
Abstract
BACKGROUND:
Social skills deficits may hinder learning, terminate relationships, and impede employment. Many individuals with autism and intellectual disability experience difficulties in social judgement, emotional regulation, and interpersonal relationships, all of which can lead to disruptive and aggressive behaviors. Explicit instruction, video modeling, and video feedback are research-based practices that have been used to teach conversation skills to individuals with developmental disabilities and social impairments.
OBJECTIVE:
This study examined the effects of explicit instruction combined with video modeling and video feedback in teaching conversation-initiation skills to six adults ages 18–20 with autism and intellectual disability in a post-high school transition program.
METHODS:
A multiple baseline across dyads design was used, with number of correct initiation responses as the independent variable. The independent variable was an intervention package including explicit verbal instruction with interspersed video modeling clips, followed by video feedback.
RESULTS:
All six participants acquired the skills and were able to initiate a conversation; five of them maintained these skills over time, demonstrating them without the intervention.
CONCLUSIONS:
Data supported a evidence functional relation between the intervention package and the participants’ social initiation skills. Social validity responses indicated that participants enjoyed watching the videos of models and especially enjoyed watching the videos of themselves.
Background
Competent social interaction requires complex skills affecting many facets of life, especially for individuals with disabilities including social impairments. Intellectual disability (ID) is often associated with difficulties in social judgement, emotional regulation, and interpersonal relationships, all of which can lead to disruptive and aggressive behaviors (American Psychiatric Association [APA], 2013). Individuals with autism spectrum disorder (ASD) frequently demonstrate inappropriate attempts to gain attention which are also aggressive or disruptive (APA, 2013). Instances of aggression and withdrawal were connected to having few positive social interactions (Monahan & Booth-LaForce, 2016). In a report from the National Longitudinal Transition Study-2 (Wagner et al., 2003), youth with disabilities are more likely to be reported by parents as never having made friends easily, or joined groups of their own accord, or felt confident in social situations as compared to typically developing peers and youth. These social skills deficits may hinder learning and lead to social isolation, poor adult psychosocial functioning, and negative health consequences (APA, 2013).
Social skills deficits
For some individuals with disabilities, deficits in social functioning negatively impact social adjustments and relationships (Hsiao et al., 2013). Although individuals with ASD or ID commonly have limitations in social communication, they desire friendships (Jobe & White, 2007). Unfortunately, challenges with social skills can negatively impact the quantity and quality of those relationships, increasing loneliness (Jobe & White, 2007). Social reclusiveness has been linked to aggressive, confrontational, and self-destructive behavior in children and adults (Monahan & Booth-LaForce, 2016).
In contrast, positive relationships with peers can be a gauge of cognitive and emotional development, supporting adaptive behaviors that are essential for individuals to live a happy and meaningful life, which involves interpersonal relationships, community engagement, and employment (Carter et al., 2010; Monahan & Booth-LaForce, 2016). Research has established that competence in social exchanges is a major component of academic success and school engagement in addition to employment (Kindermann, 2007). In a study completed by Ju, Shang, and Pacha (2012), the area of social skills was ranked among the five most important skill areas among employers. Youth with little to no difficulty communicating with others were found to be three to four times more likely to be employed after school than those with lower communication skills (Carter et al., 2012). Youth with disabilities are further disadvantaged when applying for employment as many lack soft skills necessary in the work place (Lindsay et al., 2014). Henry and Lucca (2004) also found effective social skills as a facilitator to meaningful employment.
The deficits in interpersonal communication skills typical of individuals with ASD or ID make initiating and maintaining a conversation particularly difficult (APA, 2013). One study found that individuals with ASD have a low likelihood of engaging in listener-oriented conversation (Lake et al., 2011). Similarly for individuals with ID, impairments in social skills affect their communication across communication partners (Carter et al., 2010).
Tantam (2003)v has reported that early communication deficits do not subside as individuals get older but may deteriorate further during adolescence because of the increased complexity of the students’ social environment. If individuals with social difficulties do not receive support, communication deficits may limit functioning in daily life activities across home, school, community, and work environments. Creating effective, socially valid techniques to teach social skills to adolescents and adults with disabilities may contribute to their success and inclusion in all aspects of daily life.
