
Abstract
BACKGROUND:
Rates of stroke in people of working age are increasing. Returning to work (RTW) after stroke is a key rehabilitation aspiration for younger stroke survivors. A pilot community-based Stay at Work Initiative (SAWI) was developed and delivered from March 2017 to December 2019. SAWI used a co-ordination based approach, covering rehabilitation and vocational recovery to support RTW in younger stroke survivors.
OBJECTIVE:
The aim of the study was to conduct a feasibility evaluation of SAWI.
METHODS:
A mixed methods approach was taken considering quantitative and qualitative data. Quantitative data included employment, mood, anxiety and fatigue outcomes at time of engagement with the service and at 6-months post-stroke. Qualitative data was collected on a sub-sample of SAWI clients who volunteered to participate in a semi-structured interview.
RESULTS:
Overall, there were 93 referrals to SAWI, with 42 clients completing an initial service meeting. Average working hours pre-stroke were high (mean 46.9, SD 22.0, range 5–100 hours/week). By 6 months post stroke, 71% (n = 29 of 41) of SAWI clients were working. For those with 6-month questionnaire information (n = 19), there was a significant reduction in cognitive fatigue, overall fatigue levels, and perceived impact of stroke on employment (medium effect sizes of r = 0.36, 0.34 and 0.40 respectively). No significant difference was seen on measures of mood or anxiety from pre- to post-intervention. Qualitative interviews with six SAWI participants highlighted the importance of personalised support that addresses individual needs during the RTW journey.
CONCLUSIONS:
A significant number of eligible participants referred to SAWI can engage with the service. RTW is able to be assessed as are potential predictor variables. Seventy one percent of participants had RTW at 6 months post-stroke. Mood, self-efficacy, adjustment, and fatigue likely impact RTW. Qualitative interviews identified that SAWI’s personalised support, tailored to individual need, was valued.
Introduction
Returning to work is an essential rehabilitation outcome for many young stroke survivors. Alongside the apparent impact on the individual’s financial security (Vestling et al., 2005, 2013), the consequences of being unable to return to work have also been described in terms of its effect on overall health and wellbeing, including an impact on mood (Vestling et al., 2013; Walker, 2008), the loss of self-identity and purpose (Johansson & Tham, 2006; Shipley et al., 2018; Vestling et al., 2013), and physical deterioration (Walker, 2008). Further, there can be a loss of social connection and feelings of isolation and boredom (Shipley et al., 2018; Vestling et al., 2005, 2013). It is therefore not surprising that studies have identified return to work as an important predictor of increased life satisfaction following stroke (Passier et al., 2011; Vestling et al., 2003).
Despite the value of resuming work for young stroke survivors, evidence suggests that more than half of working aged adults will not return to work following their stroke (Daniel et al., 2009; Duff et al., 2014; Glozier et al., 2008; Vestling et al., 2003; Walsh et al., 2015). Moreover, of those who do return to work, many experience a considerable reduction in working hours (Duff et al., 2014; Passier et al., 2011; Vestling et al., 2003). In hopes of improving this outcome, a plethora of research has been conducted identifying the barriers and facilitators to return to work. This research has led to recommendations that return to work interventions should target neurological deficits, reduced ambulation and participation in activities of daily living, cognitive and behavioural impairments (Treger et al., 2007; Vestling et al., 2003; Wei et al., 2016), fatigue (Andersen et al., 2012; Wei et al., 2016), psychiatric morbidity (Glozier et al., 2008), poor social support (Walsh et al., 2015), negative experiences with work rehabilitation agencies, a lack of workplace support, and an unaccommodating physical workplace environment (Fadyl et al., 2010). Despite these recommendations, the evidence to recommend particular return to work interventions for those with stroke is limited, with a systematic review identifying only one randomised control trial (Wei et al., 2016).
Effective return to work interventions have been increasingly explored and cited within the traumatic brain injury (TBI) population. TBI is damage to the brain occurring from an outside force (e.g. the head being struck) (Menon et al., 2010), and this population is in many respects similar to those with stroke, with some studies including both TBI and non-traumatic brain injury, such as stroke, as an overall ‘acquired brain injury’ group (e.g. (van Velzen et al., 2016)). A review of interventions for people with TBI denoted three categories of programs: program-based vocational rehabilitation, supported employment, and case coordination (Fadyl & McPherson, 2009). Of these interventions, case coordination had the strongest evidence for better employment and productivity outcomes. As an example, Radford and colleagues (Radford et al., 2013) evaluated outcomes in TBI patients who engaged with a case manager to assess their needs, educate them as to the effects of TBI on work and strategies to manage these, as well as liaise with employers and assist in pre-work and community integration retraining. This resulted in greater return to work compared to those who underwent usual care. Similarly, a small randomized controlled trial found increased return to work rates for TBI participants following participation in a ‘resource facilitation model’, whereby facilitators help identify person-centered goals and enable access to resources that provide education and support (Trexler et al., 2016).
