
Abstract
BACKGROUND:
Disability
OBJECTIVE:
This study examined the moderating effect of disability acceptance on the negative effects of disability stigma on job satisfaction of people with disabilities.
METHODS:
164 participants working at the time of the survey completed questionnaires measuring disability stigma, disability acceptance, and job satisfaction. The associations among the three variables were examined using simple linear regression analyses. Hierarchical linear regression analysis was conducted to identify the moderating effect of disability acceptance after controlling disability type.
RESULTS:
Disability stigma (β=–0.17, p < 0.05) and disability acceptance (β=0.18, p < 0.05) were significantly associated with job satisfaction respectively. In the final model, disability acceptance moderated the relationship between disability stigma and job satisfaction (β=–0.16, p < 0.05). Specifically, the impacts of disability stigma on job satisfaction for participants with higher disability acceptance differed from those with lower acceptance.
CONCLUSION:
The current research suggests that disability acceptance plays a critical role for people with disabilities to cope with the negative impact of disability stigma. This result implies that disability acceptance should be an important focus of intervention to increase job satisfaction.
Introduction
According to labor statistics, the employee turnover rate has been constantly increasing over the past several years, rising from 42.6% in 2016 to 57.3% in 2020 (U.S. Bureau of Labor, 2022). Given the abundant studies showing that job satisfaction has a significant impact on job retention and turnover intention, the increasing turnover can be seen as at least in part reflecting workers’ low satisfaction at work. This is of concern because job satisfaction is closely related to employees’ quality of life and overall well-being (Rice et al., 1980; Sirgy et al., 2008). Job satisfaction is essential for psychosocial health and community participation, and plays a key role in living a fulfilling and meaningful life.
Job satisfaction in vocational rehabilitation
Feeling satisfied in one’s work seems more than a means of making a living for people with disabilities. According to work adjustment theory, employees’ work satisfaction is as important to predicting job retention as the employers’ satisfaction with the employees (Dawis, 2005; Dawis & Lofquist, 1984). Empirical evidence in the field of vocational rehabilitation (VR) has supported this theory; people with disabilities consistently have reported that fulfilling and meaningful participation in employment contributes to structuring adaptive identity, building relationships, and engaging in productive activity. It also results in increased well-being and active community participation (Kocman & Weber, 2018; Reichard et al., 2019; Repke & Ipsen, 2019). In sum, improving job satisfaction can be a direct and indirect way to improve the overall outcome of vocational rehabilitation.
Recent changes in federal law affecting VR services underscore the importance of understanding how people with disabilities perceive their work. Traditionally, VR research has measured employment outcomes based on objective indicators such as employment rates, working hours, wage level, and the number of job placements. However, the Workforce Innovation and Opportunity Act (WIOA) enacted in 2014 aims to shift state VR services focus toward “individualized determination of the strengths, needs, and interests of the individual with a significant disability (Sect. 361)” (Workforce Innovation and Opportunity Act, 2014). That is, the paradigm of VR services is changing in ways that improve the individualized quality placement by taking consumers’ subjective and unique characteristics into consideration. Increasingly, therefore, job satisfaction and related factors should be addressed in VR research as important outcome factors.
Disability stigma and job satisfaction
Despite the legislative tools to prevent discrimination in the workplace, an alarming number of employees with disabilities still report the experience of widespread stigma in the workplace and lower job satisfaction compared to their colleagues without disabilities (European Commission, 2015; Goldman et al., 2006). Disability stigma, characterized by negative attitudes as well as discriminatory behaviors based on structural power imbalance, is regarded as one of the biggest risk factors in the employment of people with disabilities (Corrigan, 2000). According to numerous studies, it has been found that stigma in the workplace is actualized at the structural and individual levels of the organization, thus significantly contributing to decreased job satisfaction (Di Marco, 2016).
