
Abstract
BACKGROUND:
Disclosing a severe mental illness (SMI) and serious criminal offence is often challenging for forensic mental health (FMH) consumers when applying for vocational occupations.
OBJECTIVE:
This qualitative research aimed to explore the experiences of FMH consumers disclosing sensitive information, to better understand the facilitators and barriers that occur.
METHODS:
Nine FMH consumers were purposively selected, the main criteria for inclusion being previous experience of disclosure related to work or study. Two focus groups and a one-to-one interview were recorded, and data were transcribed verbatim and analysed using descriptive thematic coding.
RESULTS:
Two overall themes emerged: 1) ‘Experiences of disclosure’ and 2) ‘Participants’ suggestions for change’. Sub-themes for experiences included risks, levels and strategies for disclosure, challenges and frustrations, positive experiences and inadvertent disclosure. Participants suggested individualised disclosure support, simple and practical tools to explain disclosure in different scenarios, skills for managing rejection, discharged forensic consumers acting as mentors and an increased understanding of disclosure issues by clinical staff.
CONCLUSIONS:
The findings of this research provide important insights for health professionals into the lived experience of FMH consumers when disclosing for vocational occupations and highlight the need for more in-depth training of FMH staff to better support consumers in navigating disclosure.
Introduction
Forensic mental health (FMH) is the specialised area of health care for individuals who have been found not guilty, or not fit to be tried, of committing an offence (O’Donahoo & Simmonds, 2016) whilst experiencing severe mental illness (SMI), for example schizophrenia (McNeill & Bannigan, 2014). The crime is usually of a serious personal nature, such as homicide (Ogloff & Taylor, 2010; Stuart et al., 2017) and the person is held in a secure facility such as a specialised forensic hospital, or in some countries, prison.
The aim of this study was to understand the experiences of FMH consumers during disclosure of their criminal history and mental illness when applying for vocational occupations (paid employment, volunteering, further education). Disclosure is a difficult conundrum for people with mental illness in general and more so for people with a forensic history (Goldberg et al., 2005). Knowledge of barriers and enablers regarding disclosure could inform health professionals when offering support in this area.
Literature review
A literature search was undertaken using CINAHL, AMED, psychINFO, OTDBase and OTSeeker databases and was later broadened to include the Cochrane database, discounting time limits and further search terms. Whilst several articles related to disclosure, there were none specific to FMH consumers who had a serious criminal history such as homicide, had also experienced a SMI such as schizophrenia, and were seeking re-entry into work or education.
Stigma and vocational occupation
Mezey, Youngman, Kretzschmar and White (2016) describe stigma as alienation of an individual by the public due to “unacceptable” characteristics. The FMH population often face a ‘dual stigma’ when disclosing information related to mental illness and violent crime on entering the workforce or further education (Aresti et al., 2010; Coffey, 2012; McQueen & Turner, 2012; Mezey et al., 2016; Stuart et al., 2017; Tregoweth et al., 2012).
Only two studies on dual stigma were found. Mezey et al. (2016) used the self-reported Discrimination and Stigma Scale [DISC-12], created by Brohan et al. (2013), with 64 participants in the UK who had schizophrenia or schizo-affective disorder, half of whom had a forensic history. All participants experienced stigma which specifically damaged close relationships, such as with family and friends. However, there was minimal difference in stigmatisation between those who had committed a crime and those who had not. One conclusion was that the public are either more fearful of the word ‘schizophrenia’ than an offence history or that the prejudice against FMH consumers is less than thought, due to the lengthy inpatient stay and rehabilitation process (Mezey et al., 2016). However, applicability of this study may be limited, in that 22% of the FMH consumers had committed a property offence (Mezey et al., 2016), as opposed to participants in the current study, where the majority have committed violent offences.
The second study by Perkins, Raines, Tschopp and Warner (2009) interviewed 404 adults from one community in Delaware, USA, to investigate the type of prejudice the public have toward adult males with a diagnosis of schizophrenia. The participants were given four short scenarios regarding a 25-year-old fictitious male with schizophrenia. These scenarios included the character being employed or unemployed and having committed a minor or serious offence. The participants were requested to indicate how they would feel interacting socially with the individual described.