Explicit instruction
Explicit or direct instruction has been identified as an effective strategy for teaching individuals with disabilities (Marchand-Martella et al., 2005; Swanson, 1999; White, 1988). This strategy uses clear, unambiguous language to achieve student understanding and maximize responding (Kinder & Carnine, 1991). Learning targets are broken down into small components via task analysis, and rules are taught simply and explicitly. Another important feature of direct instruction is brisk pacing of questions and error correction procedures. Principles of reinforcement and assessment are incorporated as well.
Direct instruction has been used to teach and improve receptive and expressive language skills for individuals with developmental delay (Waldron-Soler et al., 2002). Waldron-Soler et al. examined the effects of a direct instruction program on children’s social adjustment abilities and found that teacher-directed instruction in which students respond to instructions, questions, and cues achieved statistically significant and meaningful effects on social skills, problem behaviors, and academic competence among participants with disabilities.
In another study, Banda and Hart (2010) used direct instruction to increase peer-to-peer interactions of two elementary students with ASD. When participants were trained to initiate and respond to one another, results indicated increased socializations in both participants, suggesting that socialization can be improved using explicit instruction. Kroeger, Schultz, and Newsom (2007) compared group-delivered programs to teach play and social skills to 25 young children with ASD using direct instruction for one group and naturalistic for the other. Researchers found not only that direct instruction was effective in teaching prosocial behavior but that its gains were greater than those with naturalist teaching.
Thus direct instruction has been effective in teaching social skills to children with disabilities; however, few studies have examined its effect on adolescents or adults with ASD or ID. Although children with disabilities can acquire a wide variety of social skills through direct instruction, these skills may fail to generalize or be maintained as age increases (Weiss & Harris, 2001). Video-based instruction has been identified by research with the potential to facilitate the learning of individuals with disabilities.
Video modeling
Video Modeling (VM) is an evidence-based practice that has been effective in teaching social skills to students with disabilities (Laver & Wilkes-Gillan, 2018). VM enables an individual to learn a new skill by watching a video of someone else demonstrating the behavior. After watching the video, the student is prompted to imitate the task (Kellems & Edwards, 2016; Van Laarhoven et al., 2010). Previous studies have used VM to increase the use of language and communication skills and to improve social initiations and interactions among children and adolescents with disabilities (Bellini & Akullian, 2007; Rayner et al., 2009).
Nikopoulos and Keenan (2007) examined the effects of VM to teach social initiation and other behaviors to three children with ASD. Results demonstrated a functional relation between the VM and social initiation skills: All children improved performance after the VM intervention, and behavior changes were generalized and maintained. In another study MacDonald et al. (2005) used VM to teach children with ASD to engage in reciprocal play with non-disabled peers. Scripted play scenarios were filmed and shown to the participants before play. Results indicated that ability to engage in reciprocal play of both typically developing peers and children with ASD increased immediately and maintained over time. Unscripted verbalizations also increased as a result of the VM procedure.
As with direct instruction, several studies have examined the effects of VM on teaching social skills to children with disabilities such as ASD (Reichow & Volkmar, 2010), but less research has applied VM to adolescents or adults as the primary population. For example, of the 66 intervention studies examined in Reichow and Volkmar’s (2010) meta-analysis of social skills interventions for individuals with autism, only three targeted adolescents or adults. To help correct this deficit, Rayner et al. (2009) suggested that further research be conducted to determine which salient components of VM interventions are most effective for the adult population.
Recently some researchers have responded to this suggestion of Rayner et al. (2009), and VM has been a component of different intervention packages for teaching specific aspects of conversation skills to adolescents with disabilities. For example, O’Handley et al. (2015) found VM effective for increasing eye contact during conversation for six males between the ages of 16 and 19 with ID and/or ASD. Additionally, O’Handley et al. (2016) examined the effectiveness of the Superheroes Social Skills intervention program (Jenson et al., 2011), which includes VM, in teaching four adolescent males the social skills of expressing wants and needs, initiating conversation, and taking turns. Though originally designed for children, Superheroes Social Skills was effective in improving socialization skills for these adolescent participants (O’Handley et al., 2016). As limited research has examined effectiveness of VM intervention packages with adult populations (Rayner et al., 2009), further study in this area is necessary.
