
Abstract
BACKGROUND:
Early intervention vocational rehabilitation (EIVR) is used to optimize return to work (RTW) outcomes for people following spinal cord injury (SCI). However, theoretical clarity is required about how EIVR works, for whom and under what circumstances.
OBJECTIVE:
To develop a theoretical understanding of how people respond to EIVR following SCI and the contexts in which mechanisms of intervention effect are likely to be activated.
METHODS:
Realist research methods were used to analyze interviews with 30 participants who had received EIVR following SCI.
RESULTS:
We conceptualized the reporting of our analyses using a travel metaphor, encapsulating the types and degree of wayfinding support participants required to think about, plan and action their vocational aspirations. Developing, maintaining and enacting hope, supporting self-identity and vocational identity, and focusing on environmental context adaptations required to enact vocational aspirations, appear to be critical mechanisms of intervention effect within EIVR.
CONCLUSIONS:
Various contexts and mechanisms of EIVR contribute to successful negotiation, achievement and sustainability of RTW outcomes for people following SCI. These theoretical understandings can refine EIVR service provision within SCI rehabilitation and inform how EIVR can improve RTW outcomes for people with acquired neurological conditions in other rehabilitation contexts.
Keywords
Introduction
Return to paid work (RTW) for people with a new health condition is linked to increased wellbeing, quality of life and better physical and mental health outcomes (Waddell et al., 2006). Furthermore, RTW encourages full societal participation and independence (Waddell et al., 2006) and a feeling of ‘normality’ and productivity (Johansson & Tham, 2006).
In New Zealand (NZ), unemployment rates for disabled people (7.4%) are nearly double the rate for non-disabled people (3.9%) (Statistics NZ, 2020). For people who have experienced an SCI, paid employment rates remain below those of the general population of working adults (Dorsett & McLennan, 2019; Lidal et al., 2007; O’Neill & Dyson-Hudson, 2020). An earlier NZ SCI cohort study of 103 people followed up 18 months post-SCI found that, of the 84 people in paid work pre-SCI, only 35 (42%) had returned to work by 18 months (McAllister et al., 2013).
Vocational rehabilitation supports people to RTW following the onset of a new health condition (Fadyl et al., 2010; Waddell et al., 2008). Typically, vocational support is offered later in a person’s rehabilitation pathway after acute rehabilitation needs have been addressed (Middleton et al., 2015). However, it has been suggested that vocational support incorporated very early following the acquisition of a health condition can improve RTW rates (Krause et al., 2010; Middleton et al., 2015). Nevertheless, we have identified only six services worldwide that provide early intervention vocational rehabilitation (EIVR) within six months of SCI onset (Dunn, Hackney, et al., 2021). These services are based in NZ (NZ Spinal Trust Vocational Rehabilitation Service formerly known as Kaleidoscope; Hay-Smith et al., 2013); New South Wales, Australia (InVoc Progamme, in three spinal units; Middleton et al., 2015); Victoria, Australia (Hilton et al., 2017) and Switzerland (Parawork; Marti et al., 2017).
The NZ-based service, run by the NZ Spinal Trust Vocational Rehabilitation Service (previously named ‘Kaleidoscope’), is dedicated to supporting people to return to meaningful and sustainable employment following SCI. It uses a client-centric framework that fosters hope for RTW very early after injury, often within the first weeks of admission to a rehabilitation unit. Between 2018 and 2020, the NZ Spinal Trust delivered EIVR to approximately 100 people with newly acquired traumatic and non-traumatic SCI per year. This service is delivered by specialist vocational consultants based at the two spinal centres in NZ (Auckland and Christchurch). It provides early individual career coaching emphasizing personalized education designed to promote empowerment.
There is some evidence supporting an early intervention approach. For example, findings from the EIVR programme piloted in three spinal units in New South Wales suggested that implementing EIVR in the hospital setting had the potential to enhance RTW rates following SCI (Middleton et al., 2015). However, there is a need to understand how different people respond to the range of resources provided within an EIVR intervention. Such an understanding will allow for ongoing intervention development to achieve equitable and optimal RTW outcomes. A clearer understanding will also ensure that key mechanisms of effect are maintained when translating EIVR to different clinical populations and/or service contexts. Therefore, further research is needed to understand why EIVR works, for whom, and under what circumstances.