On the structural level, stigma is reflected in discriminatory organizational culture. Employees with disabilities often face challenges due to the procedural injustice and lack of managerial assistance necessary to provide accommodation and shape an optimal work environment (Bezyak et al., 2021). The work difficulties that these employees experience are usually attributed not to organizational or structural limitations, but to individual limitations. Therefore, employees with disabilities are likely to be victims of a discriminatory judgment of their worth and value as members of the organization (McLaughlin et al., 2004). In such a discriminatory structure, employees with disabilities are often devalued and seen as less competent (Kirsh et al., 2009).
On the individual level, stigma toward disability is enacted and communicated through interpersonal interactions. For example, employers and managers are more concerned about the work skills of employees with disabilities than those without disabilities. Important tasks that require advanced skills or knowledge are less likely to be assigned to these employees and opportunities for advancement are relatively limited (Unger, 2002). Negative attitudes are also reflected in the form of avoidance, disrespect, and lack of assistance that cause problems in socialization, adaptation, and participation of employees with disabilities in the workplace (Brooks, 2019; Gromley, 2015; Kulkarmi & Lengnick-Hall, 2011; Lyubykh et al., 2020). These biased interactions are significant risk factors for decreased work adjustment and job satisfaction.
A more subtle but equally problematic effect of disability stigma in the workplace is that it can lead to self-stigma, also known as internalized stigma. Researchers have identified that self-stigma is associated with fewer opportunities for building relationships with colleagues, lower work engagement, low self-efficacy, and reduced job satisfaction (Brzykey & Boehm, 2021; Kourti et al., 2018). Link and Phelan (2001) explained in their stigma model that social labeling and perception of negative attitudes are the major components of developing self-stigma. In other words, perceived disability stigma in the workplace can contribute to increased employee self-stigma, bringing multiple negative consequences including damaged self-concept and maladaptive behavioral reactions (Corrigan & Rao, 2012).
However, although the negative effect of disability stigma is consistently reported, not every experience of stigma causes negative consequences or the development of self-stigma. The magnitude of the stigma can vary across individuals. The model of stigma proposed by Link and Phelan (2001) suggests that people encountering negative societal attitudes can react in three different ways: some people try to hide their disability due to shamefulness; some choose to withdraw from others for fear of social rejection; some try to communicate with others to reduce the negative attitudes around the disability. Also, in the face of prejudice or discrimination, there are people who actively resist stigma and advocate for themselves or for a group of people with disabilities (Caldwell, 2011; Nario-Redmond & Oleson, 2016). In rehabilitation research, scholars have tried to identify the factors that explain the difference in individuals’ reactions to stigma and that may reduce its negative effects.
Disability acceptance and disability stigma
Disability acceptance is conceptualized as a process of accepting loss caused by disabilities and changing personal value systems to realize individual strengths regardless of disability status (Dembo et al., 1956; Wright, 1983). In rehabilitation research, this has been discussed as a variable related to positive perspectives of people with disabilities on their own disability status. While the societal response toward disability is often to associate deficiency and impairment, people who have a higher level of acceptance are likely to view their disabilities as a non-devaluing condition, and even as a new source of capacity gained by endorsing a new set of values focused on unique strengths and possibilities (Dunn, 1994). Moreover, disability acceptance has been considered a common factor in the development of disability identity that leads to participation in the disability community and active advocacy for the rights of people with disabilities (Caldwell, 2011; Forber-Pratt et al., 2020). Thus, accepting one’s own disability provides a foundation for structuring a healthier personal/social identity and for developing more adaptive coping behaviors.
From the existing literature on acceptance of disability and its related effects, disability acceptance is associated with (a) change in personal value systems in a way that engenders focus on the individuals’ strengths and uniqueness; (b) use of adaptive and active coping strategies to deal with negative societal attitudes; and (c) increased psychological and cognitive flexibility that leads to adaptive emotions and behaviors when facing challenges and limitations derived from disability (Antonak & Livneh, 1995; Hayes et al., 1996; Wright, 1983). For employees with disabilities in the face of stigma in the workplace, disability acceptance can be a protective factor to prevent internalizing devaluation or shamefulness. It also can be a facilitator of direct coping to manage the negative work environments in an adaptive manner. Finally, those with higher disability acceptance can regulate their thoughts, emotions, and behaviors better in response to the disability stigma in the workplace (Gabryś, 2020; Kim, 2021).