As little research has focused on developing a community based, case coordination return to work program specifically for working aged stroke survivors, the aim of the present study was to conduct a preliminary investigation to evaluate the feasibility and acceptability of such a program, the Stay at Work Initiative (SAWI). Qualitative research of young stroke survivors within Australia suggested the need for more age relevant information, including on return to work alongside further guidance from professionals (Shipley et al., 2019). SAWI aimed to provide stroke survivors with a coordinator early within their recovery journey to ensure coordinated care. The coordinator assessed for facilitators and barriers to return to work, followed by supporting access to services, information, and resources, assistance with problem solving, liaison with the workplace and employer, and provision of ongoing support throughout the recovery process.
The objective of this study was to conduct a feasibility evaluation of the SAWI program. Specifically: The feasibility of recruiting participants. The ability of participants to complete the SAWI intervention. The rate of return to work and the characteristics of those who did and did not return to work; as well as changes in work role and hours, adjustment, mood, anxiety, fatigue, and self-efficacy from engagement in the program. Establish acceptability of SAWI via a qualitative evaluation of a sub-group of participants’ experience of the service.
Methods
Study design
Development and delivery of the SAWI service was led by the Stroke Association of Victoria (SAV). SAV is a community-based support organisation for people who have had a stroke. SAV worked in collaboration with Barwon Health (the public health service covering Geelong and surrounds in Victoria, Australia), and Deakin University. The feasibility trial was conducted from March 2017 through December 2019. Quantitative data was taken from referral and service data collected during the course of the intervention. A qualitative evaluation was conducted on a sub-group of volunteering clients, using a semi-structured interview. As quantitative data was collected as part of usual clinical care, the analysis and publication of this was covered by an Ethics Exemption granted by Barwon Health HREC (17/74). The qualitative sub-study received full ethical approval by Barwon Health HREC (18/225).
Participants
Quantitative evaluation
Individuals included in the quantitative evaluation were all those referred to SAWI by Barwon Health. Some service referral criteria changed within the first three months of the pilot delivery to ensure all stroke survivors who may benefit from the service were identified and referred. These included: definition of employment (people in volunteer roles and at home caring roles were included), age (increased from 65 to 75 to be more in line with the increasing retirement age in Australia and be inclusive of those who choose to work beyond retirement age) and time since stroke (originally 6 weeks, increased to 3 months to allow greater time for recovery, referral, and engagement). To be included in the analysis, clients needed to be aged 18 to 75 at point of referral, working prior to the stroke (one or more hours per week for pay or in a family business), and be discharged home from hospital (acute or rehabilitation).
Qualitative evaluation
To be eligible for participation in the qualitative component of this research project, participants had to be past or present SAWI clients who responded to an invitation to participate and were able to (a) provide informed consent and (b) read the research information. If required, a support person could also read the research information to them.
Intervention description
SAWI was a case coordination approach, where a RTW coordinator was assigned to the client. The RTW coordinator (“SAWI Coordinator”) was a Stroke Association of Victoria staff member, who had university qualifications. Two coordinators were in the role over the duration of the project; the first had a rehabilitation counselling degree, the second had a teaching degree with experience working in management, disability, and employment sectors.
After referral, the client was invited to an initial face-to-face meeting with the SAWI Coordinator. During this meeting, the coordinator gathered information about the client’s current health, financial, and employment situation, including utilising validated measures including the Patient Health Questionnaire-9 (Kroenke et al., 2001) and GAD-7 (Spitzer et al., 2006) for depression and anxiety; the Neurological Fatigue Index –Stroke for fatigue (Mills et al., 2012), the Work and Social Adjustment Scale (Mundt et al., 2002), and the General Self Efficacy scale (Schwarzer & Jerusalem, 1995). In addition, barriers and facilitator to return to work were identified as well as financial commitments, social supports, and mental health supports. Details on current health providers and the employing organisation were also collected.
Following the initial meeting, the coordinator and client discussed gaps in care, potential referral options and a plan of action for follow-up. Subsequent meetings were either face-to-face or via telephone. The coordinator liaised with relevant stakeholders as required (e.g. GP, rehabilitation teams, employer), or encouraged the client to facilitate a referral through their GP as needed (e.g. for further rehabilitation or a mental health plan). Written resources were sent to the client as needed via post or email. Assistance was provided with navigating services and filling out paperwork (e.g. Centrelink (Social Security)/ income protection insurance applications), creating CVs, and identifying training opportunities if required. If indicated and appropriate the coordinator met with the employer and client to discuss keeping the job open during the recovery period as well as with respect to any required job adjustments or a graduated return to work plan. In addition, some clients were referred by the coordinator to the team psychologist (AT) for an initial assessment to determine need for further intervention if mood was flagged as an issue. Brief group programs, each including two group sessions covering recovery, adjustment, navigating services, and career options, were offered as sufficiently sized groups of interested SAWI clients occurred. Intervention duration was up to 12 months, and ended when no further support was indicated or the client did not want further support.
