
Abstract
BACKGROUND:
In Denmark, people with permanent and significantly reduced work capacity can be assigned to a flexi-job (FJ) scheme. In 2013, the social security policy for FJ was reformed to improve employment possibilities for people with reduced work capacity.
OBJECTIVE:
To describe work participation in the FJ scheme before and after the reform in the North Denmark Region.
METHODS:
The study population was assigned to the FJ scheme between 2010 and 2015 and followed for two years. Work participation score (WPS) was defined as the number of working weeks divided by the total number of weeks in the FJ scheme. High WPS was defined as above the median.
RESULTS:
A total of 4,668 people were included in the study. High WPS was significantly influenced by enrolment after policy changes (odds ratio (OR)) 1.60, 95% CI 1.41–1.81), male sex (OR 1.20, CI 1.06–1.36), age above 50 (OR 0.72, CI 0.58–0.90), peripheral living (OR 0.75, CI 0.63–0.90), contact to both somatic and psychiatric healthcare (OR 0.55, CI 0.43–0.71) and a prior strong association to the labour market (OR 5.70, CI 4.40–7.37).
CONCLUSIONS:
Policy changes increased work participation in the FJ scheme.
Introduction
In Denmark, a flexi-job (FJ) scheme can be awarded if a person’s ability to work is permanently and significantly reduced in any profession due to health problems and/or psychosocial difficulties (The Danish Agency for Labour Market and Recruitment, 2012). The FJ scheme was introduced in Denmark in 1998 to support a more active employment policy with the overall goal of ensuring employment of people with permanently reduced work capacity. The number of people allocated to the flexi-job scheme has increased during the years; in 2018, more than 84,000 people took part in the JF scheme (Deloitte, 2018). In 2013, the Reform of the Disability Pension and Flexi-job Scheme was significantly changed in order to help more people with permanently reduced work capacity to maintain affiliation to the labour market. According to the Danish Agency for Labour Market and Recruitment (STAR.dk) the target demographic of this reform was persons with a complex set of problems, for whom social-, employment- and health-related challenges created barriers to entering the labour market, and without an interdisciplinary initiative they were at risk of ending up on a permanent disability pension. The implication was that it should be more difficult to obtain a disability pension, especially for those under the age of 40. In addition, rehabilitation teams were set up to strengthen the level of cooperation between municipalities and the regional healthcare system. The rehabilitation team has to consider different factors such as physical and mental health, level of education, previous work experience and social network before awarding the FJ scheme. By law, a health professional (usually a medical doctor) has to participate in the rehabilitation team to counsel on healthcare matters. The FJ scheme can be awarded after a period where the individual in collaboration with a social worker has made several adjustments to optimise his or her ability to work. In the FJ scheme each case is individualised and different work situations are tried out in one or several periods of internships to uncover challenges during work for each participant. Often a mentor is attached to help optimise the workday and discuss and solve work-related problems.
After being awarded the FJ scheme, the person has to seek employment like everyone else, but the job often contains a reduced number of work hours and takes into consideration the individual’s disability. Income in the FJ scheme is a combination of a salary from the employer and a supplement in the form of a flexible pay subsidy from the local authority. Regulations for payment in the FJ scheme also changed with the policy changes. After the 2013 reform, the employer only pays for the number of work hours, and the employee receives a wage subsidy. This regulation was introduced to encourage employers to engage FJ workers even for a few work hours a week.
The policy changes in 2013 were implemented to increase the number of people in the Danish workforce by including people with a low work capacity in the FJ scheme. The policy change was evaluated by the Danish Agency for Labour Market and Recruitment in 2017 and by a consultancy in 2018 (Deloitte, 2018; Styrelsen for arbejdsmarked og rekruttering, 2018). These reports concluded that more people were able to work after the policy change in 2013; however, differences in the populations being assigned to the scheme before and after the reform were not taken into consideration. In this cohort study from the North Denmark Region, we aimed to describe work participation in the FJ scheme before and after the policy change in 2013, taking into account presumed predictors of work participation such as sociodemographic factors, healthcare use and work participation before the award.
Methods
Study population
The study included individuals aged 18–65 years living in the North Denmark Region (approximately 600,000 inhabitants) who had been awarded a FJ scheme in the period between 1 January 2010 and 24 August 2015. The population was followed until they discontinued the FJ scheme either because of old age pension, disability pension, early retirement, death or end of follow-up (3 September 2017). For each individual, the follow up period was no longer than two years. In order to investigate the impact of the 2013 policy changes, the population was divided into two groups. The first group included people who had been awarded a FJ before the new reform became effective on 1 January 2013, and the second group included people who had been awarded a FJ after this date.