Based on a review of previous studies, disability acceptance needs to be considered in the discussion of disability stigma and job satisfaction. The role of disability acceptance as a facilitator of job satisfaction as well as a protective factor from the adverse effects of disability stigma requires further examination. In sum, the main purpose of this study is to understand the role of acceptance in the relationship between disability stigma and job satisfaction. To this end, the research hypotheses are as follows:
Hypothesis 1. A higher level of disability stigma is associated with decreased job satisfaction.
Hypothesis 2. A higher level of disability acceptance is associated with increased job satisfaction.
Hypothesis 3. The effect of disability stigma on job satisfaction is moderated by disability acceptance.
Materials and methods
Procedures
Data used in the present analyses were provided through the Participation and Disability Dataset (PDD) (Fleming & Phillips, 2020; Phillips et al., 2022), a longitudinal study by Phillips and Fleming initially created in December of 2016 with a sample of 1,014 people in the United States with a variety of disability conditions. Follow-up studies were conducted in February 2017, September 2018, and February 2020. The data from the 2017 survey were used for the current research. Human subjects approval for this project was granted by the University of Wisconsin–Madison Institutional Review Board (Social Experience and Employment Survey, no. 2018-0923-CP002). Participants were recruited using a combination of the crowdsourcing data collection tools Amazon Mechanical Turk (MTurk) and TurkPrime (now CloudResearch) as described by Phillips and Fleming (Fleming et al., 2020; Phillips et al., 2022). MTurk is used by thousands of researchers to obtain sample participants while CloudResearch provides a more user-friendly interface and additional options for data collection (Litman et al., 2017).
The PDD Researchers worked directly with CloudResearch to identify participants with disabilities by asking MTurk participants whether they had a disability or chronic illness. Participants were paid at the same rate regardless of their response, reducing the likelihood of someone providing a false report. In follow-up with participants who self-reported as having a disability or chronic illness, participants were asked to list and describe all of their disabilities, and in the case of multiple disabilities, which they considered to be their primary disability. These disability descriptions were reviewed by the research team for face validity, with fewer than five participants deleted from the dataset as a result of this process. Participants with the same MTurk account or IP address were prevented from taking the survey more than once. Participants were administered an online survey via Qualtrics; those who completed the survey received a $4.00 incentive payment at each administration (Phillips et al., 2022).
Participants
A total of 164 adults (ages from 20 to 84) who were employed at the time of the February 2017 PDD survey were included in the present analyses. The mean age was 42.73 years (SD = 12.68, range = 20–84), with 52 (31.7% male, 111 (67.7% female, and 1 (.6% not identified. A total of 148 (90.2% reported as Caucasian. African American (3.7%), Latinx/Hispanic (1.8%), Asian or Pacific Islander (0.6%), or multi-racial (3.7% are followed. A total of 19 (11.6% held a high school diploma or GED, 40 (24.4% received some post-secondary education, 24 (14.6% held an associate degree, 54 (32.9% held a bachelor’s degree, and 27 (16.5% held a graduate degree. Regarding participants’ primary diagnosis, medical disability, including those with a variety of chronic health conditions represented the largest percentage of the sample (n = 50, 30.5%), followed by physical disability (n = 45, 27.4% and depression or anxiety (n = 42, 25.6%). Other diagnoses including neurocognitive, developmental, and intellectual disabilities consisted of 16.5% of the total sample (n = 27).
Measures
Disability stigma. The perception of disability stigma was measured using the 14-item Perceived Disability Stigma Scale (PDSS). These items were adapted and modified based on the Stigma Scale for Chronic Illness (SCCI) (Rao et al., 2009). This measurement includes the item asking about the perceived common stereotype in the community (e.g., “People in my community would treat people with disabilities just as they would anyone else”). All the items are scored on the 5-point Likert-type scale (1 = never, 5 = always). Total item scores are summated and higher score indicates higher perception of stigma. The Cronbach’s α for the sample in this study was 0.93.