The findings revealed beliefs that if the character had committed a serious crime he would be more likely to hurt others, but if he was employed and had committed a minor offence, he would be a more valuable member of society (Perkins et al., 2009). Furthermore, participants felt the same about the employed character who had committed a serious crime and the unemployed character with a minor offence record, suggesting there is less stigma felt toward those who have an offence record and schizophrenia, but are employed. Perkins et al. (2009) suggested that increasing FMH consumers’ awareness of self-perception and advocacy skills would result in more positive vocational outcomes. Concurrently, public education should be designed to reduce prejudice and enable employment opportunities for this marginalised population.
These two studies serve to indicate that people can be impacted by dual stigmas in vocational and relational areas of life. The study by Perkins et al. (2009) serves to show that employment is a factor that moderates or reduces stigma, although it is not always predictable.
Disclosure when seeking or applying for vocational occupations
Tregoweth et al. (2012) interviewed four males and four females regarding their experiences of re-entering the workforce after an extended time in a forensic hospital in New Zealand. The participants all had a SMI such as schizophrenia, schizo-affective disorder, or bipolar disorder. They had committed a range of crimes from property theft to human assault, and all had been employed for a minimum of six months in the previous ten years. Participants acknowledged disclosure was complicated and confronting, and pre-disclosure training was considered necessary (Tregoweth et al., 2012). Although vocational occupation allowed participants to develop their knowledge and self-confidence, this coincided with issues such as stigma and the complexity of disclosure.
A qualitative study by Aresti et al. (2010), in which five ex-offenders were interviewed regarding their change in perception of self, found that not only did the participants feel stigmatised by the past, they were apprehensive of future rebuff following disclosure. This had led to avoidance of disclosure until they judged rejection was less likely to occur. The authors asserted that choosing not to disclose a past criminal history allows the individual to maintain higher self-esteem and retain a sense of belonging within society; both traits that contribute to overall wellbeing. Although this study is useful for the purpose of understanding disclosure experiences, the participants were not identified as having a mental illness.
While these studies demonstrate that disclosure is a complex issue and can be a cause of anxiety, there may also be positive aspects of disclosing. For example, if a consumer displays honesty, this could result in increased support from employers, such as offering flexible work options and could decrease stigma (Hielscher & Waghorn, 2015).
Rationale for research
Given the limited research, this study aimed to explore the lived experience of FMH consumers when disclosing their criminal history and mental health needs for vocational occupations, to better understand their perspectives, barriers and enablers. This research aimed to provide much-needed insight to increase health professionals’ understanding of disclosure issues and provide consumer-driven suggestions for changes to practice.
Research questions included: What are the experiences of FMH consumers regarding disclosure for vocational occupations? What has helped to support FMH consumers to prepare for disclosure? What changes would FMH consumers like to see in relation to support for disclosure?
Methods
Qualitative research provides an insight into the perspectives of participants and sheds light on their actual lived experience (Luborsky & Lysack, 2006). According to Creswell (2013) and Liamputtong (2013), qualitative research is also suited to gathering information from marginalised groups of people who might not usually have the opportunity to share their experiences. Therefore, as this research sought to explore the experiences of FMH consumers, a qualitative methodology was adopted. Procedures were followed in accordance with the ethical standards of the Monash University Human Research Ethics’ Committee and Forensicare Operational Research Committee.
Participants and recruitment methods
Purposive and convenience sampling (Liamputtong, 2009) were used by health professionals to identify 18 consumers at a secure forensic hospital and community forensic service in Australia as possibly being eligible for the project.
Inclusion criteria were English speaking FMH consumers over 18 years, who were working, seeking paid or unpaid work, applying for or undertaking education. Experiencing acute symptoms of mental illness was an exclusion criteria, and was determined by the relevant clinical staff. A total of nine participants were included (Fig. 1).
