model predictors ranged from medium to large, and the correlation matrix for all variables is presented in Table 2. Results of the HRA, including values of change in R2 (ΔR2), along with unstandardized regression coefficients (B), standard errors (SE B), and standardized coefficients (β), for the predictor variables at each step and in the final model are presented in Table 3.
Correlations, means, and standard deviations for the predictor and outcome variables
Correlations, means, and standard deviations for the predictor and outcome variables
*p < 0.05; **p < 0.01.
Hierarchical regression analysis for prediction of life satisfaction (N = 194)
Note: F(13, 180) = 34.29, p < 0.001 for the full model; ΔF(4, 189) = 20.84, p < 0.001 for Step 1; ΔF(1, 188) = 27.64, p < 0.001 for Step 2; ΔF(3, 185) = 23.52, p < 0.001 for Step 3.
Demographic covariates were entered in the first step of the regression analysis. This set of variables accounted for a significant amount of variation in life satisfaction scores (R = 0.55, R2 = 0.31, F(4, 189) = 20.84, p < 0.001). Upon examining the standardized partial regression coefficients, being married, β= 0.27, t(193) = 3.49, p < 0.01; and educational attainment, β= 0.36, t(193) = 4.67, p < 0.001 were found to significantly contribute to the variation in life satisfaction scores after controlling for the effect of other demographic variables in the model. The results indicated that being married and higher levels of educational attainment were associated with higher levels of life satisfaction.
The challenges/stressors variable (epilepsy severity) was entered in the second step of the regression analysis. Epilepsy severity accounted for a significant increase in the variation in life satisfaction scores beyond that explained by the demographic variables: R = 0.63, R2 = 0.38, ΔR2 = 0.09, F(1, 188) = 27.64, p < 0.001). In examining the standardized partial regression coefficients, being married, β= 0.20, t(193) = 2.73, p < 0.01; educational attainment, β= 0.24, t(193) = 3.25, p < 0.001; and epilepsy severity, β= – 0.34, t(193) = – 5.26, p < 0.001, were found to contribute significantly to the variation in life satisfaction scores after controlling for the effect of the demographic variables in the model. It appears that seizures and epilepsy related symptoms are significant daily stressors that negatively affect life satisfaction. Controlling for epilepsy severity and other demographic variables, being married and a higher level of education were still significant predictors of life satisfaction.
Environmental factors (social support from family and friends and perceived social stigma) were entered in the third step. Environmental factors accounted for a significant increase in the variation in life satisfaction scores beyond that explained by the demographic variables and epilepsy severity (R = 0.75, R2 = 0.56, ΔR2 = 0.17, F(3, 185) = 23.52, p < 0.001). In examining the standardized partial regression coefficients, being married, β= 0.16, t(193) = 2.54, p < 0.05, epilepsy severity, β= – 0.24, t(193) = – 3.89, p < 0.001, family support, β= – 0.52, t(193) = – 7.76, p < 0.001, friend support, β= 0.35, t(193) = 5.58, p < 0.001, and perceived social stigma, β= – 0.11, t(193) = – 1.99, p < 0.05 were found to contribute significantly to the variation in life satisfaction scores after controlling for the effect of the demographic variables and epilepsy severity. With the addition of environmental variables, educational attainment was no longer a significant predictor of life satisfaction. As expected, support from friends was associated with life satisfaction, and perceived social stigma had a negative effect on life satisfaction. In addition, family support was negatively related to life satisfaction.
Person factors (resilient personality, secure attachment, spirituality, epilepsy self-efficacy, and core self-evaluations) were entered in the fourth step. Person factors accounted for a significant increase in the variation in life satisfaction scores beyond that explained by the demographic variables, epilepsy severity, and environmental factors: R = 0.84, R2 = 0.71, ΔR2 = 0.15, F(5, 180) = 18.81, p < 0.001). In examining the standardized partial regression coefficients, family support, β= – 0.44, t(193) = – 7.18, p < 0.001, friends support, β= 0.15, t(193) = 2.72, p < 0.01, attachment, β= 0.11, t(193) = 2.01, p < 0.05, core self-evaluations, β= 0.29, t(193) = 4.13, p < 0.001, and resilient personality, β= 0.19, t(193) = 2.67, p < 0.01, were found to contribute significantly to the variation in life satisfaction scores after controlling for the effect of the demographic variables, epilepsy severity, and environmental variables. The effect of marital status, educational attainment, epilepsy severity and social stigma on life satisfaction dissipated in the presence of person-environment contextual variables. Supports from friends and family remained significant predictors of life satisfaction. Three of the person variables (attachment, core self-evaluations, and trait resilience) also significantly predicted life satisfaction in the final model. The person-environment variables accounted for 32% of the variation in the life satisfaction scores (f2 = 0.47, >0.35, a large effect size).