Register data
Data were obtained from three databases and were linked using the unique and anonymised Danish Social Security number. In Denmark every individual receiving social benefit or healthcare is registered in Danish databases. This enabled us to have a complete dataset without missing data.
Information on people receiving benefits in the FJ scheme was obtained from the DREAM Database of the Ministry of Employment, which holds data on all recipients of benefits in Denmark and is updated on a weekly basis. Public social benefits paid to the study participants five years before entering the FJ scheme were identified, and a working week was defined as week during which the person in question had received no social benefits besides study grants. The proportion of time working was the number of weeks at work divided by the total number of weeks during this five-year period; it was categorised into four groups (0–<25% of the time at work, 25% –<50% of the time at work, 50% –<75% of the time at work and 75% –100% of the time at work)
Contacts to specialised healthcare were identified from the Danish National Patient Register (NPR), which contains data on somatic inpatient visits since 1977 as well as emergency and outpatient visits and all contacts to psychiatric hospitals since 1995. Inpatient or outpatient visits to specialised health care in the two-year period before entering the FJ scheme were categorised into four groups: no visits, only somatic visits, only psychiatric visits or both types of visits.
Information on date of birth, sex, place of residence and death was obtained from the Danish Civil Registration System (DRS). Age at assignment to the FJ scheme was divided into four groups: 18–29 years, 30–39 years, 40–49 years and 50–65 years. The place of residence was grouped into peripheral, rural or urban municipalities according to the Danish Rural Development Programme from 2007–2013 (European et al., 2013).
Work participation score (WPS)
We used the WPS as an outcome measure for job retention in the FJ scheme. An individual in a FJ scheme can either be working, absent owing to illness or job seeking. The WPS was calculated as the fraction of the number of working weeks divided by the total number of weeks in the FJ scheme.
A high WPS was defined as a WPS above the median. The median was chosen as the data did not follow a normal distribution, and it was close to the average WPS for people in FJ schemes in Denmark (Styrelsen for arbejdsmarked og rekruttering, 2018).
Statistical analyses
Statistical analyses were performed using Stata SE 15 with the Kruskal-Wallis test and rank sum test as appropriate for univariate analysis, as the data did not follow the normal distribution. Baseline characteristics were compared using the Chi-square test. Logistic regression was used to estimate the association between policy changes and a high WPS. The model was adjusted for sex, age, place of residence, contacts to specialised healthcare and the proportion of time in a job in the five years before the FJ. P values below 0.05 were considered statistically significant.
Ethics
The Danish Data Protection Agency (ref. 2008-58-0028) approved the study. According to Danish law, informed consent is not required for register-based studies.
Results
In total 4,668 people received FJ benefits during the study period, the majority of whom (64%) were awarded the FJ scheme before the reform (Table 1). In general, more women were in the FJ scheme, most were above 40 years, lived in a rural area and have had contact to the somatic healthcare system in the two-year period before the award. These variables did not differ significantly before and after the policy change. However, the proportion of time in a job in the five-year period before the FJ was awarded was significantly lower among individuals assigned a FJ scheme after the reform; the proportion with a strong affiliation (above 50%) was reduced from 38% to 30%.
Baseline data for individuals assigned to the flexi-job scheme before and after the policy change in 2013
Baseline data for individuals assigned to the flexi-job scheme before and after the policy change in 2013
Figure 1 illustrates the changes in the WPS for people in the FJ scheme before and after the policy changes in 2013. Overall, the median WPS was 65% with a significant increase from 60% before the policy change to 70% after (P < 0.01). For almost all groups, the WPS was associated with a significant increase after the reform for most sociodemographic characteristics (Fig. 1). It is noteworthy that for individuals without contact to specialised health care before the award of the FJ or with contact to only psychiatric healthcare before the award of the FJ, no significant difference in work participation before and after the policy change was observed (Fig. 1).