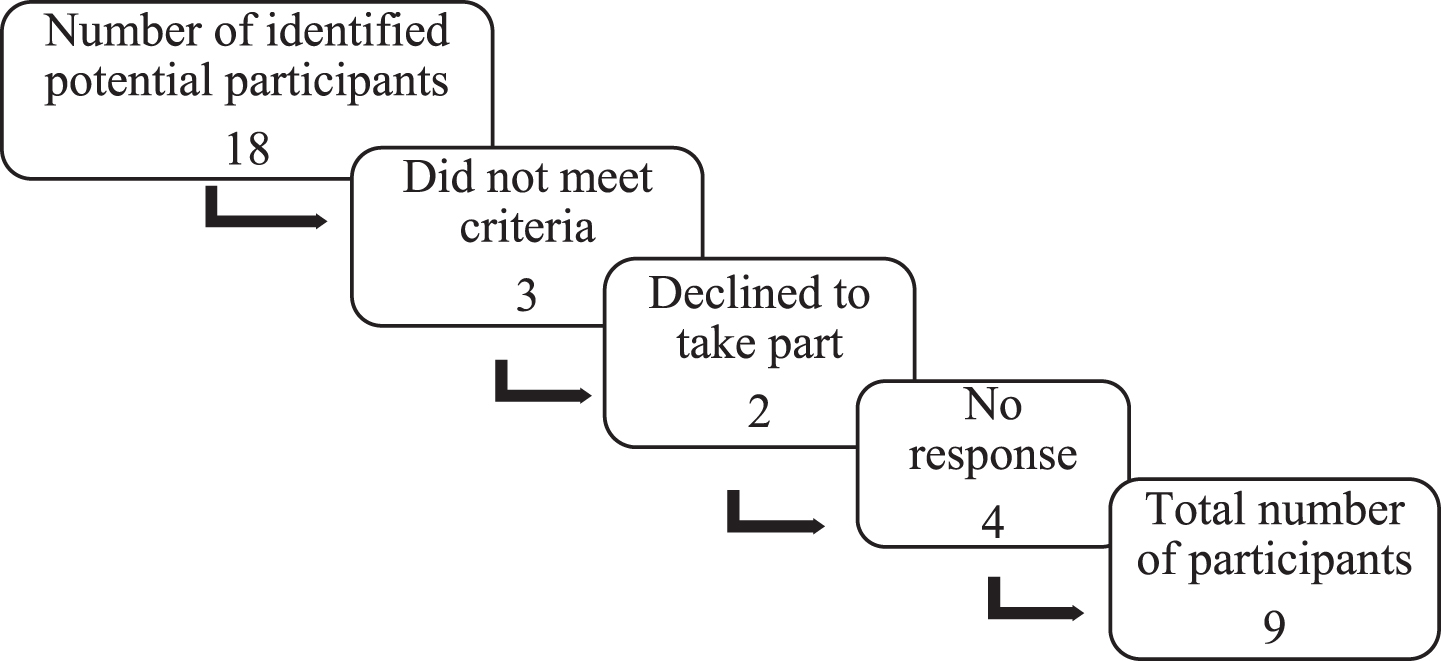
Recruitment of Participants.
Krefting (1991) described immersion and prolonged engagement in the setting as a method of providing research rigour and trustworthiness. The primary author spent 165 hours in the setting prior to data gathering, building rapport with staff and patients and being involved in therapeutic group sessions.
Once written consent had been provided, two one hour focus groups were held; one with five participants in the hospital rehabilitation unit and the second with three participants at the community forensic service. An interview took place in the hospital sub-acute unit. A note-taker, not known to participants, was present at each focus group.
A short demographic questionnaire was given to each participant before recording the discussion. Semi-structured open-ended questions following a broad to narrow trajectory (Halcomb et al., 2007) were asked, to allow the participants to become familiar with each other before the more sensitive topics were addressed (Davidson et al., 2013; Halcomb et al., 2007).
Data analysis
Fossey, Harvey, McDermott and Davidson (2002) explain the importance of using descriptive analysis when illustrating the findings of a study, to enable the reader to understand the life story and perspectives of the participants. Therefore, this methodology was adopted to identify, examine and interpret the data.
Participants were invited to review transcribed discussions to confirm their accuracy, diminish any potential power relationship (Creswell, 2013; Fossey et al., 2002; Kuper et al., 2008) and increase the credibility of the research (Davidson et al., 2013). All participants were satisfied with the transcription.
Triangulation of data was incorporated through the second and third authors reviewing and agreeing with the themes and categories, utilising notes made during the focus groups and an audit trail, including documents such as reflective journals (Kuper et al., 2008).
Results
Background of participants
Participants included one female and eight males. Pseudonyms were selected to support anonymity. The demographic survey provided context for the study, such as the highest year completed at school, length of time since previous work (Table 1), further study and past employment history (Fig. 2).