Measures
The SAWI Coordinator trialled the following validated measures to help identify potential issues that may become barriers to return to work. These were used during the initial interview and readministered at later time points (including a 6-month post-stroke check in interview) if the person was still engaged with the service. Other data (e.g. return to work status) was taken from initial interview and clinical notes up until the 6-month time point.
Vocational outcomes
Work status was taken from clinical notes and defined as having engaged in paid employment (or working within a family business) for one or more hours per week at the point of the most recent contact, or at the 6-month post-stroke point for those engaged with the service at that time. If people were still on paid or unpaid leave from their employer and had not engaged in work activities since their stroke they were not defined as working.
Job title, time spent at employer, number of hours worked per week, and job status (full time/part time/casual) were self-reported. Role change was explored by the question “If you are currently working, has your role changed?” with an additional open-ended response option to describe the role change.
Mood and anxiety
Depression severity was evaluated with the Patient Health Questionnaire-9 (PHQ-9) (Kroenke et al., 2001). The PHQ-9 is a self-report instrument that is comprised of nine items, which cover depressive symptoms experienced during the last two weeks. Each item is rated on a scale ranging from “0” (not at all) to “3” (nearly every day). PHQ-9 total scores can range from 0 to 27 with higher scores indicating greater depression severity. Scores of five, ten, 15, and 20 are considered to indicate mild, moderate, moderately severe, and severe depression. Internal consistency in the current study was good (Cronbach’s α baseline = 0.775; follow-up = 0.829).
Anxiety severity was assessed with the General Anxiety Disorder-7 (GAD-7) (Spitzer et al., 2006). The GAD-7 is a 7-item self-report instrument that assesses anxiety symptoms experienced over the past two weeks. All items are rated on a scale ranging from “0” (not at all) to “3” (nearly every day). GAD-7 total scores can range from 0 to 21. Higher scores indicate greater anxiety severity: scores of five, ten, and 15 are considered to indicate mild, moderate, and severe anxiety. Internal consistency in the current study was good (Cronbach’s α baseline = 0.878; follow-up = 0.853).
Fatigue
Fatigue was evaluated with the Neurological Fatigue Index –Stroke (NFI-Stroke) (Mills et al., 2012). The NFI-Stroke is comprised of a 10-item summary scale as well as physical (eight items) and cognitive (four items) subscales. Each item is rated on a scale ranging from “0” (strongly disagree) to “3” (strongly agree) with higher scores suggesting greater severity of fatigue. Internal consistency in the current study was high (Cronbach’s α baseline = 0.932; follow-up = 0.915).
Self-efficacy
Self-efficacy was assessed with the General Self-Efficacy Scale (GSE) (Schwarzer & Jerusalem, 1995). The GSE is a self-report instrument that consists of 10 items, which are rated on a scale ranging from “1” (not at all true) to “4” (exactly true). GSE total scores can range from 10 to 40; a higher score indicates greater self-efficacy. Internal consistency in the current study was high (Cronbach’s α baseline = 0.928; follow-up = 0.921).
Impairments in work and social adjustment
Work and social adjustment was evaluated with the Work and Social Adjustment Scale (WSAS) (Mundt et al., 2002). The WSAS is a self-report instrument that is comprised of five items, each measuring impairment in one functioning domain: employment, home management, social leisure activities, private leisure activities, and close relationships. The items on the WSAS are rated on a scale ranging from “0” (not at all) to “8” (very severely). WSAS total scores can range from 0 to 40. Higher scores indicating greater functioning impairment: scores of ten and 20 are considered to indicate moderate and severe impairment. Internal consistency in the current study was good (Cronbach’s α baseline = 0.867; follow-up = 0.882).
Qualitative interview
To allow for the detailed exploration of participants’ experiences with SAWI, qualitative interviews consisting primarily of open-ended questions were conducted via telephone. The interviews took between 30 and 50 minutes and were semi-structured, loosely guided by an interview schedule. All conversations were audio-recorded and then transcribed verbatim. Names were replaced by a pseudonym. The transcripts were sent to the participants for review, ensuring correct representation of their experiences. The member of the research team who conducted the qualitative interviews had no direct involvement with SAWI, enabling the participants to speak openly about their experiences with the program.