Transitioning into adulthood and facing stressors and challenges such as independent living, postsecondary education, healthcare, romantic relationships, employment and community participation can be difficult, particularly for persons with epilepsy. These stressors and challenges are further intensified because of stigma and discrimination that society continues to associate with epilepsy (Herrmann et al., 2016). Thus, it is crucial to assist young adults with epilepsy in developing resilience, self-efficacy, and coping resources to enable them to cope effectively with the psychological, social, and cultural demands of adulthood. Resilience is one of the most thoroughly investigated constructs in positive psychology (Catalano et al., 2011; Joyce et al., 2018). In general, research on resilience has demonstrated a strong relationship between resilience and life satisfaction (Ring et al., 2016). There are, however, many positive person-environment contextual factors that contribute to resilience, including core self-evaluations, support from friends, and access to resources and opportunities (Catalano et al., 2011; Smedema, 2014; Tansey et al., 2017). In the present study, we examined Kumpfer’s resilience constructs as predictors of life satisfaction. Findings of this study indicated that Kumpfer’s resilience framework model significantly predicted life satisfaction in young adults with epilepsy.
Specifically, marital status, educational attainment, epilepsy severity and symptoms, and social stigma were significant predictors of life satisfaction. Young adults with epilepsy who were married reported higher levels of life satisfaction than young adults with epilepsy who were not married. This finding is consistent with positive psychology research indicating that support received from spouses is a proxy for social connectedness (Burman & Margolin, 1992; Dehle et al., 2001; Diener et al., 2000; Elliott et al., 2011; Lachman & Weaver, 1998). Educational attainment was positively associated with life satisfaction, and severity of epilepsy was negatively related to life satisfaction. The tangible benefits of postsecondary education are well documented (O’Neill et al., 2015). A college education has both tangible and intangible benefits. It can increase the odds of getting a good job with benefits that provide career advancement opportunities. In addition to tangible benefits, the four-year college experience affords students with disabilities the opportunity for personal and professional growth including self-esteem, social skills, emotion efficacy, generalized self-efficacy, internal locus of control, vocational competence, and vocational outcome expectancy (Dutta et al., 2019). Couldridge, Kendall, and March (2001) conducted a systematic literature review to examine the medical impact and psychosocial effects of epilepsy. Findings indicated that education is a significant protective factor contributing to improved quality of life for people with epilepsy (Couldridge et al., 2001). In terms of seizure severity, particularly for individuals with active epilepsy, seizure frequency and seizure severity have been found to be strongly associated with life satisfaction (Jacoby & Baker, 2008; Jacoby et al., 1996). In the present study, approximately 71% of the participants were taking two or more anti-epileptic drugs (AEDs), which would be associated with greater severity of epilepsy, along with experiencing other unwanted symptoms. Results from the current study provide support to previous research, as increased seizure severity was predictive of lower levels of life satisfaction.
Epilepsy is a highly stigmatized disorder, and, because of the general ignorance about epilepsy, stigma and discrimination is still a major source of stress and limitations for persons with epilepsy (Herrmann et al., 2016; Jacoby et al., 1996; Jacoby & Baker, 2008). Findings from the current study are consistent with previous research on life satisfaction in the general population and for people with epilepsy (Kobau et al., 2012) with higher levels of stigma predicting lower levels of life satsifaction. Interestingly, the effects of these demographic and symptom severity variables (being married, educational attainment, and seizure severity) on life satisfaction dissipated in the presence of positive person-environment variables (secure attachment, core self-evaluations, trait resilience, spirituality, family, and friends support), supporting Kumpfer’s assertion that resilience is not merely a personality trait but a nomological network of resilience-related constructs.
In the present study, support from friends, secure attachment, core self-evaluations, and trait resilience were the most significant positive person-environment predictors after controlling for the effects of other variables in the regression model. A surprising finding was the negative effect of family support on life satisfaction. In the present study, high levels of family support were associated with lower levels of life satisfaction. An examination of the relationships among the demographic and epilepsy severity variables revealed that participants who rated high levels of social support from their families were more likely to be female, single, less educated, and with more severe seizures and symptoms. Therefore, these factors may be a proxy for severity of epilepsy and poverty, and partially explain the inverse relationship between family support and life satisfaction in our sample of young adults with epilepsy (Hesdorffer et al., 2005). Conversely, support from friends was positively associated with life satisfaction. Young adults with epilepsy who depend on friends for social support may be higher functioning and therefore more independent from their parents (Elliott et al., 2011).
Core self-evaluations is an important construct in applied psychology. Judge, Locke, Durham, and Kluger (1998) defined core self-evaluations as the overall, fundamental perception that people have about their worth and capability as human beings. It is a higher order positive human trait comprised of self-esteem, emotional stability, generalized self-efficacy, and internal locus of control (Judge et al., 2003). Judge and colleagues (1998) indicated that people who consider themselves to be good or competent will react differently to obstacles in life than individuals who believe they are incompetent, and core self-evaluations are predictive of job performance, job satisfaction, and life satisfaction. In the present study, core self-evaluations was the strongest predictor of life satisfaction among the positive person-environment variables, and these results provide support to previous research. A recent meta-analysis reported a strong relationship between trait resilience and big-five personality type. Resilience as a personality trait was moderately related to emotional stability, extraversion, openness and agreeableness (Oshio et al., 2018). In addition, secure adult attachment was related to a positive view of self and others, balanced needs for interpersonal closeness and independence, and healthy social adjustment, which also supports findings from the current study. Young adults with epilepsy with secure attachment are more socially skillful and socially connected, which can lead to higher levels of life satisfaction (Blake et al., 2018).