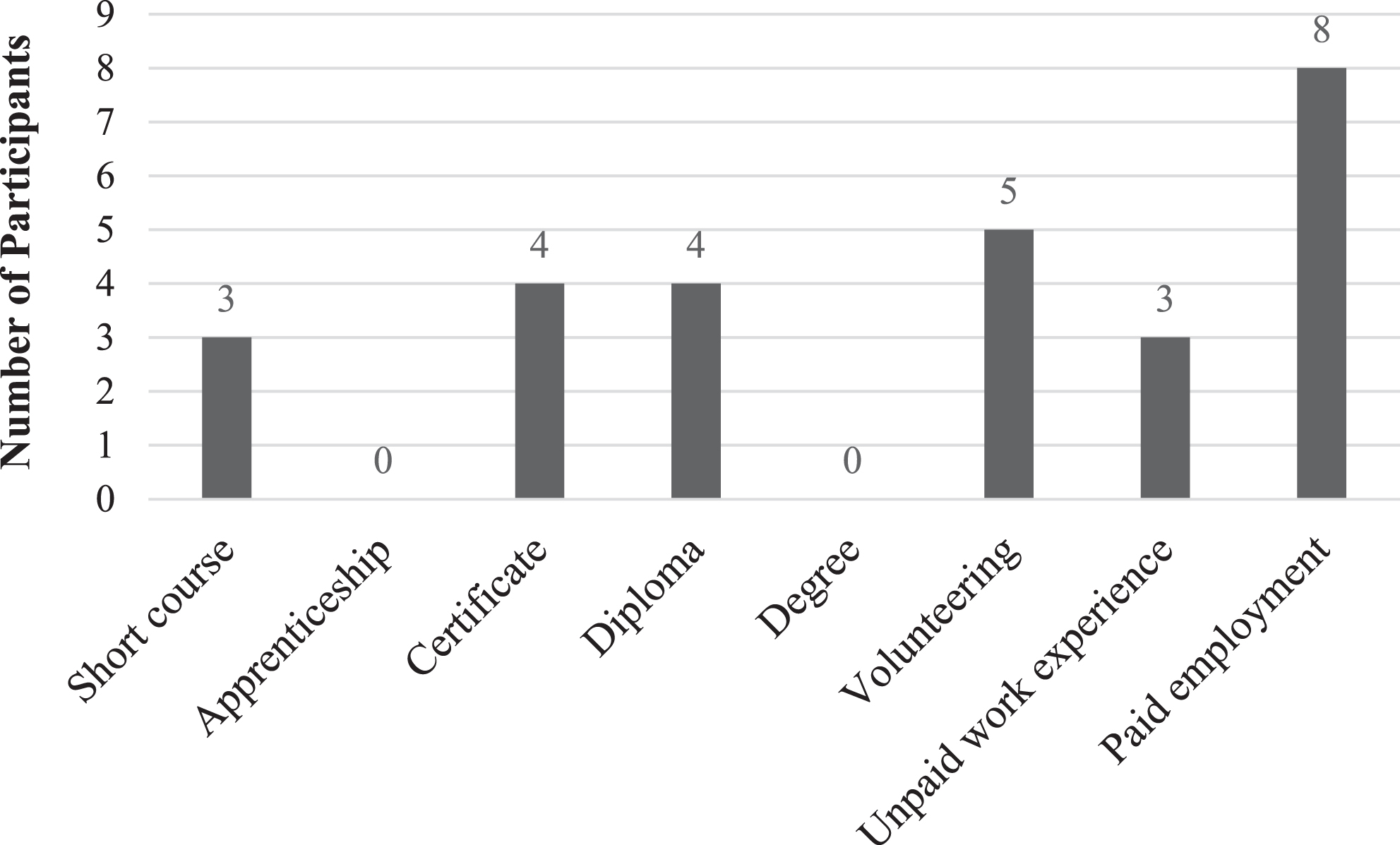
Participants’ Further Education and Work Experience, Inclusive of Before and After their Offence.
Description of Participants
Two overall themes emerged as a result of data analysis: “Experiences of disclosure” and “Participants’ suggestions for change”. There were twelve sub-themes in total (Fig. 3). For the purpose of this publication a selection of sub-themes from each theme will be described. On occasion, ‘anonymous’ has been used in place of a pseudonym, where comments were potentially identifying.