Statistical analysis
Data was extracted from clinical notes into an Excel file. Intervention length varied depending on client need (any time up to 12 months) post stroke over the course of the service pilot; however, very few clients were seen past the 6-month time point. Available data was included; this includes return to work status derived from clinical notes for all engaged clients; and additional data (including validated scale measures) for those who were still engaged at 6 months post stroke and completed a check in interview at that timepoint. In some cases, validated measures had 0.5 options selected, in these cases the score was rounded up to the next full number. Data analysis was conducted using IBM SPSS Statistics © Version 26. Self-reported job title was categorised according to the Australian and New Zealand Standard Classification of Occupations (ANZSCO) (Australian Bureau of Statistics, 2019). ANSZCO skill levels are rated by level of education, training and experience required to perform the role, with Skill Level 1 being the highest skill level (Bachelors degree or higher/ 5 years of experience or more) through to Skill Level 5. Due to small samples sizes and non-normal data distribution, change over time for continuous data was tested using the Wilcoxon Signed Rank Test, and group differences were examined using the Mann-Whitney U Test. Effect size for change over time were calculated using Wilcoxon Z via r = Z/ (√N), where N = number of observations (i.e. cases x 2) (Pallant, 2011); and effect size is defined as a small effect = 0.1, medium effect =0.3 and a large effect = 0.5 as per (Cohen, 1988). Significance was set at p < 0.05.
Qualitative analysis
Interpretative Phenomenological Analysis (IPA) was used to explore the interview data. The first step of the analysis process involved reading the transcripts multiple times to facilitate immersion in the data, as per IPA guidelines (Smith et al., 2009). Subsequently, each transcript was assigned with exploratory and interpretive comments. The codes that resulted from this initial analysis were converted into emergent themes. Conceptually similar themes were then collated and assigned a descriptive label. Following this process, interrelations between themes across all transcripts were identified and key themes developed. To increase rigour of the analysis process, the themes that were derived from the IPA were validated by a Provisional Psychologist with expertise in qualitative research.
Results
Quantitative outcomes
Recruitment, retention, questionnaire completion and participation
As shown in Fig. 1, during the course of the project, 333 stroke survivors aged 23–75 [mean (SD) = 61.4 (10.6)] years were identified from hospital lists (n = 214 (64.3%) male). Of those a total of 93 referrals (27.9%) were made to the service; while 214 (64.3%) were ineligible and 26 (7.8%) not interested. Of the 93 referrals sent to the service from Barwon Health, 92 were processed. Of those 92 referrals, 46.7% (n = 43) were engaged in the service, 18.5% (n = 17) could not be contacted, 30.4% (n = 28) declined (of those n = 15 returned to work, while n = 4 decided to retire), 3.3% (n = 3) were ineligible, and one died. A further two were excluded from the analysis, as they did not meet minimum employment criteria, leaving a total sample of 41 participants for further analysis. Of the total sample, 20 (49%) completed the validated questionnaires during a 6-month check-in assessment with the RTW coordinator. Three group programs (each with two sessions) were completed over 2017–2018, with 11 participants in total attending at least one group session (3–5 participants per program).