VM alone may not be successful in eliciting desired changes in behavior (Reichow & Volkmar, 2010). The successful Superheroes package incorporates components such as animated videos, role playing, and behavioral skills training; thus differentiating effectiveness of an individual component such as VM is particularly difficult (O’Handley et al., 2016). The success of this program may have been due to the combination of strategies (Shukla-Mehta et al., 2010). Incorporating other strategies with VM may increase an intervention’s overall effectiveness.
Video feedback
Video feedback (VFB) involves filming the participant’s performance and having the participant watch the video with an instructor, evaluate the behavior, and look for areas for improvement (Mainoe & Mirenda, 2006). VFB is suggested to provide individuals with more accurate feedback than verbal comments (Booth & Fairbank, 1984), but to date limited research has examined the VFB effectiveness in teaching social skills.
Although few studies have been conducted using VFB, the method has shown promise for teaching socialization skills to individuals with disabilities. Mainoe and Mirenda (2006) used VM with VFB to teach appropriate social language during play activities with peers to a five-year-old boy with ASD. The VFB plus prompting package was incorporated when the child was fixated with the toy cars presented in one of the three play activities. The child increased his social language intervention, but it was impossible to tell whether it was the VFB or prompting alone that had been most effective (Mainoe & Mirenda, 2006). While video results involving feedback interventions are encouraging, further study is needed to examine specific causality.
Thiemann and Goldstein (2001) used a VFB intervention package to teach five students with ASD to engage in social communication with non-disabled peers. Treatment included social stories, text cues, and pictures of socials skills in addition to the video evaluations. Data demonstrated an increase in social interaction after self-evaluation using VFB, supporting the efficacy of VFB to teach social skills to children with disabilities.
VFB has also been used to teach social employment skills to adults with disabilities. Barnes (2014) used VFB to increase eye contact during job interviews for transition-age adults with ASD. Participants were given job listing information and asked ten questions during filmed interviews that were reviewed for eye contact. Participants were considered successful if they engaged in eye contact for more than 50% of the session. Results indicated VFB was an effective and socially valid intervention to increase the percentage of time the three adult participants with ASD engaged in eye contact during mock interviews.
Because VM and VFB have successful in teaching social skills to children and a few adolescents with a variety of disabilities, this study hypothesized that a VM and VFB, combined with explicit instruction, intervention package may be effective in teaching social initiation skills to adults with ID and ASD. Further research is needed to identify (a) if a video-based intervention package is effective in increasing initiation among adults with these disabilities, (b) which if either component is most salient, and (c) whether a video-based treatment is socially valid among this population.
Objective
The purpose of the present study was to explore and develop evidence-based interventions to teach conversation skills to adults with disabilities in order to improve their social effectiveness. Explicit instruction, VM, and VFB were incorporated to determine whether using these strategies together would help adults with disabilities to initiate conversations successfully. Two research questions guided the study: What are the effects of combining explicit instruction with video modeling and video feedback in teaching adults with disabilities to initiate a conversation? How socially valid is an intervention package consisting of explicit instruction, video modeling, and video feedback for teaching adults with developmental disabilities to initiate a conversation?
Methods
Participants
The six individuals participating in the study all had an active IEP while attending a transition program for students ages 18–21 in a suburban school district in Western U.S. Ranging in age from 18 to 20, all had been diagnosed with either ID or ASD. They were referred by their teachers based on whether they met study criteria and would potentially benefit from the skills taught. Participant criteria included (a) being on an active IEP, (b) having adequate expressive and receptive verbal ability to complete the intervention without use of a communication device, (c) being able to speak and understand the English language, and (d) being able to attend visually and cognitively to the videos. Participant information is found in Table 1, including the standard scores for communication and social skills sections of assessments previously given.
Participant Information
Participant Information
Note. Communication and social functions are reported as standard scores. *No other testing information available. Wechlser Adult Intelligence Scales, 4th edition, bWoodcock Johnson Tests of Cognitive Abilities, 3rd edition, cStanford-Binet Intelligence Scales, 4th edition, dStanford-Binet Intelligence Scales, 5th edition.