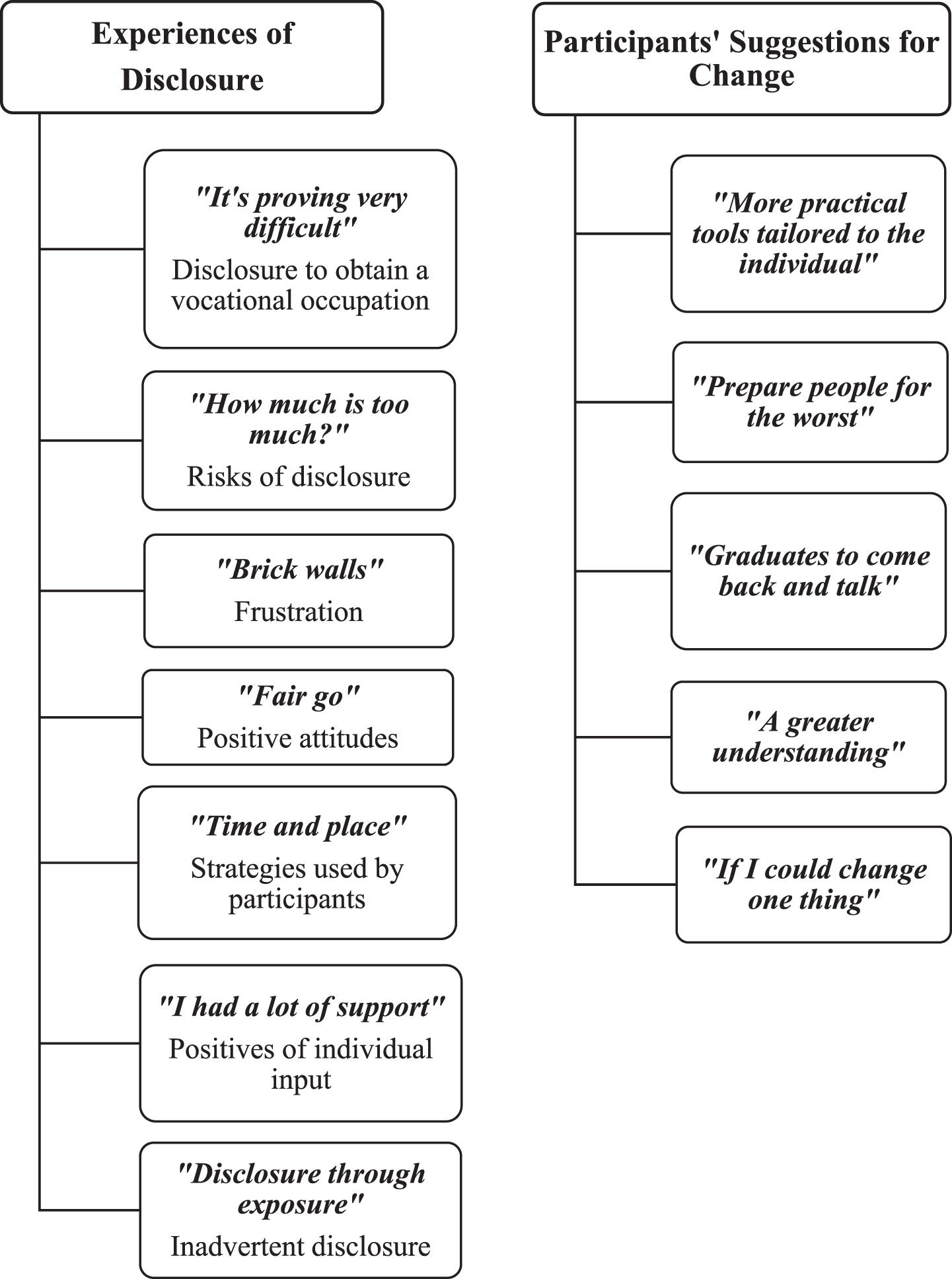
Themes and Sub-Themes.
The first theme incorporated seven sub-themes that related to outcomes of disclosure. When asked about their experiences with disclosure, participants described some positive, but mostly negative, reactions. Very few disclosures were received empathetically. Different strategies for disclosure were described by participants, with an unexpected issue; that of inadvertent disclosure by clinical staff. Three sub-themes, “It’s proving very difficult”, “Time and place” and “Disclosure through exposure” will be outlined, using participant quotations.
A further obstacle to gaining employment or participating in education was the institutional restriction associated with off-campus leave, such as curfew times and number of outings permissible in one week. Those participants who have transitioned from the hospital into the community (known as ‘extended leave’) must keep appointments with clinicians and case managers, causing potential difficulties in fulfilling work or study commitments.