We conducted this study within a larger research project (‘Early vocational rehabilitation following neurological disability study’) which aims to better understand how people with acquired neurological impairments respond to an EIVR intervention and in what contexts key mechanisms of intervention effect were likely to be activated (Dunn, Martin, et al., 2021). Alongside this study, the larger research project also included a realist literature review (Dunn, Hackney, et al., 2021), an online survey of RTW outcomes for people following SCI (Snell et al., 2021), and focus groups with EIVR and other vocational providers. These data will collectively inform the development of mid-range theory (Salter & Kothari, 2014) to be used when developing an EIVR implementation plan for improving RTW outcomes for people with acquired neurological conditions other than SCI. This paper only reports on the findings of the interview data gathered from people following SCI.
Study objective
We sought to articulate deeper theoretical understandings of the various contexts and mechanisms contrbuting to the successful negotiation, achievement and sustainability of RTW outcomes for people following SCI as a result of receiving EIVR.
Methods
In this qualitative, cross-sectional study, we conducted one-on-one interviews with people experiencing SCI who had received EIVR via NZ Spinal Trust Vocational Rehabilitation Services. We used a realist research methodological approach (Emmel et al., 2018; Wong et al., 2012). Realist research approaches aim to develop deeper levels of explanation and understanding to produce ‘portable’ theories, which then contribute to further cycles of enquiry and ongoing theoretical development (Salter & Kothari, 2014). The ‘Early vocational rehabilitation following neurological disability study’ project, including this qualitative study, received ethical approval from the University of Otago Human Ethics Committee (ref H19/170).
Inclusion criteria
Interviews were conducted with participants who had sustained their SCI at least three months prior to the interview. Participants were included if they were NZ residents aged between 18 and 65 years at SCI onset (or wished to RTW after 65 years of age), had sustained an SCI resulting in admission to an NZ spinal unit for rehabilitation, were employed at the time of SCI, received EIVR services from the NZ Spinal Trust, and were able to participate in interviews in English.
Recruitment
Participants were purposively selected to ensure a representative sample. We included people who had and had not RTW, those with traumatic and non-traumatic SCI, participants who identified as Māori (the indigenous people of NZ), and those residing in rural and urban areas. Potential participants were identified by NZ Spinal Trust staff from their client database and invited by an NZ Spinal Trust staff member, via email and follow-up phone call, to participate in an interview. A research assistant (TY) contacted all those expressing interest in participation to check eligibility, ensure they had the study information, answer any questions and gain consent.
Data collection
Following recruitment, participants were interviewed by RM, who is experienced in both qualitative and realist research methods, including realist interviewing (Manzano, 2016). Interviews were conducted online via a video-conferencing system, or for inpatients, in the spinal unit. As well as interview questions specific to our research aim, we also collected demographic information, including personal, health and employment information, and living and financial situations. The interview guide (Appendix) was developed to explore how the participants experienced EIVR, their RTW pathways (if relevant), and the contexts that promoted, or not, the activation of mechanisms within EIVR. The questions remained flexible, with participants being asked to comment on activities and interactions during the provision of strategies or interventions that supported, or interfered with, RTW. Interviews were recorded on a digital recording device, transcribed verbatim and anonymized for analysis.
Data analysis
Interviews were coded independently by three team members (RM, JN and TY). Each transcript was read and re-read to gain a sense of the whole before manual line by line coding was undertaken. We gathered data under the following a priori determined code headings: (a) intervention resources, actions or tasks, (b) contextual factors, (c) mechanisms, and (d) outcomes. To focus on chains of causality, we paid particular attention to data extracts that provided evidence of links between these code headings. The researchers met to compare and debate their coding decisions on three occasions. We used manual diagramming to bring together, summarise and refine key context-mechanism-outcome configurations of the emerging theory. This was an iterative process involving ongoing analysis, conceptualization and refinement of theory. We also articulated those context-mechanism-outcome configurations as ‘if-then-because’ statements –that is, statements of the assumed context (if), outcome (then) and mechanism (because). To assist in articulating the developed theoretical understanding, we conceptualized the reporting of our analyses using a travel metaphor. The emerging analysis was also presented to EIVR providers and the broader research study team for feedback and ongoing refinement.