Procedures involving experiments on human subjects were conducted in accord with the ethical standards of the institutional review board (IRB) at the university where the researchers are employed. Participant and parent or guardian consent were obtained prior to beginning the study. Participants were given pseudonyms to protect confidentiality.
In the school where the study took place, one of four different rooms was used for data collection, depending on availability: a conference room, the cafeteria, a small library, and a mock apartment. Settings were always quiet and undisturbed. Participants were brought to each setting in randomized and alternating dyads to converse. Multiple seating options were available in each setting at a table either next to or across from a communicative partner. Participants were able to choose their own seat.
At least two researchers were present throughout each session. One sat near the participants, conducted the instruction, and collected data on initiations of one participant. The other sat at the opposite end of the table or room and collected initiation data on the second participant, but was not involved in the intervention in any other way.
Tasks materials and equipment
Initiating a conversation was selected for instruction, as it is a fundamental component of social interaction (Kavale & Mostert, 2004). A video was developed for each of the discrete components within the target task, including being an arm’s length away, vocalizing loudly enough to be heard, demonstrating nonverbal cues, and waiting for a response. Two researchers acted as models in the videos, selected for familiarity with the task and similarity in age and appearance to the participants. Prior to beginning baseline data collection, the models were filmed iniating a conversation exactly as the students would be taught and asked to do it. Using this video as a reference, a task analysis was developed, outlining every step of the conversation skill. Data collection sheets were developed based on the task analysis. The performing researcher again video recorded the task, using the task analysis as a script to ensure every step was accurately included in each intervention video. Table 3 identifies the steps in the task analysis.
The videos were edited with iMovie® and uploaded into the VideoTote app (The Prevention Group, 2012). The video modeling examples were delivered via a second-generation iPad Mini,TM supported at an angle landscape style by an OtterBox Defender Case for iPad MiniTM during instruction.
Intervention
Participants were designated as numbers 1–6, with numbers drawn at random from a cup and placed as different dyads during baseline, intervention, and maintenance phases to create conversation partners. Although conversation partners were randomized and alternated throughout all phases of the study, a participant who had moved into intervention was no longer paired with one who was still in baseline. Students were paired only with partners in the same stage of the study to prevent carryover effects. The intervention consisted of three components: explicit instruction, video modeling, and video feedback.
Explicit instruction: Initial scripts
The direct instruction lessons were initially developed using principles of instructional design (e.g., model-lead-test format) to allow sufficient scaffolding of information for the teacher to organize and activate knowledge while sustaining high engagement (Coyne et al., 2011). Lessons were validated by outside special education experts to ensure content accuracy. Each lesson began with explicit verbal instruction by a researcher, outlining and explaining specific steps to perform in appropriately starting a conversation (see Table 2). These initial scripts were then enhanced with video modeling examples, guided practice, and video feedback, in accordance with accepted techniques.
Steps for Initiating a Conversation
Steps for Initiating a Conversation
Five video clips were interspersed throughout instruction, one to illustrate each of the discrete social skills involved in starting a conversation, including both examples and non-examples; the five totaled 31 seconds. Between video segments, researchers verbally and physically emphasized parts of the video that participants would later be asked to perform. For example, the researcher might point while saying, “Notice how she is looking up right there. He is making eye contact!” During non-example videos, researchers emphasized inappropriate demonstrations of the target task: perhaps pointing and saying, “Look at her body language. Notice how she is uncomfortable because her partner is too close and too loud.”
Explicit instruction: Guided practice
Following the model-lead-test format of direct instruction, guided practice was conducted. In guided practice, participants were asked to apply with a partner what they had seen in the videos about starting a conversation. Researchers prompted this practice as appropriate based on each participant’s skill levels, following a least-to-most prompting hierarchy. Some students needed verbal and even physical prompting to complete each of the five steps in the task analysis. Others required minimal or no prompting.