The gap in work history on the resume of a FMH consumer risks probing questions by potential employers. As Shannon said, “When they ask, ‘What’s your experience and what have you been doing for the past five to ten years?”’, this can lead to ‘forced’ disclosure, or the person not wishing to divulge further information and making something up, rousing suspicion and resulting in rejection.
Stigma related to criminal issues was implied as the main problem in obtaining work by David, who stated, “It’s a bit of a process getting into the workforce. So you throw this place [forensic hospital] into ... the picture and it becomes really difficult.”
The negativity experienced by the community focus group appeared to have resulted in immense frustration. Charlie explained how they are affected:
I think because we’ve come such a long way through the hospital, our expectations of ourselves are a lot greater than they were... prior to the offence. So when people... write you off or think something negative of you, cos you’ve been in the hospital or you committed an offence or you’ve got a mental illness, it hits you a lot harder cos, like, all the work we’ve done and continue to do ... it seems like it’s not recognised. Like, for some people it’s never going to be enough. No matter how much treatment, rehab, time stable,... once they hear those words, they’re gonna instantly cast judgment and it’s really hard for people like us, because we’ve tried so hard and we’ve put a lot of effort into getting better and staying on the right track.
Participants’ past experiences appeared to contribute to an overall expectation of the inevitability of rejection following disclosure. Reinforced by media and social networking commentaries, this has had a negative outcome resulting in discouragement, illustrated by Charlie who stated, “It’s hard to get going when sometimes all you’re hitting is brick walls”.
Much of the discussion with the community-based participants also included the topic of FMH case managers. Although disability job agencies had been involved in assisting consumers to find work, participants were frustrated by having experienced case managers contacting potential employers and disclosing more than they wanted. Conversely, Charlie explained how having a disability job agency being involved when applying for work could be used to help:
... They are a buffer between [case managers] and the employer, so [disclosure] is more ‘need to know’ for the employer dealing with the job agency... the agency was well aware of my offence and my, um, illness and they sorta try and get you into employment, so they’re not gonna, you know, shoot you in the foot before you get there.
Participants talked about the complexity of disclosure, describing it as having “three different levels” (Morgan) dependent on who they were talking to, such as an employer, colleague, educational supervisor, peer or friend. These levels were: 1) Non-disclosure/lying, 2) Partial disclosure (of only the mental illness) and 3) Full disclosure of both the mental illness and previous offence.
Partial disclosure was mentioned as being favourable in some circumstances, due to mental illness appearing to be generally ‘accepted’ today (Charlie). Morgan explained how constructing a new perspective on this had helped disclosure feel more authentic:
I needed to reframe because I have a lot of shame about being at [forensic hospital], or, or had a lot of shame... and the stigmatisation that goes with being a forensic patient ... then I could honestly disclose in a way that was more just. By that I mean ... if somebody asks about my situation... I never say I’ve got schizophrenia. Um, what I say... is “I’ve got a serious and complex medical condition that is being treated and is in remission”. And ... people can just accept it... they don’t usually probe.
‘Full’ disclosure of both mental illness and a serious offence during interviews for paid work appeared to have only resulted in negative responses, whereas educational institutions and unpaid work placements were more supportive. Morgan described a positive experience on disclosing at a work placement: “I said ‘I’m at [forensic hospital] and he said [the employer], ‘We’ve all had issues”’.
In terms of being trained or supported by health professionals to prepare for disclosure in various situations, aside from Morgan who stated he had “worked hard to build a plan”, participants appeared to “think on the spot” (Jason). There was a strong feeling among all participants that, as Shannon stated, disclosure “depends on what you’re comfortable with”.
There was discussion in the two groups about a local shopping strip being a “thoroughfare for [forensic hospital] patients” (Shannon), as many patients are escorted there when commencing off-campus leave. Morgan referred to this as the “baptism of fire”. As many staff wear uniform when escorting or visiting consumers on work placements, Jason pointed out that, “Everyone wonders, no matter where you go ... you’ve got two people ... escorting one person ... obviously there’s some sort of danger”. Morgan suggested, “If this hospital is taking people into the community, the staff should dress in civilian clothes”. This was met with mutual agreement by the other participants.
The group also acknowledged that various shopkeepers know their FMH history and raised concern that their names could be noted from their payment cards and subsequently looked up on the internet. Some participants mentioned wanting to have their images and previous criminal history removed from the internet, to prevent potential employers, peers and friends from being able to find their criminal histories.