Results
Participants
A total of 30 people were interviewed (Table 1). The majority of participants (57%) were aged 46 to 60 years at the time of research participation (range 21 –67 years). Our sample included more males (67%) than females and averaged 51 years of age at the time of SCI. Two thirds (67%) of the participants were interviewed within 12 months following their SCI, and 43% (n = 13) were in part- or full-time employment at the time of the interview. Of the participants who were interviewed within one year of their SCI (n = 20), only five were working. In comparison, there were 10 participants interviewed who were > 12 months since their SCI, with almost all (n = 8) working. Interviews took between 21 –78 minutes.
Demographic and clinical characteristics of participants (N = 30)
Demographic and clinical characteristics of participants (N = 30)
Key: ASRU, Auckland Spinal Rehabilitation Unit, Auckland; BSU, Burwood Spinal Unit, Christchurch; SCI, spinal cord injury.
We have articulated our analyses using a travel metaphor, encapsulating the types and degree of wayfinding support participants required to think about, plan and take action towards their vocational aspirations following SCI. In this analysis, we have conceptualized EIVR providers as guides or navigators who facilitated a milieu, allowing participants to wayfind their own vocational futures while also providing targeted individual-directed support when appropriate. Figure 1 summarizes the various context-mechanism-outcome configurations and how these link to critical contexts. The critical contexts and context-mechanism-outcome configurations (referred to hereafter as CMO’s) are described in more detail below.
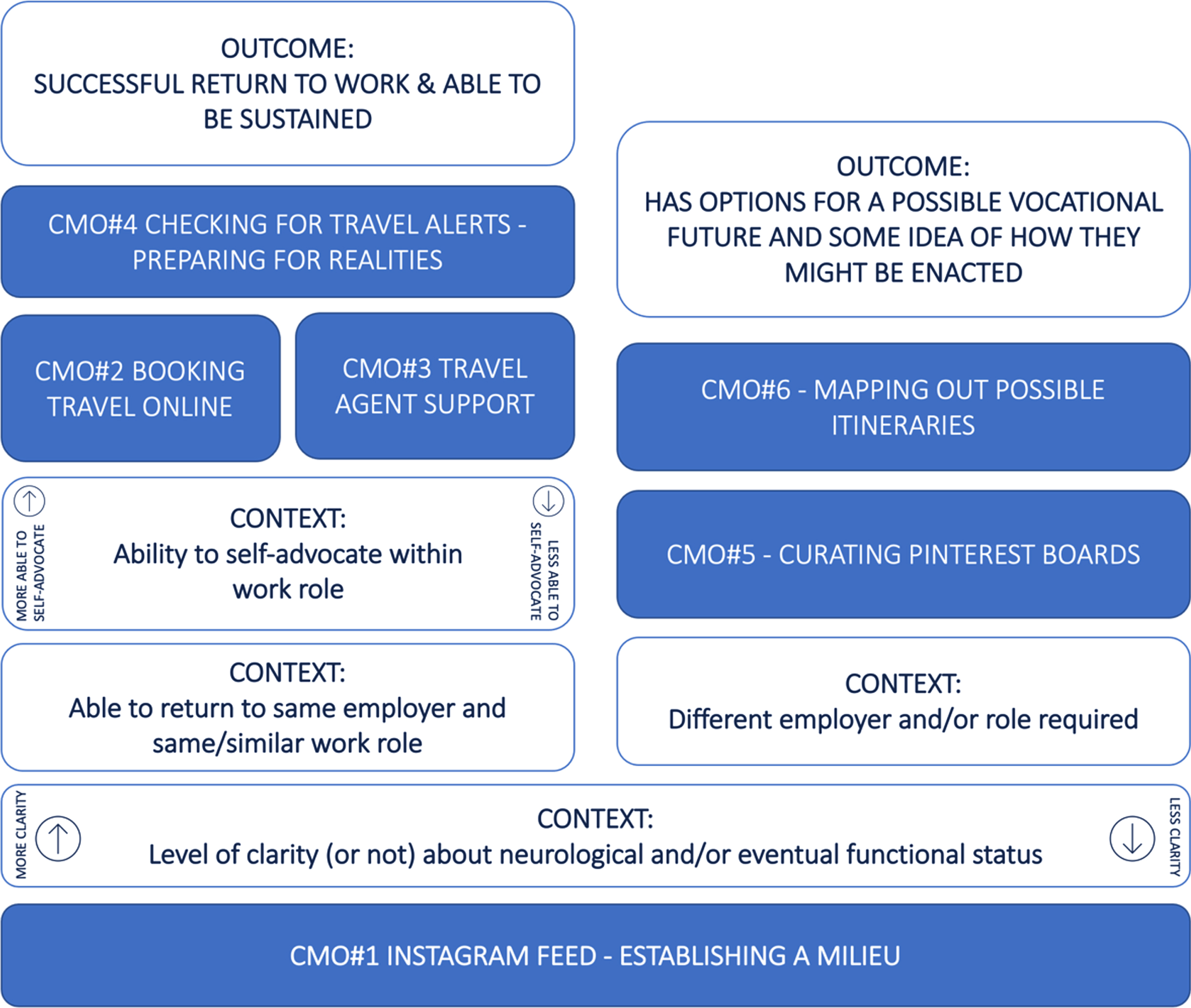
Overview of context-mechanism-outcome (CMO) configurations and the impact of critical contexts on the type of degree of wayfinding support required by participants.
EIVR was provided flexibly to participants in response to three critical contexts: the person’s level of clarity (or not) about neurological and eventual functional status, their ability to return to the same employer in the same or similar role, and the degree of decision-making influence they retained within their pre-SCI employment role.
Functional status clarity (Or not)
The nature of EIVR conversations offered by the EIVR providers before greater clarity emerged appeared to be aimed at relationship building, exploring vocational identity and fostering generic hope for RTW. This context is discussed more in CMO#1, in which lack of functioning clarity is a crucial context.
Ability (Or not) to return to the same or similar work role