Video feedback
Once students reached 100% accuracy in guided practice, they would move on to independent practice, during which they would practice the skills with their partner, as in guided practice, but without any help or prompting from researchers. During this interaction, researchers would video record the participants on an additional iPad. Following independent practice, participants were shown the recording of their interaction and given feedback on their performance. Researchers highlighted and praised correct steps completed and emphasized areas for improvement. Students with 80% or above accuracy were praised and encouraged for specific steps they had completed well. Students with a score below 80% were asked to practice again the specific aspect(s) that had been difficult for them. Following this additional practice, the session was complete, and students were asked to return to their regular class.
Data collection
Data were collected simultaneously with or immediately following participants’ demonstration or non-demonstration of a conversation. During each session two researchers, one focused on each conversation partner, used a hard copy data collection sheet laying out the task analysis to record data on the dependent variable, the number of steps the participant completed correctly, noting correct and incorrect independent responses. Table 3 lists steps in the task analysis.
Task Analysis of Targeted Skill
Task Analysis of Targeted Skill
Data collected on conversations of the randomized dyads were recorded, graphed, and analyzed. After one or two data points for a dyad had been collected, a probe was given to all other dyads to confirm the baseline before a subsequent dyad moved to the intervention phase. The researchers collected data only for initiations and reciprications between participants; they did not record any conversation initiations made to researchers.
During baseline, researchers selected a pair of students and began with the following explanation: “We need your help. Can you come with us?” Participants were brought individually from their respective classrooms and led to one of the four areas of instruction. If the participants asked questions, researchers were to reply, “We can’t answer questions right now, but we can talk about it later,” or “We will be in this room. Remember, I’m not allowed to talk to you while we’re in this room.” If the two students did not initiate in one minute, researchers dismissed them by saying, “Thanks. We have what we need, and we will do this again another time. You can go back to class.” Baseline procedures were designed without prompting so that conversations would be spontaneous and natural. Some participants did attempt to initiate conversation with their partner, as shown in Fig. 1.
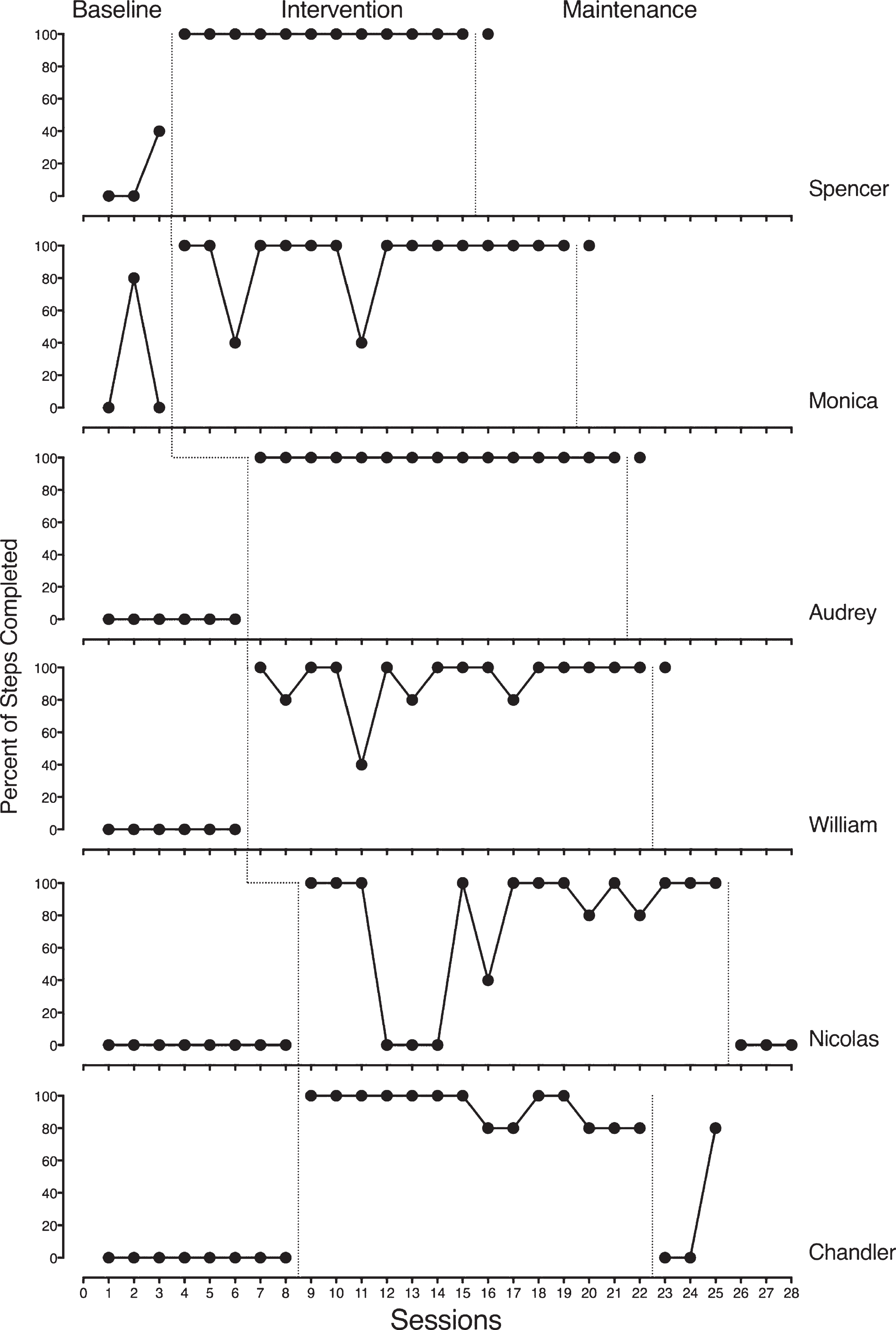
Participant results.
Intervention procedures were video recorded to later review for interobserver agreement. The camera was in a far corner of the room, away from participants and instruction. As participants were brought to a designated instructional area, an explanation was offered: “We need your help. We’re going to have a lesson. Can you come with us?” The session would begin with the lesson plan of explicit instruction for initiating a conversation, with the designated video modeling clip played on an instructional iPad as appropriate.