Disability acceptance. Disability acceptance was measured using the 10-item Acceptance of Chronic Health Conditions Scale (ACHC) (Stuifbergen et al., 2008). This is a single factor measurement for assessing disability acceptance level based on the lived experience of people with disabilities or chronic health conditions. All the items are measured based on level of agreement with 10 statements (e.g., “I can’t conquer my disability, but I can adapt to it”) on a 5-point Likert Scale (1 = strongly disagree, 5 = strongly agree) and the sum of the item scores reflects the level of disability acceptance. A higher score indicates higher level of disability acceptance. Cronbach’s α in this study was 0.80.
Job satisfaction. The 5-item Brief Overall Job Satisfaction measure (Judge et al., 1998), was used to assess job satisfaction. This instrument measures respondent’s affective response to his/her job by asking the perception concerning the current work (e.g., “I feel fairly well satisfied with my present job”, and “On most days I am enthusiastic about my work”). Items are measured on a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree). The total score is computed by summing each item score, with higher scores reflecting higher job satisfaction. Cronbach’s α in this study was 0.92.
Data analysis
Descriptive analysis was conducted to identify the demographic characteristics of the research participants. Mean comparison using analysis of variance (ANOVA) was used to examine the differences in independent and dependent variables across the groups with different primary diagnoses. Linear regression analysis was performed to examine the association between stigma and job satisfaction, and acceptance and job satisfaction respectively. Finally, hierarchical multiple regression (HMR) analysis was conducted after controlling the primary diagnosis to examine the relationship between disability stigma, job satisfaction, and acceptance. To evaluate the moderating effect of disability acceptance, the method proposed by Baron and Kenney (1986) was used. The dependent variables, stigma, acceptance, and the interaction term were entered sequentially in a three-step analysis. Statistical assumptions were checked in multiple ways using descriptive statistics, P-P plot, correlations, and test of variance inflation factors (VIF). All data analyses were conducted using Statistical Package for Social Scientists (SPSS) version 26.0 (IBM Corp., Armonk, NY, USA).
Results
Preliminary analyses
Preliminary analyses were conducted to examine the assumptions of normality, linearity, homoscedasticity, and multicollinearity. The detailed statistics showing normality of the data are shown in Table 1; all values of skewness were smaller than 2 and kurtosis was smaller than 7 (Curran et al., 1996). The assumptions of homoscedasticity and linearity were satisfied based on analysis of the P-P plot of the regression showing that the slope of standardized residual was near 45 degrees and a standardized scatterplot appearing as a near-rectangular band (Garson, 2012). The assumption of multicollinearity was also fulfilled, with the correlation coefficients less than .80 (Dattalo, 2013) and VIF less than 5 (maximum VIF = 1.44) in the regression model.
Descriptive statistics (n = 164)
Descriptive statistics (n = 164)
Criteria for normality: skewness > 2; kurtosis > 7; multicollinearity: intercorrelations r > 0.80; *p <0.05. **p <0.01.
Based on the literature indicating possible discrepancies in stigma and acceptance depending on the disability type (McLaughlin et al., 2004; Werner & Shulman, 2015), two-way ANOVA was performed to test the differences in predictors and outcome variables depending on the primary diagnosis. As shown in Table 2, the result showed that significant differences existed in the level of job satisfaction across the groups with different diagnoses (F = 4.63, p < 0.01). Specifically, people with depression or anxiety reported significantly lower levels of job satisfaction compared to those with physical and other disabilities. There were no significant differences in level of disability stigma and acceptance based on the primary diagnoses.
Primary diagnosis and mean differences in disability stigma, acceptance, and job satisfaction
Primary diagnosis and mean differences in disability stigma, acceptance, and job satisfaction
**p <0.01.
Simple linear regression analyses demonstrated significant relationships of stigma and acceptance with job satisfaction. Specifically, disability stigma (β=–.17, P < 0.05) was negatively associated with job satisfaction, and acceptance (β=0.18, p < 0.05) was positively associated with job satisfaction. Further detailed information is shown in Table 3.
Linear regression analyses for relationships of stigma and acceptance with job satisfaction
Linear regression analyses for relationships of stigma and acceptance with job satisfaction
*p <0.05.