If participants could return to their previous employer in the same or similar role, EIVR aimed to ensure that RTW was achieved and maintained over time. CMO’s #2, #3 and #4 are more applicable to participants in this context. If participants required a different employer or role, EIVR focused on providing them with options for a possible vocational future. Depending on psychological readiness and degree of clarity, EIVR supported the person with SCI to explore either a range of options that may work for their unique situation (CMO#5) or the development of work readiness, training or RTW plans (CMO#6).
Ability (Or not) to self-advocate within work role
The nature of EIVR resources offered to those who, before their SCI, were in a position of influence within their work role (CMO#2) were fundamentally different to those who had limited influence (CMO#3). However, a vital role for the EIVR providers across a range of contexts was ensuring that all parties were prepared for the realities of RTW, ensuring that expectations were realistic, potential challenges were anticipated, and strategies put in place (CMO#4).
CMO#1 curating an instagram feed - establishing a milieu
Participant’s narratives suggest that EIVR was focused on establishing relationships early in their rehabilitation, when they were experiencing a lack of clarity about future functioning and not prioritizing vocational issues within their constellation of concerns. This focus on relationship establishment facilitated a safe space to engage in future discussions about RTW. In this context, EIVR providers curated an ‘Instagram feed’ (i.e., a series of images that piqued interest and provided examples of a possible future) about what RTW might look like in general after an SCI. Within informal conversations, EIVR providers often included narratives about possible vocational roles for those who have experienced an SCI. These conversations aimed to foster a sense of hope by supporting participants to imagine a possible future and challenging expectations and assumptions about what was possible. Anxiety about the potential negative impacts of SCI on their vocational future was also reduced for some participants, allowing them to focus on their rehabilitation goals. These early conversations gave participants information about the type of vocationally-focused support available to them and was particularly helpful for those who felt less financially secure.
Conversations focused on establishing a relationship of trust, thereby curating a relational space in which the person with SCI can hear and engage with RTW messages at this very early stage.