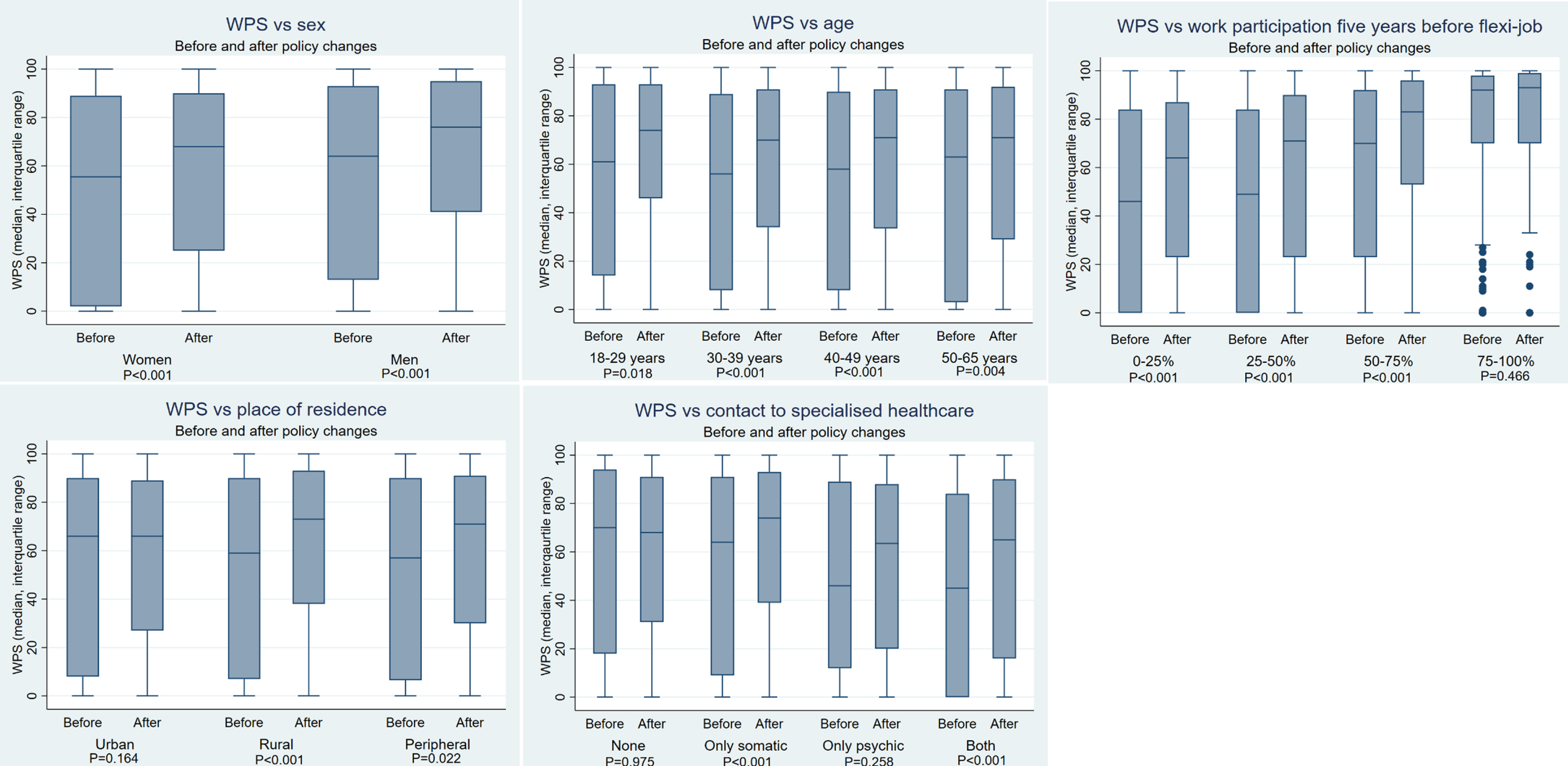
Work participation score (WPS) and its association with sociodemographic characteristics in individuals awarded a flexi-job scheme before and after policy changes in 2013.
In the logistic regression model, the policy change was associated with a high WPS; in the multivariate analysis, the impact of the policy change was even more pronounced (Table 2). However, the strongest predictor for a high WPS in the FJ scheme was strong affiliation to the labour market in the years before the FJ was awarded. Furthermore, young age and urban living were also linked to a high WPS, whereas individuals with contact to both specialised somatic and psychiatric care in the years preceding the award were less likely to have a high WPS than individuals with no contacts to specialised healthcare.
The association between policy change, sociodemographic factors, healthcare use, previous work participation and a high work participation score (WPS) in the flexi-job scheme. Proportions and odds ratios (OR)
*adjusted for the other variables in the table.
The FJ scheme was introduced in 1998 to ensure the employment of people with a permanently reduced work capacity. In 2013, the Danish government changed the FJ scheme markedly in order to help more people with permanently reduced work capacity to maintain affiliation to the labour market. The intention of the reform was to include people with very low work capacity in the FJ scheme. Before the policy change, these individuals might have been awarded disability pension. This study demonstrated that the proportion of individuals with high work participation increased after the FJ policy changes in 2013. This may be a result of the obligatory cross-disciplinary approach to the process of assigning individuals to the FJ scheme.