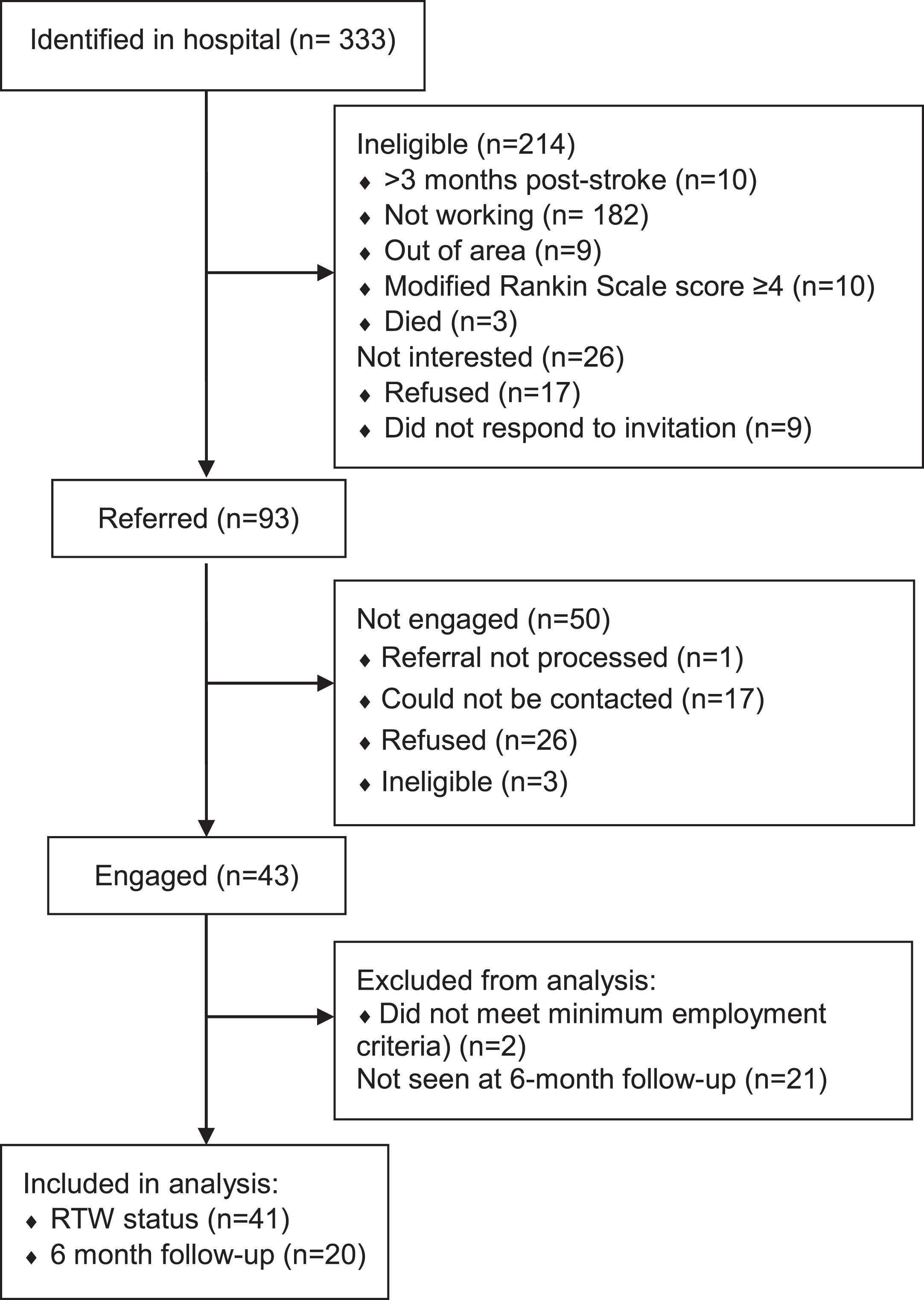
Participant flow.
An audit of clinical notes of 13 active participants found that the number of sessions per participants ranged from 4 to 21 (median 7, IQR 5–17), including contact via phone, face-to-face, email and/or postage. All participants had at least 3 phone contacts (median 5, range 3–15). Eleven participants also had face-to-face sessions (median 2, range 1–6). Stakeholders were also engaged for some participants via telephone and/or face-to-face. Specifically, for 9 participants the coordinator had contact with partners/family, while for 8 participants there was contact with other stakeholders including employers, health care providers, job skills centres and employment agencies.
Demographic characteristics of the client group whose data underwent analysis can be seen in Table 1. Almost two-thirds of the group were male, with an average age of 55 years. Most had partners, while just under one-third had dependent children at home. Only 15% reported having income protection insurance when asked at baseline. Just under one-third were self-employed, while the average time with their employer was 11 years. Rates of people employed at each ANZSCO job skill level declined as the skill level required to perform the job increased. Pre-stroke, the average hours of work were 47 hours/week, and the majority of clients had worked full-time.
Participant characteristics of SAWI clients
Participant characteristics of SAWI clients
ANZSCO: Australian and New Zealand Standard Classification of Occupations. PHQ-9: Patient Health Questionnaire-9. WSAS: Work and Social Adjustment Scale.
With regard to well-being at baseline, average mood and anxiety levels were in the mild severity level. For functioning, average levels of impairment in all five domains were also mild. There were no statistical differences in baseline demographic, employment, or wellbeing measures between those who did and did not attend the 6-month follow-up
Clinical notes review indicated that, by 6 months, 29 of the 41 (71%) clients had returned to paid work in some capacity. Of those who did not RTW (n = 12), reasons noted included: medical reasons (including sick leave, total and permanent disability, ongoing medical complications; n = 5, 42%); plans to RTW outside window (e.g. waiting for licence; retraining; n = 4, 33%), retired (n = 1, 8%), or unknown (n = 2, 17%).
Further vocational details were available for clients who attended a 6-month check-in assessment with the RTW coordinator (n = 20). For those who did not RTW who completed a 6-month check-in (n = 8), five (63%) had income protection insurance activated.
Job status pre- and post-stroke was compared. For those working casually pre-stroke (n = 3), two returned to casual work, and one was unemployed at 6 months. One person was working part-time pre-stroke and returned to part-time work. For those working full-time pre-stroke (n = 16), four (25%) returned to full-time work, five (32%) returned to part-time work, one (6%) returned to casual work, and six (37.5%) had not yet RTW by 6 months. Of 12 clients who had RTW and had 6 month follow up data available, nine (75%) reported that their role had changed at work; ranging from reduced hours and tasks modifications (e.g. reduced participation in more strenuous tasks) through to more significant position changes (e.g. ongoing restrictions to driving necessitating position change within the organisation). For working clients, the average number of hours worked per week at follow-up was 30.3 (SD = 15.2) compared with 47.8 (SD = 21.4) hours, which was a significant decline from pre-stroke (Z(12) = –2.99, p = 0.003).