Rather than just push on who she works for, or what she does, she sort of sat down and talked to you. [ ... ] She made time to get to know you. Rather than go, ‘Right, this is what I’m gonna do.’ [ ... ] I tell ya’, she could almost be a psychologist, that lady. Yeah, oh gosh, just how I was feeling, all those concerns, ‘How are things going?’ She’d always put your interests first. She was making sure that ‘OK, I don’t wanna go talking to this guy if he’s not in a very good space and he’s not feeling very well, or he feels like shit.’ So, I guess her approach was quite valued. [SCI09]
Participants experiences suggest that determining the most appropriate timing of EIVR was crucial. EIVR providers needed to take the time to listen and understand the degree to which the person with SCI could prioritize vocational issues within their broader constellation of concerns. If EIVR conversations moved to specific RTW plans too early, meaningful engagement was less likely to occur. Alternatively, if these conversations were not early enough, opportunities and self-belief related to achieving RTW outcomes could be lost. For instance, existing work roles could be lost due to a lack of information about possible RTW options.
The nature of the interactions was a crucial resource that impacted participant’s ability to respond to the EIVR intervention at this very early stage. There needed to be a strong focus on the person with SCI taking the lead and setting the pace within casual conversations with EIVR providers. Participants appeared to be able to best respond when EIVR conversations were linked into self-identity narratives. Understanding the person’s vocational identity, values, and motivations contributed to EIVR providers understanding who the participant was before their SCI, while also exploring how this sense of self could be maintained in future vocational roles.
Work at some stage, I think, is an incredibly important part of identifying yourself as normal. And meaningful work as well, not work that is made up so that you can feel part of a community because you can do something. [SCI14]
While conversations with EIVR providers fostered hope for work, RTW narratives within rehabilitation processes more generally (e.g., goal setting, rehabilitation planning) reinforced (or not) hope for successful RTW options for participants.
CMO#2 booking travel online
If the person with SCI had a pre-existing work role open, they could return to this role, and they were able to self-direct their RTW plan, then the person with SCI often perceived that they did not require EIVR support. Participants appeared to be able to self-advocate when they had a position of influence within their work role, higher levels of agency and higher perceived levels of workplace support.
I have a really good relationship with my work, so most of the things I just talk and I talk to my manager instead of asking [EIVR provider] to help because I [have] confidence that I can talk to him and then pick up, can negotiate and discuss the support I need. So yeah, I’m OK with that, yep. [SCI26]
However, participant experiences also suggested that EIVR reinforced the person’s cognitive and affective responses. The EIVR providers also supported RTW narratives within the rehabilitation planning process and provided information to address specific RTW questions or uncertainties. Therefore, in this context, EIVR supported RTW outcomes by supporting the work role to remain open and facilitating successful work environment modifications, including workplace (employer and colleague) attitudes. In this context, EIVR maintained the person’s levels of agency, confidence and capability, and if required, supported the maintenance of the occupation bond with the employer and vocational identity within the person with SCI.
[The EIVR provider] just maintained constant contact and just always had that thought of, ‘Look, when the time is right to actually start making a plan, we’ll make a plan,’ you know. But that initial contact was always good because it sowed a positive seed, you know, that this will be a plan, you know, ‘You will do this.’ [SCI23]
Another resource that participants frequently referenced in this context, and across other context-mechanism-outcome configurations, was the opportunity to talk to other people with SCI working within the rehabilitation unit. Seeing others with SCI in paid work roles provided strong messaging about the possibilities for work and allowed the participants with newly acquired SCI to access specific, trusted advice about what they might need to consider in their work context.
CMO#3 travel agent support
More active EIVR wayfinding support was provided if the person with SCI had a pre-existing work role open, but they were less able to self-direct their RTW plan. In this context, the resources provided to participants by EIVR included advocacy on behalf of the person with SCI, information about processes and entitlements, facilitation of rehabilitation team goals, rehabilitation planning to solve specific RTW barriers, and development of the RTW pathway, including providing information to address employer questions and uncertainties.
[The EIVR provider] is helping me [to stay in] contact to work and telling them what’s happening to me, and the job is still there. My bosses where I work, they kept ringing until now, to check if I’m OK. My job is still there for me, plus [the EIVR provider] messaged them or contacted them about and so I know the job is still there for me, and they told me that I can take my time, take my time until I feel completely ready to come back to work. [SCI11]
Participants experiences suggest that the proximal outcome was that the role was kept open and a RTW plan was developed for them. More distally, EIVR aimed to support participants to return to their pre-existing work role in the future. EIVR in this context ensured that successful modifications to work environmental and attitudinal contexts were made, employer knowledge was increased, and the expectations of employers and work colleagues were realistic. For people with SCI, EIVR increased levels of confidence, agency and capability that, in partnership with EIVR provider, they could develop RTW pathways.