The mean comparison analysis showed that participants’ level of job satisfaction was significantly different across the participants’ primary diagnoses. Therefore, four dummy variables were created for primary diagnosis to be controlled in the regression analysis. To reduce multicollinearity, predictor (i.e., disability stigma) and moderator (i.e., acceptance) variables were mean-centered, and the interaction term (i.e., disability stigma x acceptance) was created. As shown in Table 4, three-step hierarchical multiple regression analysis was performed after controlling the primary diagnosis variable.
Hierarchical regression model of moderating effect under primary diagnosis variable controlled (n = 164)
Hierarchical regression model of moderating effect under primary diagnosis variable controlled (n = 164)
*p <0.05. **p <0.01.
In step 1, the model accounted for approximately 9.4% of the total variance of job satisfaction after the effect of primary diagnosis variable was controlled (F(4, 164)=4.15, p < 0.05). In step 2, the model including primary diagnosis, stigma, and acceptance accounted for approximately 11.2% of the variance in job satisfaction (F(5, 164)=3.98, p < 0.05). In step 3, the interaction of disability stigma and job satisfaction explained an additional 2.3% of variance in job satisfaction (F(6, 164)=4.06, p < 0.05). Although the amount of variance accounted for by the interaction was small, McClelland and Judd (1993) noted that a significant interaction effect should be regarded as important regardless of its contribution to the variance in outcome variable due to the difficulty of detecting this effect in field research.
Figure 1 shows the graphic information regarding the interaction effect of disability acceptance. Based on the recommendation of Cohen and Cohen (1983), high and low acceptance regression lines were plotted separately. These lines show how the relationship pattern between disability stigma and job satisfaction is moderated depending on the acceptance level. The job satisfaction of the high acceptance group increases faster as the disability stigma decreases, but in the case of the low acceptance group, the level of job satisfaction maintains as the disability stigma level decreases.
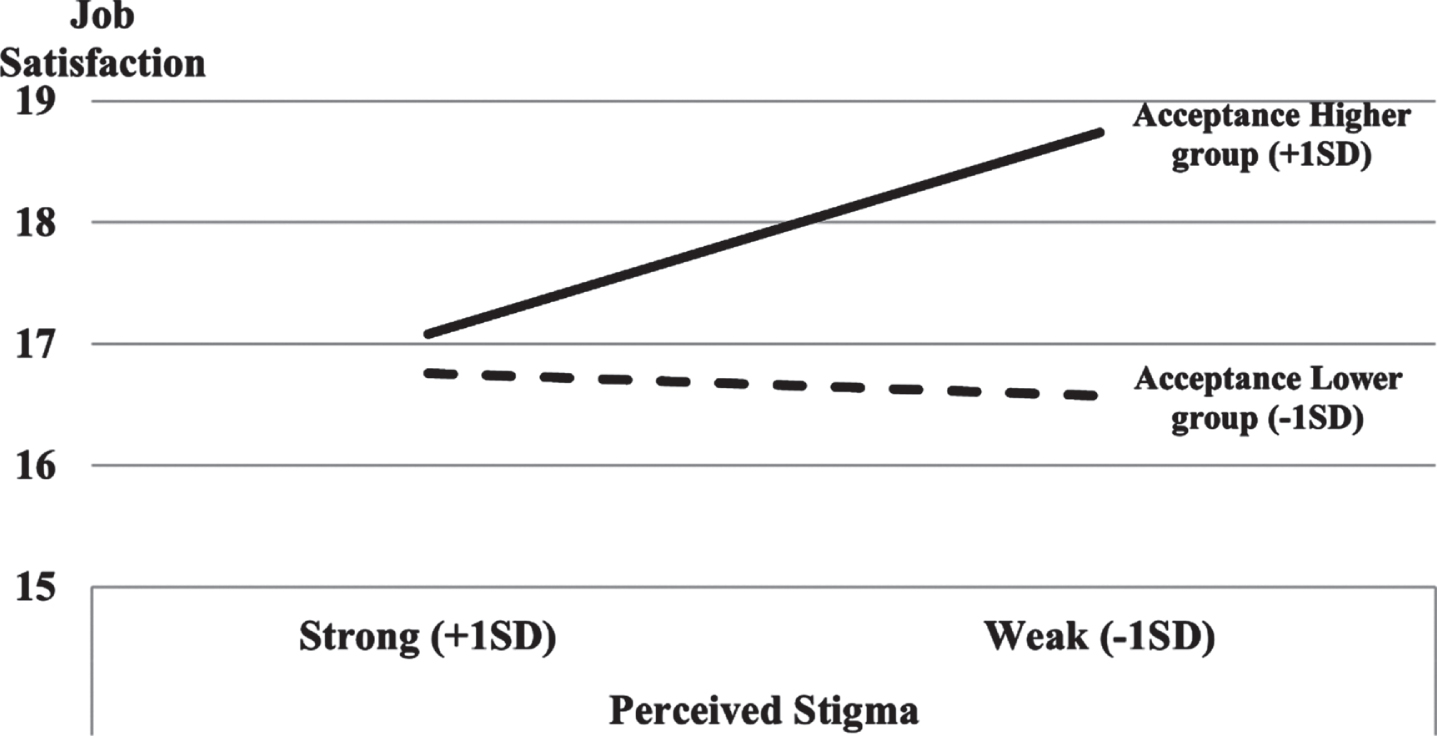
Moderating effect of disability acceptance.
The current study aimed to extend the understanding of job satisfaction of employees with disabilities in relation to disability stigma by exploring the moderating effect of disability acceptance. As in the research hypothesis, disability stigma and disability acceptance are respectively associated with job satisfaction, and disability acceptance moderates the negative effect of disability stigma on job satisfaction. This role of disability acceptance corresponds well with the goal of vocational rehabilitation that aims at maximizing the job satisfaction of people with disabilities. Further, the results provide evidence for the potential benefits of improving disability acceptance in vocational rehabilitation services for people with disabilities.