Following the direct instruction procedures, the lesson continued as participants were guided to practice starting a conversation with each other, with support of the researchers as necessary. Once students had correctly completed the steps for initiating a conversation with at least 80% accuracy, they were prompted to start another conversation on their own. This conversation was video recorded by a researcher. Data were collected either simultaneously or immediately following this independent attempt.
After independent practice, the researcher continued with VFB procedures by playing back the video recording for participants to view. Specific praise was given to participants who correctly demonstrated the conversation skill, and specific feedback was also offered if they did not demonstrate all components. Participants who had reached criterion independently were released to go back to their regular classroom; those who had not were prompted to have another conversation with each other.
Maintenance phase followed the same procedures as baseline. No instruction, videos, or directions were provided to participants other than the same request: “We need your help. Can you come with us?” Participants were scored if they spontaneously initiated a conversation with their partner. Those who did not initiate within one minute were dismissed, and data collection was recorded as zero percentage of steps completed correctly.
The researchers used a multiple baseline across dyads design to determine the effects of the intervention package on conversations initiated between pairs of students with disabilities. They paired participants randomly for each baseline session to ensure that partnerships were always different. After baseline data collection, they assigned participants randomly to create new dyads. Because all participants’ baseline scores were equivalent, researchers randomly selected one dyad to begin the intervention phase. Once the first group demonstrated skill acquisition, a stable baseline was collected on the second dyad, and a probe was conducted on the third. To demonstrate task mastery, each participant had to complete at least 80% of the five steps correctly for each session three times. To prevent participants who had received the intervention from teaching the target skills to participants still in baseline, the researchers did not co-mingle participants in different phases. However, a participant who had received the intervention could be paired with any of the other participants in subsequent intervention sessions.
To optimize generalization, four different researchers rotated leading instruction in four different settings within the school. Communication partners were also alternated to help promote generalization among participants.
Interobserver agreement and procedural fidelity
To discern interobserver agreement (IOA), additional researchers scored video recordings of 30% of the sessions. IOA was calculated as 93.03%, by dividing the number of agreements by the total number of agreements plus disagreements and multiplying by 100.