Participant: Every time she contacts my employer, she’ll want me to come in there and have a chat about what they were talking about and ...
Interviewer: Did she encourage you to talk to your employer by yourself at all?
Participant: Yes, but she said if I, whenever it’s hard for me to do, then let her know, and then she’ll do it. [SCI08]
Participants with SCI were also able to maintain their occupational bond and vocational identity, and they experienced reduced anxiety about the future as explicit fears relating to this were addressed.
CMO#4 checking for travel alerts - preparing for realities
Resources provided as part of the EIVR intervention (e.g., conversations about work roles, workplace environments and graduated return to work planning) facilitated checking for unrealistic RTW expectations. These resources prepared the entire RTW team (including the person with SCI, family/whānau, employer and colleagues) for the likely RTW trajectories and the challenges that might emerge, thereby supporting the development and use of strategies for RTW. In a situation where incorrect or unrealistic expectations (either overly positive or negative) are held, EIVR endorsed the exploration of more realistic, and therefore sustainable, RTW plans. The long term outcome was for people with SCI to sustain their work roles, thereby preventing long-term disempowerment and loss of confidence in their ability to RTW.
Participant narratives suggested expectation checking was directed at a range of factors, including the type of role the person could get back to, challenges transitioning from the rehabilitation unit to home and how this transition may impact RTW plans, speed of graduated RTW hours, the impact of equipment provision delays on RTW, sustainability of hours over time, issues relates to work-life balance, and unrealistic expectations of self in relation to their colleagues and employer.
[The EIVR provider] basically told [the employer and work colleagues] what to expect and informed them of all the knowledge that she had of being in a wheelchair onto them, so they could understand what the situation was, so that they were fully informed what to expect from my injury. ... She was always very cautious not to push me very much, and she did express that to work, you know, ‘cos you know, she said, in fact, that you know, ‘As soon as she gets home, there’s gonna be changes, and it could be like starting all over again. It could be very difficult, so we need to do this very cautiously, as we go.’ [SCI19]
Resources provided by EIVR to facilitate expectation checking included sharing stories of other’s RTW pathways, providing information about potential barriers and/or enablers, providing a clear and specific RTW plan, and brainstorming particular strategies to draw on when needed. By changing perceptions and increasing awareness of future challenges, EIVR supported the development of solution-focused strategies, and increased the understanding of the person with SCI about their capabilities and strengths and their contribution in a future work role.
I was sort of asking her advice around kind of, how I should start and how long should it take to build up to a point where I’m either kind of part-time or heading towards full-time. So that was, that was really useful. So [the EIVR provider]’s kind of working out a bit of a plan for me; she was advising things like how that sort of balances with my fatigue from other things. [SCI33]
CMO#5 curating pinterest boards – planning for possible return to work destinations
As participants gained some clarity about their eventual functional status and it was likely that a new work role would be needed, they began to think about plausible vocational options that might work for them. In this context, EIVR can be conceptualized as the process of curating multiple Pinterest boards (i.e., similar to starting a mood board or an old-fashioned scrapbook) to collect ideas of possible RTW options and pathways, keeping in mind that their function may change over time. EIVR ensured that various vocational possibilities were collated so that the person with SCI could start to think about RTW destinations that might work for them. Options and expectations were explored, and plausible pathways were also identified, including finding information about training options, collating resources that would help find work, and providing information about RTW processes that may be followed in the future.
If I decide to do something, she’ll sort of look for ways that I can get there, so if I told her that I wanted to do forklift driving ... she’d probably help me get a course where I can sit my driver’s licence for full, and like get my ‘F’ endorsement. She will like definitely encourage me along the way to getting it, and, but she also opened me up to other ideas. ... She just helps me and encourages me on whatever idea I get, but she doesn’t let me like stray off track, like if I’m just going off track a bit, she’ll be like, ‘No, come back. You need to come back in line.’ [SCI06]
In this context, EIVR continued to be explicitly framed by participants as optimizing alignment with the persons pre-SCI self and their future work aspirations and preferences. Participants frequently contrasted this approach with vocational interventions provided later in their rehabilitation pathways, which focused on impairment levels and the types of work roles that someone with their level of functioning could do with minimal environmental modification.