Limitations
There are several limitations that should be taken into consideration when interpreting results from this study. First, the sample was limited to participants who were involved with organizations such as Lily’s Fund and several chapters of the Epilepsy Foundation throughout the United States. Therefore, individuals who completed the survey could have more access to services through these non-profit affiliations, limiting the generalizability of the results to other young adults with epilepsy. In addition, because this study is a descriptive correlational study, causality of the relationships between predictor variables and the outcome variable of life satisfaction cannot be assumed. Concerns about selection bias are also important to note. There are nearly one million unique visitors to the Epilepsy Foundation website each month (“About Epilepsy,” 2017). Individuals who did not complete the online survey may have limited access to the internet, may not be familiar or comfortable with technology, or may be more susceptible to increased symptomology than the broader population of individuals who did participate in the current study, potentially biasing the findings toward persons with greater functional abilities and higher socioeconomic status. Additionally, data were collected based on self-report measures, making responses vulnerable to bias of recall, but the anonymity provided through the survey may have helped to limit bias due to social desirability.
Implications for vocational rehabilitation counseling practice
Findings from the present study have several implications for the professional practice of vocational rehabilitation counseling. In the present study, educational attainment was a significant predictor of life satisfaction. College, university, and vocational training are standard vocational rehabilitation services (O’Neill et al., 2015). For counselors who work with young adults with epilepsy who are motivated and have the academic abilities to complete a college education or vocational/technical school training, postsecondary education should be considered as a possible rehabilitation service option. Seizure severity also has a negative effect on life satisfaction. The CDC (2018) has developed several evidence-based self-management programs to help persons with epilepsy manage their conditions (https://www.cdc.gov/features/epilepsy-self-management/index.html). Rehabilitation counselors who work with young adults with epilepsy can use these epilepsy self-management interventions (treatment management, seizure management, and lifestyle management) to help their clients manage their conditions and improve functioning. In addition, secure attachment and social support from friends are important resilience related factors. However, it is not possible to recreate the secure bonding between people and their parents. One of the benefits of secure attachment is better social functioning as an adult. Helping young adults with epilepsy develop empathic and social self-efficacy could strengthen their social functioning and ability to develop friendships and positive relationships at work, leading to better quality of life (Sanchez, 2018).
Core self-evaluations was the most significant person-environment predictor of life satisfaction. There is emerging evidence to support the use of positive psychology interventions to improve core self-evaluations in rehabilitation counseling and psychology (Smedema, 2014). Judge and Kammeyer-Muller (2011) discussed the malleability of core self-evaluations and suggested that core self-evaluations could be improved through the use of positive feedback. They also recommended the use of positive psychology interventions to enhance self-esteem, generalized self-efficacy, internal locus of control, and emotional stability. For example, positive psychology research has demonstrated that people can increase their happiness through simple intentional positive activities (Lyubomirsky & Layous, 2013). Examples of empirically validated activities include writing letters to express gratitude, counting blessings, performing kind acts, cultivating strengths, visualizing ideal future selves, and meditating and mindfulness. All of these practices are brief, self-administered, and cost-effective. There are also specific resilience training programs. Joyce and colleagues (2018) conducted a meta-analysis to evaluate efficacy studies published in the positive psychology literature and concluded that resilience interventions based on a combination of cognitive-behavioral therapy and mindfulness techniques have a positive impact on individual resilience. Seligman, Steen, Park, and Peterson (2005) also developed a resilience training program, the Penn Resilience Program (PRP). Brunwasser, Gillham, and Kim (2009) conducted a meta-analytic review of the PRP’s effect on depression based on 17 controlled evaluations of PRP (N = 2498). They found evidence that PRP significantly reduces depressive symptoms through at least one year post-intervention. As a result, rehabilitation counselors can use programs such as the PRP to help young adults with epilepsy develop strengths in the person-environment factors identified in this study, which will help improve their psychosocial adjustment and employment outcomes.
Conclusion
In conclusion, findings of the present study strongly support the validity of Kumpfer’s (1999) resilience framework model. The results also validate the importance of including person-environment factors to operationalize resilience using a model approach. This model approach to define resilience can be used by rehabilitation counselors in case conceptualization, assessment, planning, and counseling. It can also be used to guide the development and validation of multi-faceted resilience interventions to help young adults with epilepsy develop confidence, capability, and self-worth in order to improve their educational, employment, and relationship outcomes.
Conflict of interest
None to report.