The study showed a strong impact of policy change after adjustment for sociodemographic factors, healthcare use and prior work participation. It also demonstrated that several factors seemed to have an impact on job retention in the FJ scheme. The most powerful factor was strong affiliation to the labour market in the years before being awarded the FJ. This indicates that the time during case management towards being awarded a FJ scheme should be as short as possible, because the chances of success in a FJ seem to be larger with previously strong affiliation to the labour market. Furthermore, work participation after assignment to the scheme may also be important as described in an earlier study (Jensen et al., 2014,). That study showed that almost a quarter of individuals assigned to the FJ scheme never entered the labour market if they received unemployment benefits for more than three months after the award. This emphasises the need for individual case management to ensure employment as soon as the FJ scheme is awarded.
The amount of research on return to work for various patient groups has increased considerably over the years. Recent reviews have revealed the importance of age, sex, sociodemographic factors, comorbidity and previous sick leave on return to work for conditions and diseases such as mental disorders, low-back pain and cancer (de Vries et al., 2018; Kiasuwa Mbengi et al., 2016; Steenstra et al., 2017). The present study demonstrates that the same factors influence work participation in a FJ scheme, even though a job in the FJ scheme is designed to take the individual’s disabilities into consideration.
Individuals being awarded a FJ scheme after the policy change in 2013 seem to include a more vulnerable group of people, as it became possible to gain a job with very few work hours. Despite that, the WPS increased after 2013. This success may partly be due to a change in the wage subsidy that encourages employers to hire for only a few hours a week. Another significant change after 2013 was the introduction of more systematic case management for each individual on long-term sick leave and a cross-disciplinary approach that includes municipal, medical and social expertise. In the FJ scheme each case is individualised and therefore, case management might affect work participation by providing a more precise description of the individual’s needs for obtaining employment. A Cochrane review from 2017 indicates that standardised return-to-work coordination programmes have no benefit (Vogel et al., 2017); on the other hand, our results show that an individual approach could have significantly increased the WPS for a population with very low work capacity.
Complicated health-related problems such as physical and psychiatric diagnoses that require specialised medical treatment have a negative impact on the WPS in the FJ scheme. One explanation for this could be that it is difficult to find a job that considers physical and psychological needs during the workday. This is supported by a Swedish study which found that individuals with long-term sick leave often have psychiatric–somatic comorbidity and that a majority of these individuals need medical rehabilitation to return to work (Linder et al., 2009). The policy change in 2013 did not succeed in increasing work participation among psychiatric patients, despite the cross-disciplinary approach.
Strengths and weaknesses
A strength of this study is its register-based design with complete follow up. The DREAM database is updated on a weekly basis, and thus provides detailed information on the study population. Denmark is known for its unique identification number for each inhabitant, which can be linked to services such as healthcare and social benefits (Frank, 2000). The databases are considered valid for research purposes (Andersen et al., 2011; Hjollund et al., 2007; Schmidt et al., 2015). However, information about the precise number of work hours is not registered in the databases. Information about the number of work hours could have added valuable information on the impact of the policy change. We were unable to investigate the association between educational level and WPS. However, we may reasonably assume that the level of education has not changed in individuals awarded a FJ before and after the policy change in 2013. During the study period, the overall unemployment rate in the Danish population varied, with the highest proportions in the beginning of the study period (OECD Data, n.d.). The need for labour may have influenced the number of available FJs in Denmark during the study period.
Conclusion
The policy change in 2013 with an introduction of an obligatory cross-disciplinary approach to individuals with low work capacity increased work participation among individuals in the FJ scheme. Still, the strongest predictor for high work participation was prior affiliation to the labour market, indicating the need for short case management periods towards a FJ. This means that an individual approach and fast case management could be key elements in the process of helping people with reduced work capacity back to work.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Author contributions
All authors contributed to the study’s conception and design. Material preparation, data collection and analysis were performed by Nanna Weye, Kirsten Fonager and Ditte Munkedal. The first draft of the manuscript was written by Ditte Munkedal and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Conflict of interest
The authors have no conflict of interest.
Ethical approval
The Danish Data Protection Agency (ref. 2008-58-0028) approved the study.
Funding
None to report.
Informed consent
According to Danish law, informed consent is not required for register-based studies.