I got a lot of inspiration off (the EIVR provider); you know, she always gave me the confidence that you can, you know, you can do whatever you want when you get out of here. You know, you just need to find what you want to do and you know, and it makes sense, and I think that people need to realize that if you’re in a job, you need to enjoy it, you’ve gotta love it, you know, or don’t do it, you know? So, and just getting all that sort of words like that from her, you know, the confidence. [SCI09]
In this context, key mechanisms activated by EIVR included developing optimism about participating in personally meaningful work, gathering ‘specific visions’ for a future self that aligns with their past self, and building self-efficacy in the person with SCI.
Hearing other people with spinal cord injuries or other disabilities, have like gotten back their same jobs, or have gotten different jobs that they actually love more than their old job, it’s really inspiring. I’m like, ‘Well, that’s cool.’ ‘Cos that gives me hope that there is something out there for me to do that I might eventually like, or you know, gives me hope to go back to my same job, similar job. [SCI06]
CMO#6 - mapping out possible itineraries
For some participants, EIVR actively facilitated them to explore specific options that might work for them and their unique situation. However, because they could not start this process during rehabilitation, this type of support is typically provided by vocational providers outside of an EIVR service. For those participants who had received both EIVR and later vocational rehabilitation via another provider, they frequently referenced a lack of alignment between services in terms of communication and linkages with past explorations of vocational options. They specifically highlighted the value of focusing on self-identity narratives within EIVR, which they did not experience in later vocational services. Instead, these services typically assessed body and structure impairments or activity limitations, and then used these to determine possible vocational roles.
Participants tended to move from a CMO#5 space into this more targeted and focused space as they continued to gain clarity and as they were able to prioritize RTW goals. In this context, EIVR can support people with SCI to map out and plan RTW itineraries, constructing specific pathways and specific, actionable goals for the person to enact their RTW future. EIVR provision for participants at this stage supported the development and growth of self-efficacy, and vocational identity was sustained.
Discussion
The varying types and degree of wayfinding support required to think about, plan and action vocational aspirations mean that EIVR is provided flexibly to people with newly acquired SCI in response to three pivotal contexts: the person’s level of clarity (or not) about neurological and eventual functional status, their ability to return to the same employer in the same or similar role, and their degree of decision-making influence within their pre-SCI employment role.
Participants’ experiences suggest that developing, maintaining and enacting hope is a crucial mechanism of intervention effect within EIVR. Very early in their rehabilitation, EIVR offers people with SCI the resources to foster a sense of hope. This is achieved by supporting them to imagine a possible future while also challenging expectations and assumptions about what was possible vocationally while living with the experience of SCI. This finding is similar to previous studies in the SCI population, where hope or ‘interest in the future’ appears to enhance motivation within EIVR programmes (Hay-Smith et al., 2013; Middleton et al., 2015; O’Neill & Dyson-Hudson, 2020; Ramakrishnan et al., 2018). For those who can return to the same employer in a similar role, EIVR contributes to the maintenance of hope by either facilitating an environment allowing them to enact their pathway to RTW or providing practical support to ensure that RTW pathways are put in place with employers. For those required to imagine and plan for a new vocational future, EIVR develops and sustains hope by working with people following SCI to gather ‘specific visions’ for a future self that aligns with their past self. In some instances, it supports the enactment of hope by constructing specific pathways and actionable goals for the person to enact their RTW future.
There is a clear alignment between Snyders Hope Theory (Snyder, 2002) and participants narratives within this research. Of specific note is the important role EIVR plays providing opportunities for people with SCI to be actively involved in actions and plans to enact hope. This contrasts with general conversations about possible vocational futures, with messaging suggesting that for people with newly acquired SCI, their ability to realize their vocational aspirations is ‘out there’ somewhere in the future. Instead, EIVR appears to provide people very early in their rehabilitation the opportunity to explore pathways to enact hope, and in ways that support them to explore alignment between their pre- and post-SCI self. Bloom et al. (2020) postulate that an empowerment framework in EIVR may be useful in facilitating self-efficacy, hope and motivation to improve employment outcomes following SCI. Research also suggests that hope development is protective and promotes coping and adjustment and prevents despondency following SCI (Dorsett, 2010).