Baseline demographic and wellbeing characteristics for those who did and did not RTW by 6 months
Differences in baseline data between those who did and did not RTW by 6 months can be seen in Table 2. No statistically significant differences were observed for age or selected work variables; however, the baseline levels of symptoms of depression and fatigue were higher, and self-efficacy and overall work and social adjustment lower, in those who did not RTW compared to those who did RTW.
Baseline characteristics of those who did and did not RTW by 6 months
Baseline characteristics of those who did and did not RTW by 6 months
ANZSCO: Australian and New Zealand Standard Classification of Occupations. PHQ-9: Patient Health Questionnaire-9. * Mann-Whitney U Z score.
Change in mood and wellbeing scores from the first assessment to the 6-month check-in are illustrated in Table 3. Measures of physical fatigue and overall fatigue, and perceptions of impact of the stroke on employment, significantly improved over time. Other measures of mood and wellbeing showed numerical but not statistical improvement from baseline to 6 months.
Change in mood and wellbeing data from initial meeting through to 6 months post-stroke
Change in mood and wellbeing data from initial meeting through to 6 months post-stroke
aWilcoxon Signed Ranks Test Z; bZ/√N where N = cases x 2. PHQ-9: Patient Health Questionnaire-9. WSAS: Work and Social Adjustment Scale.
A total of 41 eligible SAWI clients were approached. Six accepted the invitation to participate. The participants’ demographic information is detailed in Table 4.
Qualitative study participants’ demographic information
Qualitative study participants’ demographic information
Abbreviations: RTW, Return to Work.
Superordinate theme and key themes
The key theme Impact of Stroke summarises participants’ experiences of the sequelae of their strokes. Participants described changes in capabilities and confidence which ultimately impacted their ability to RTW. For instance, Adam [not his real name] stated that his difficulties with balance and coordination initially hindered his attempts to RTW: “And if you’re a bit wobbly, or a bit shaky on it, well it’s not going to be good, be good for a painter”. Similarly, Jason explained that his speech difficulties due to stroke led to a loss of self-confidence which impacted his RTW journey: “And yeah, just not to be able to form words properly and so forth, and to lose that confidence in myself that I couldn’t go out and do what I did before”. The theme Impact of Stroke highlights the substantial need for support after stroke and SAWI’s potential value in providing personalised care during the RTW process.
Theme 2: Support vs Personal Need
The key theme Support vs Personal Need summarises participants’ experiences of the support provided by SAWI. Generally speaking, the participants experienced the program as helpful and felt that the support they received assisted their recovery from stroke as well as their RTW process. However, participants also indicated that the support had to align with their personal needs to be beneficial. For example, Bill described SAWI not appropriately addressing his need to alleviate the financial stress he experienced as negative: “No work at all, and I wasn’t helped with the financial stress, or social support”. In contrast, meeting her personal needs, Louise identified the benefits of talking to the SAWI co-ordinator: “So, yeah, so that first initial phone call with (SAWI co-ordinator), a lot of it was (SAWI co-ordinator) how do I do this, and how do I do this, and how do I get this form, and she was able to help me with all that, so that was fantastic”. The theme Support vs Personal Need highlights the value of personalised support that is tailored to address people’s individual needs.
Theme 3: Validation
The key theme Validation summarises the impact of validation on participants’ recovery from stroke and RTW. Participants found that validating interactions with the SAWI co-ordinator assisted their overall recovery, and their RTW journey in particular. For instance, Jason described how positive feedback from the SAWI co-ordinator that acknowledged his improvement boosted his confidence during the RTW process: “Oh it’s good, it gives me the self-confidence to go out there and knock on doors again and have a renewed belief in myself”. Louise contrasted the validation she received from the SAWI co-ordinator with the invalidating interactions with friends: “But when I spoke to (SAWI co-ordinator), she talked to me and she knew exactly what was going on, and she could also sort of help me accept things that were going on, instead of my friends going oh you know, do this or do that, (SAWI co-ordinator) would be like no these things are just going to take time”. The theme Validation highlights the positive impact of validation provided by SAWI on participants’ stroke recovery.
Personal Effort
The key theme Personal Effort summarises how personal effort was required to facilitate the participants’ recovery and RTW process. For example, Richard said: “Yeah well, there’s only one way to go with a stroke, you sit around and don’t improve, or you can have a go at it, you know”. Participants also described how their self-motivation and determination to improve shaped their engagement with SAWI. For instance, Jason explained that engaging with SAWI required some personal effort; however, that effort resulted in a positive outcome: “I was a bit reluctant at first when I was contacted, but um you know, I got over, went and did it, and it’s been rewarding”. Richard similarly identified that SAWI required a level of personal effort: “Its effort to be there, and the effort to do the work on the day”. The theme Personal Effort highlights how participants’ motivation to improve not only facilitates their recovery but also their engagement with support services.