Theme two: Participants’ suggestions for change
Participants suggested changes that could be made to improve disclosure support and “aid re-integration into society” (Morgan).
I thought they would give you an example of something like, “This is how you answer this if someone says, ‘Where do you live?”’ They had an answer and it was something like, “I live in a community with other people who also need help like I do” and I thought, “Why would you say that? That’s just going to trigger off 20 questions, like; ‘Oh, what help do you need?”’
Leigh gave an example of advice they were given to, “Just say you live in [suburb] if anyone asks”. The risk of this response backfiring on the patient was then described by Leigh: “Oh, whereabouts? I live in [same suburb]! How much rent do you pay? Who do you live with? We should catch up!” The overall opinion of the participants was that great care is needed in constructing answers, to avoid further probing questions.
Shannon described how consumers had taken part in disclosure role plays within an occupational therapy group session, but that the reality of the situation within the community was different:
Nothing can prepare you for when you’re in that moment ... when you’re in that position, your heart’s racing and you’re thinking ... you know, all these things are going through your head, “Oh I can say this, this and this, but I can’t say this, this and this”.
I know it’s like, pessimistic, but really getting people prepared for the worst... so that way if you’re rejected for a job... how do you cope with that? And then if the outcome’s better, well it’s a win-win.
This comment was met with mutual agreement and Shannon suggested health professionals could “boost up that self-esteem and confidence... to handle those situations”. Charlie then explained further:
Knowing how to take the negative reaction. I mean,... it’s hard. It’s always gonna be hard but ... there might be some easier ways to look at things or reframe things in your mind... to take the sting out of it, you know?
Discussion
This research sought to understand the experiences of FMH consumers when disclosing their mental illness and/or offence for the purpose of participating in a vocational occupation, whether disclosure support has been helpful, and changes consumers would like to see in relation to disclosure. It was conducted to provide information for health professionals to better support FMH consumers in preparing for disclosure and to contribute to the limited literature on this topic.
Experiences of disclosure
The experiences of disclosure for FMH consumers were predominantly negative. Participants displayed a level of frustration and pessimism due to their experiences or expectation of negative reactions to disclosure, leading to a sense of futility, decreased self-efficacy, lack of confidence and fear of saying ‘the wrong thing’. This has resulted in participants feeling that lying, or covering up the ‘whole’ truth, is warranted, leading to further reactions of confusion, embarrassment and guilt (Brohan et al., 2013). Although participants had qualifications and/or work experience, stigma surrounding FMH consumers appeared to be an obstacle to participating in vocational occupations.
Conversely, when participants had experienced a positive disclosure encounter with employers, these stories were narrated in a more animated manner, often with a smile, indicating the beneficial impact this had on their self-efficacy. This is in line with the findings of Dunn, Wewiorski and Rogers (2008), who discuss the traits of “pride, self-esteem and empowerment” (p.61) experienced by participants as a result of being employed.
Participants varied in their levels of understanding the importance of having a disclosure strategy, underlining how complicated it is, and that there has been a lack of structured support related to preparing for disclosure. For example, participants described the difficulty faced with knowing how much information to disclose in a given situation, particularly to potential employers or close acquaintances.
Participants’ suggestions for change
Participants appeared to have varying attitudes toward disclosure for vocational occupations and would like support to be tailored to their specific needs and preferences. They requested assistance with knowing how to cope with rejection on disclosure. This suggestion is congruent with Thornicroft et al. (2009) and Tregoweth et al. (2012), where the authors stated there was an expectation of failure from consumers.
Tschopp, Perkins, Hart-Katuin, Born and Holt (2007) interviewed FMH service providers and found that building resilience and instilling hope into consumers was important when considering applying for work. Participants suggested one approach for addressing this would be to invite FMH consumers residing in the community to talk with inpatients about their experiences of disclosure. However, caution is advised in selecting and preparing candidates for such peer support, as these consumers may also have experienced negative reactions on disclosure, therefore a balance between reality and hope would need to be communicated.
Strengths
The first author was immersed in the FMH setting during the year in which this project was completed, thus enabling richer data to be gained through having a good understanding of the environment. Rapport had been built with some members of the focus group on the rehabilitation unit, which perhaps led to participants feeling more ‘comfortable’ to talk.
As the first author was a university student rather than employee of the forensic setting for the purpose of this research, the risk of bias was greatly reduced.