The mean agreement was 94.15% during baseline and maintenance conditions and 90.83% during intervention. Mean agreement was calculated for individual students across conditions: Spencer, 90.00%; Audrey, 100.00%; Nicolas, 90.00%; Monica, 100.00%; Chandler, 88.33%; and William, 93.33%.
To maintain procedural reliability, during all sessions of all phases the researchers followed a checklist outlining each step required to implement the intervention as designed. Checklists ensured that the same setting, equipment, and materials were used for each participant for every session. Some specific checklist items included manipulating the room so that participants would be likely to face each other and ensuring that researchers were always in their designated areas. The checklist specified that only one minute of waiting time was available for participants to start a conversation. To calculate the procedural reliability level during all the intervention sessions, the number of correctly completed steps was divided by the total number of steps and multiplied by 100. The data collected from the procedural reliability checklist was 100% across all participants and settings. Table 4 outlines the fidelity checklist.
Treatment Fidelity Checklist
Treatment Fidelity Checklist
The purpose of this study was to measure effects of a video modeling intervention package on the conversation initiation skills of adults ages 18–21 with ASD or ID. Figure 1 presents data representing the performance of each participant. The graphs are set up in a multiple baseline across dyads, with each panel representing one participant and each dyad representing one leg of the multiple baselines. A description of each graph is included below, along with Tau-U effect size estimates to supplement the visual analysis of the graphic data.
Participant performance
The first dyad consisted of Spencer and Monica. During baseline Spencer demonstrated none of the steps for initiating a conversation during the first two sessions, increasing to under 40% of the steps for the third session and returning to zero for the final three baseline attempts. When introduced to the intervention, Spencer completed 100% of the conversation initiation steps during each session. Spencer’s improvement from baseline to intervention demonstrates an immediate change in the level, trend, and variability of the data. These data produced a large Tau-U effect size estimate of 1.00. In one maintenance session Spencer demonstrated 100% of the steps, affirming the initial durability of the intervention effects.
In baseline Monica’s behavior was highly variable, with two data points at zero, one at 80%, and three more at zero. When the intervention began, Monica completed no conversation initiation steps during the first two sessions, but in the third session she demonstrated 100% of the steps and continued to do so for the remainder of the intervention with the exception of the ninth session, when her performance dropped to 40%. Researchers noted extraneous variables which could account for the significant one-time drop in her performance. Monica’s data demonstrated a change in level and variability, although the effect of the intervention was delayed. These data produced a large Tau-U effect size of 0.95. In maintenance, Monica again completed 100% of the steps, indicating initial durability of the intervention effect.
Audrey and William comprised the second dyad. In baseline Audrey completed none of the conversation initiation steps in any of the nine sessions, suggesting a very low and stable pattern. When exposed to the intervention, Audrey immediately performed 100% of the steps across all treatment sessions. This immediate increase in level suggested that the intervention was immediately and maximally effective. The Tau-U effect size estimate was 1.00, suggesting a large effect size. This level of attainment continued into the maintenance phase.
During the baseline phase, William demonstrated none of the conversation initiation steps across all seven sessions in which he participated, demonstrating a low and stable baseline. William began the intervention phase demonstrating 80% of the initiation steps, then vacillated between 80% and 100% of steps for the remainder of this phase—an immediate and pronounced increase in level. In the treatment phase, William’s performance became more variable but remained well above baseline levels. These data yielded a large Tau-U effect size estimate of 1.00. The effect of the intervention held for one maintenance session, indicating the initial durability of the intervention effect.
The last leg of the multiple baseline included Nicolas and Chandler. During the baseline phase, Nicolas demonstrated none of the steps of the conversation initiation skill across five sessions, a low and stable pattern of performance. When Nicolas began the intervention, his performance immediately advanced to 100%. His execution remained variable throughout the treatment sessions but ended at 100% across three sessions. These data produced a large Tau-U effect size estimate of 0.92. In the maintenance phase, Nicolas’ performance dropped to zero across three sessions, indicating a lack of durability of the intervention.