Time
The key theme Time summarises how being able to access support from SAWI throughout the RTW journey (i.e., across time) was particularly beneficial. For instance, Graeme explained: “So she was involved with my journey with that, and that was three months that I had to go through, and there were a lot of issues and stuff with that, so being positive and that positive support, and she would always call me and you know, give me a call back, and yeah”. Importantly, the participants also indicated that their need for the support provided by the SAWI co-ordinator changed over the course of their RTW process. Louise stated: “Well, um, you know, I think (SAWI co-ordinator) and I are probably just going to slow down the conversations, probably just down to monthly now, just because I am going alright and getting the hang of it all”. The theme Time reiterates the significance of the support provided by SAWI addressing the specific but changing needs of each participant.
Discussion
Around half of those referred to SAWI engaged with the service. Some (20%) of these were available for the 6-month follow-up, though clinical notes allowed assessment of RTW outcomes for all enrolled. Seventy one percent of the 41 persons engaged by SAWI had returned to work at 6 months. For the subgroup seen for a 6-month check-in, it was found that over time, levels of fatigue and work adjustment significantly improved. Those who did not RTW had lower baseline mood, self-efficacy, and adjustment scores than those who did RTW, while fatigue ratings were higher. Qualitative interviews highlighted that participants valued personalised support addressing individual needs during RTW. This included meeting the client’s personal needs, providing accessible support, considering changing needs over time, and providing validation (e.g. recognising improvements). In addition, clients identified that self-motivation and determination are important but can be a challenge in the face of the stroke sequelae. Overall, the findings support that it is possible to recruit and engage a significant number of eligible participants in a case coordination RTW service following stroke; employment outcomes can be ascertained for these individuals and they are able to complete relevant measures,; and overall clients value the service.
The 71% RTW rate is somewhat better than the 50% usually reported (Daniel et al., 2009; Duff et al., 2014; Glozier et al., 2008; Vestling et al., 2003; Walsh et al., 2015), and the overall findings of a systematic review of international studies (41% at 0–6 months and 53% at 1 year; (Edwards, Kapoor, Linkewich, & Swartz, 2018). However higher RTW rates were seen in an Australian study, which reported a RTW of 75% at 12 months, with most of those resuming employment within the first 2–3 months post-stroke (Hackett et al., 2012). It is difficult, however, to compare to observational studies of the larger stroke population given our data is from those interested in and able to engage with a RTW support service. An effectiveness trial would be required to sufficiently determine whether community-based support services such as SAWI lead to increases in RTW rates over those receiving usual care alone.
Of the participants who did not RTW, almost two-thirds had activated their income protection. As a group, they had elevated levels of fatigue and depression symptoms and lower self-efficacy and adjustment scores at baseline. This indicates that these factors likely impact RTW and could be investigated as potential predictors of a challenging RTW journey. However, these finding should be interpreted with caution, given sample size and study design. Indeed, in an Australian observational study mood was not found to be a predictor of RTW overall (Hackett et al., 2012). It may be that there are differences in the characteristics of those who do and do not engage with RTW support that is offered in addition to usual care.
Even upon returning to work, many participants in SAWI did so in altered circumstances. Consistent with findings from other studies, they did so at a significantly reduced number of hours (Duff et al., 2014; Passier et al., 2011; Vestling et al., 2003), and more often with changed roles and/or responsibilities (Radford et al., 2020). This could potentially have positive or negative effects on wellbeing. For example, decreased hours may result in decreased work stress, or conversely increased distress from, for example, reduced financial capacity or insufficient time to do the job at the expected level. We found no significant changes in mood, anxiety, or self-efficacy over time; however, some aspects of fatigue, and employment adjustment did improve. Once again, these findings need to be interpreted with caution given small sample size, follow-up rates and lack of a comparison group.
The qualitative sub-study was able to elicit the experiences of clients receiving the service. Findings highlight the importance to clients that care is directed to meet their perceived needs, and if that is achieved it is seen to positively facilitate positive RTW. This is consistent with previous findings for such interventions (Andersen et al., 2017). Conversely, if support provided did not meet participants’ needs, for example due to staffing and time limitation, this is seen to impede RTW. It was identified by participants that it is important to be able to access RTW support and resources over time during the RTW process, supporting previous findings indicating that long term follow-up of RTW clients, and capacity for long term support and access to services is important (Brannigan et al., 2017; Edwards et al., 2018). Qualitative results also expanded upon quantitative findings, with participants who described more pervasive physical and cognitive impairments after stroke identifying greater impediments to RTW (Wei et al., 2016).
Study limitations
As indicated above, there are a number of limitations to the current evaluation. The sample size was small, follow-up rates low, and no comparison group was included. Additional variables that would be likely predictors of RTW, such as disability and cognition, were not collected as service data, but examined via observation and discussion of work barriers and facilitators rather than objective tools administered by trained clinicians. Given the intervention was a new pilot, it is possible what was provided by the coordinator changed over time as experience developed and/or the coordinator changed. This is less a concern given all individuals received tailored interventions. The qualitative evaluation included only six participants (14% of those invited) which may have limited the experiences described, however, inclusion of the qualitative component allowed us to elicit in-depth information of significant clinical relevance.