The findings of this research provide health professionals with insight into the barriers and facilitators FMH consumers experience in relation to disclosure for vocational occupation. Being better informed about their lived experience will allow professionals to better support FMH consumers in preparing for and managing disclosure.
Limitations
Although Morgan (1997) suggests that research can be less biased if participants are not known to each other, this is not viable within a supervisory context such as a forensic hospital, However, he points out that familiarity of the participants can contribute to a more relaxed environment which encourages richer data to be gathered.
Limitations of this research are that it took place within one setting and involved a limited number of participants, none of which were culturally and linguistically diverse (CALD), and that results of qualitative research are not transferable to other populations (Minichiello, Aroni & Hays, 2008). Additionally, the research specifically related to disclosure for vocational occupations, however, it was evident that broader issues of disclosure are a priority for FMH consumers, for example when shopping or socialising.
Implications for practice
Being able to disclose within vocational and community settings was important to participants and it is recommended that staff involved with psychiatric rehabilitation are familiar with potential disclosure scenarios and are equipped to support consumers to prepare for these situations.
Participants felt inadvertent disclosure occurs through conversations between community case managers and potential employers, where more information is divulged than has been permitted by consumers. It is recommended that case managers seek guidance on disclosure conversation techniques and gain consent from the consumer as to what information can be shared.
Given concern of disclosure by exposure, it is recommended that staff consider wearing an outer layer to cover their uniform when escorting off-campus leave or visiting consumers on work placement. They should also be mindful not to initiate interaction when unexpectedly crossing paths with consumers in the community as this could lead to inadvertent disclosure, for example, if the consumer is with a friend or peer who is not aware of their FMH status.
Although participants stated that support had been welcomed and was helpful, the tools offered need refining. Specifically, the participants suggested a simple booklet with potential disclosure scenarios. This request is congruent with the point made by Cotterill (2014), that it is important language used by clinicians/health professionals is free of jargon, so recipients can understand what is being said, or written. For example, diagrams or pictures could be used to break up the text. Creation of video scenarios was also suggested by participants.
Participants were keen to have a mentor program, where previous inpatients come back to discuss disclosure experiences and techniques and suggested this could be part of the required transition program into the community.
A few participants discussed whether their offence history could be removed from the Google search engine, as this allows unwanted disclosure. This could be further investigated by FMH professionals and, if possible, consumers supported to apply for removal of web-based sensitive material.
Future revision of resources to support disclosure and staff training as a result of this research would be beneficial.
A final implication for practice is for staff to be aware that consumers may feel as though they are not trusted, or their hard work during recovery is not recognised due to the requirement of regular work visits or feedback from employers or lecturers. It is recommended that consumers are encouraged and praised for a ‘job well done’. However, obligations relating to preparation of court reports and their organisation’s responsibility to minimise risk to the community should also be explained, so that FMH consumers clearly understand the expectations placed upon staff.
Conclusion
This research sought to understand FMH consumers’ experiences, support given and suggestions for improving support when disclosing for vocational occupations, with a view to better equipping forensic mental health professionals to provide assistance in this area.
Stigma, whether encountered or anticipated, plays a big part in discouraging this marginalised population from seeking employment or education, leading consumers to experience low self-efficacy and hopelessness. Media and social networking are significant propagators of stigma, where people with schizophrenic illnesses are painted as being potentially violent and dangerous human beings. In combination with possible mandatory police or working with children checks, some FMH consumers may feel there is little hope of obtaining a vocational occupation.
Despite this, most participants appeared motivated to seek employment or study. Staff who provide support with disclosure should advise on when it is most appropriate to disclose, how to accept rejection and how to remain positive. Care needs to be taken by staff when communicating with potential employers, that ‘too much information’ is not disclosed.
Recommendations for future research
Exploring the experiences of a broader range of participants from other FMH settings would provide a more comprehensive picture of the experience of disclosing both a mental illness and criminal history. Including a wider range of stakeholders, such as health professionals and prospective employers would provide further perspective on aspects such as the experience of providing disclosure support and how recipients of disclosure perceive FMH consumers.
As disclosure for more general community participation also appeared to be challenging for the participants, this “social disclosure” could be explored further, including exploration of “forced” or inadvertent disclosure to friends, acquaintances and community members.
Finally, it may be useful to explore the experiences of and techniques used by FMH consumers who have achieved successful re-entry to vocational occupations following positive disclosure.
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Acknowledgments
We would like to thank the participants involved in this study for their willingness to share about their experiences.