EIVR also explicitly allows the person with SCI to explore their vocational values, preferences, and aspirations. This is tied into an individual’s occupational bond or connection to the world of work (Bloom et al., 2019). The construct of occupational bond has been suggested to be helpful when considering intrinsic RTW motivations following SCI (Bloom et al., 2020). Participants experiences highlight the importance of not only exploring roles based on their previous job or their post-SCI limitations and challenges. Participants’ experiences of vocational rehabilitation services provided later in their rehabilitation suggest that their limitations and restrictions post-SCI were prioritized, rather than exploring vocational identity and work roles that might emerge from a strength-based, aspirational stance. EIVR’s explicit attention to exploring the values and preferences of the person with SCI and possibilities for environmental context adaptations that could allow them to enact vocational aspirations appeared to be a critical mechanism of intervention effect. Bloom et al. (2020) postulate this is due to the vocational consultant including interventions that improve an individual’s self-efficacy.
For participants who were interviewed later in their rehabilitation, many described the lack of momentum and alignment of approach between EIVR and other vocational rehabilitation services. This area requires further investigation since, while EIVR can set up aspirational expectations, people with SCI can feel a sense of abandonment and experience a loss of hope without timely follow-up. This finding echoes survey results from another phase of the overall research, which identified a risk of losing momentum and RTW hopefulness if there was no continuity of support beyond the acute setting (Snell et al., 2021).
Participants’ experiences suggest that for those who could self-advocate to establish a RTW plan, the presence of EIVR providers within the rehabilitation team facilitated a vocationally-focused milieu, allowing people to wayfind towards their own vocational futures (Bloom et al., 2017). However, many participants did not overtly recognize the role of EIVR in this space, feeling that they achieved RTW without any support. Nevertheless, some participants’ experiences suggest that EIVR provider persistence with casual conversations about possible vocational futures, even in the face of some reluctance, could potentially contribute to smoother RTW pathways.
This study has collected data from people who received EIVR, and often up to two years after receiving it. There is, therefore, a need to gather data closer to the point of EIVR delivery, and preferably through observing and discussing the responses of people with newly acquired SCI. Further understanding of how EIVR facilitates a vocationally-focused milieu within a rehabilitation team is needed - particularly since we want to develop an EIVR implementation plan to improve RTW outcomes for people with acquired neurological conditions other than SCI in different rehabilitation team contexts.
Participants’ experiences suggest that an inherent tension exists between flexible, casual and person-led EIVR delivery and a frequent lack of clarity about the EIVR role. This needs to be considered carefully when translating EIVR into other rehabilitation contexts and when capturing and measuring RTW outcomes as a result of EIVR.
Conclusion
We have articulated various contexts and mechanisms that appear to contribute to the successful negotiation, achievement, and sustainability of RTW outcomes for people following SCI in response to EIVR. Consistent with previous research, findings from this study provide further support to the importance of hope in optimizing RTW outcomes after SCI. However, participant narratives in this study have emphasized the important role that EIVR has in supporting people with SCI to be actively involved in actions and plans to enact hope. The importance of a vocational rehabilitation approach that explores vocational identity from a strength-based, aspirational stance has also been highlighted. These theoretical understandings can optimize RTW outcomes by refining the provision of current EIVR services, while also informing the development of EIVR interventions for people with acquired neurological conditions in other rehabilitation team contexts.
Funding
This research was supported by a grant from the NZ Health Research Council in collaboration with the Ministry of Social Development (Grant 19/834).
Footnotes
Acknowledgments
The authors would like to thank participants who gave their time and to the NZ Spinal Trust Vocational Service for their support of this research.
Conflict of interest
The authors declare they have no conflicts of interest.
Ethical declaration
The ‘Early vocational rehabilitation following neurological disability study’ project, including this qualitative study, received ethical approval from the University of Otago Human Ethics Committee (ref H19/170).
Informed consent
Written informed consent was obtained from all participants. All identifying data has been removed.