Implications for research
Given these initial positive findings combined with emerging evidence in both the TBI and stroke literature supporting the case coordination approach (Donker-Cools et al., 2016; Fadyl & McPherson, 2009; Sinclair et al., 2014; Wei et al., 2016), a well-designed full-scale evaluation of a service such as SAWI is warranted. Design considerations should include factors such as the definition of RTW (as the primary outcome), and selection of appropriate secondary outcomes, potential mediator/moderators, and process outcomes and measurement (quality of life, cognition, disability, and treatment fidelity, in addition to mood, anxiety, fatigue and self-efficacy as measured in SAWI). A standardised definition of employment should be utilised to allow comparison with other studies; as to this has been major limitation to generalisability to date (Edwards et al., 2018). Consumer input should be sought regarding important outcomes and potential mediators of treatment outcomes from the lived experience viewpoint. Outcomes’ measurement conducted via telephone by assessors blinded to allocation would both ensure reduced risk of bias and increased follow-up rates (Nota et al., 2014). Assessment of all participants at regular time points, regardless of service engagement, needs to occur. RTW usual care in Australia varies across services and regions and remains ill-defined (Killey et al., 2014); as such the intervention would need to be evaluated across a wide range of services and within metropolitan, regional, rural, and remote regions. A concurrent process evaluation and health economic evaluation should be included to inform future translation and implementation. Qualitative interviews with health professionals (referrers and other stakeholders) and quantitative measures of client satisfaction and therapeutic alliance would complement and expand on the qualitative subgroup findings. With regard to the intervention, alternative modes of delivery should be considered when face-to-face sessions are not possible due to time or distance.
Of note, the SAWI pilot was completed at the end of 2019, prior to the COVID-19 pandemic. Future research and service development will need to consider the impact of this pandemic. Significant job losses occurred in Australia and elsewhere, with greater psychological distress and poorer mental and physical health evident in those who lost their job or had work reductions, than those whose work did not change (Griffiths et al., 2021). Given stroke survivors are already at higher risk of psychological distress and job instability, they may be disproportionately affected and these additional stressors and needs should be addressed. In addition, those whose work requires ongoing face-to-face contact may perceive even greater risk in return to work given the potential consequences of a COVID-19 infection while recovering from stroke. With regard to treatment, the increased emphasis on telehealth due to the pandemic (Garfan et al., 2021) means that clients are becoming more familiar and comfortable with the technology involved, and service access may increase for those in more remote areas. However, for those stroke survivors who are less comfortable or familiar with these approaches, support and advocacy may be required to ensure they do not avoid or miss out on needed support. Finally, the rise of teleworking for those who could work from home can be both a benefit and a barrier. For many, home situations may make it challenging to work and maintain motivation and energy (Pulido-Martos et al., 2021), particularly if multiple roles are expected to be completed simultaneously, such as childcare. For others, flexible work arrangements at home (for example, work hours that allow for sufficient breaks) may be beneficial for graded return to work, and management of fatigue, cognitive load, and stress. All these issues need to be considered in future RTW support planning.
Conclusions
Overall, the findings of this study indicate that a community based RTW support service can be delivered, providing personalised and person-centred support. RTW rates from such an intervention are promising, and should be further examined in a larger study with a comparison group. Results also reinforce the importance of addressing ‘invisible’ barriers to RTW, including mood and fatigue, and supporting adjustment to stroke.
Footnotes
Acknowledgments
The authors wish to acknowledge the Stroke Association of Victoria (SAV) staff for leading the SAWI service; and SAV and SAWI staff, members and clients for supporting the SAWI service evaluation. They also wish to thank Barwon Health staff who supported the SAWI team in identifying potential clients.
Conflict of interest
AT has received grant/research support from the National Health and Medical Research Council (NHMRC), AMP Foundation, Deakin University and the Stroke Foundation. IK has received grant/research support from the Medical Research Future Fund (MRFF), National Health and Medical Research Council (NHMRC) the Stroke Foundation, Stroke Association, National Health Service of Great Britain and Northern Ireland and the University of Technology Sydney.
Ethical approval
As quantitative data was collected as part of usual clinical care, the analysis and publication of this was covered by an Ethics Exemption granted by Barwon Health HREC (17/74). The qualitative sub-study received full ethical approval by Barwon Health HREC (18/225).
Funding
The service and evaluation work, including salary time for authors AT and JM, was funded by AMP Foundation.
Informed consent
As quantitative data was collected as part of usual clinical care, informed consent for data analysis and publication was not necessary. Participants of the qualitative sub-study provided informed consent prior to study participation.