In baseline, Chandler demonstrated the same pattern of consistent zeros as his partner Nicolas. When he received the intervention, Chandler performed 100% of the steps across three sessions, then he completed between 80 and 100% of steps for the remainder of the treatment phase. These data demonstrate an immediate change in level and a slight increase in variability, with a large Tau-U effect size estimate 1.00. In maintenance, Chandler completed none of the steps for two sessions, but achieved 80% on the third.
Across all dyads, an effect was apparent three times, suggesting a functional relation between the video modeling instructional package and improved conversation initiation performance for the study participants. Additionally, the weighted Tau-U effect size estimate for the intervention was 0.93, suggesting a large effect size. Taken together, these data suggest that the VM intervention package was effective for increasing the conversation initiation skills of individuals with either ID or ASD.
Social validity
To measure the social validity of the study, researchers administered to each participant a verbal questionnaire with eight open-ended questions and two yes/no options. When asked what they thought of the lessons, half of the participants reported that they liked them. Three of the six enjoyed interacting with their partners during the practice part of the lesson, which they reported was their favorite part of each session. Two participants stated they did not like the parts when researchers were describing how to have a conversation and explaining the conversation steps.
Overall, participants said that they enjoyed watching videos on the iPad during the lessons, and some thought they were funny. Participants especially enjoyed watching themselves during the video feedback. Most participants felt that the video examples helped them learn how to start a conversation. Only one participant reported a conversation skill level that remained the same.
Most of the participants stated that they would like to watch more videos teaching them how to do things. Students provided ideas of topics they would be interested in for future video-based instruction lessons, including everyday school skills and job skills. Most students expressed interest in learning more specific conversation skills, such as showing affection, talking on the phone, and staying on topic.
Discussion
This study investigated the use of an intervention package that included explicit instruction, video modeling, and video feedback to teach conversation skills to six adults with ASD and ID. The results demonstrate that the intervention package was effective, as all six participants acquired the conversation skill and five of them maintained their ability to initiate a conversation after the intervention was withdrawn.
Limitations
During some of the baseline sessions, participants spontaneously initiated conversations with research assistants, which were not included in the percentages since baseline procedures were defined to record only attempts at initiation with the participant’s designated communication partner. Thus many participants demonstrated the skill of initiating a conversation with a similar-age peer, although their score was 0 with the partner who had a communication disability. This may have resulted in unrealistic baseline percentages.
Another limitation to the study was the shortage of maintenance data collected. Individual schedules and the end of school year prevented additional maintenance sessions. Although five of the six participants maintained conversation levels once the intervention was removed, retention over time could not be measured.
Although this study examines a high need area, the complextity of the intervention may make it challenging to replicate in the field. Research methods and overall research design, including the use of rotating dyads, contribute to the potential difficulty of replicating the current study. Future research may need to adjust methods and design to identify the effectiveness of the intervention package.
Implications for future research
Competent social skills can increase access to academic success, meaningful relationships, and fulfilling employment. A combined intervention package was successful in teaching six adults with ASD and ID to initiate a conversation with a peer who had comparable difficulties with social skills. From this study those who teach adults with disabilities can learn the effectiveness of teaching social skills using explicit instruction, video modeling, and video feedback. However, more research is necessary to identify a combined instructional approach as evidence based.
Future replications may be more socially valid if practitioners rely primarily on video instruction rather than including an explicit lesson. Further studies might benefit from identifying salient components of social skills instruction to adults with ID or ASD using VM and VFB. The authors also suggest monitoring the quality of conversations in future replications, as some participants may have only echoed initiation examples seen and heard in the videos.
Conclusion
This study explored the effects of an intervention package consisting of explicit instruction, VM, and VFB to teach conversation skills to adults with developmental disabilities to improve their conversation initiation ability. The researchers also verified the social validity of using these strategies as an intervention package to teach this skill. Results indicate a functional relationship between the intervention package and the participants’ social initiation skills, and five out of six participants maintained their ability to initiate a conversation after the intervention was withdrawn. Social validity responses indicated that participants enjoyed watching the videos of models and especially enjoyed watching the videos of themselves. Most participants also enjoyed the explicit instruction component of the intervention.
Conflict of interest
The authors declare that they have no conflict of interest.