In the present study, perception of disability stigma negatively affected job satisfaction, but a higher level of disability acceptance contributed to increased job satisfaction. This research outcome is consistent with previous studies that have demonstrated the negative effect of stigma on a wide range of psychosocial outcomes, and that have suggested the facilitative role of disability acceptance in the psychosocial adjustment process (Ferrie et al., 2020; Monden et al., 2021). In addition, considering a body of literature indicating that job satisfaction is closely associated with overall psychosocial well-being and quality of life (Bowling et al., 2010; Sirgy et al., 2008), this effect of disability stigma and disability acceptance needs to be taken into consideration in the developing and improving vocational rehabilitation services for people with disabilities.
The results also demonstrate the moderating effect of disability acceptance in the relationship between the disability stigma and job satisfaction level. More specifically, in the current sample, for those participants with disability acceptance levels higher than 1 SD above the mean, job satisfaction is steeply increased as the level of disability stigma decreases. However, for those with disability acceptance levels lower than 1 SD below the mean, job satisfaction is slightly reduced as the disability stigma weakens. This change pattern suggests that the job satisfaction of the group with higher disability acceptance could be greatly affected by perceived disability stigma compared to that of the group with lower disability acceptance. This pattern of moderation seems consistent with Link and Phelan’s stigma model (2001). As suggested by this model, stigmatized individuals display different reactions when encountering negative attitudes. People who feel shamefulness or fear due to their stigmatized identity, often associated with lower disability acceptance, are likely to avoid or withdraw from the stigmatizing situations or individuals in the workplace. These individuals’ satisfaction level would be less affected by the discriminatory work conditions, but it also would be less likely to be affected by any change in stigma perception, even when the stigma is decreased because they might want to keep trying to be distant from any stigma issue in the workplace. In contrast, people who actively cope with the stigmatization and injustice, usually associated with higher disability acceptance, are likely to be more attentive to change in relation to stigmatization in their workplace. Since they want to reduce the negative attitudes and improve the work environment, their job satisfaction could be significantly improved as the level of disability stigma is decreased. This result provides a meaningful practice implication in vocational rehabilitation service provision. Taking into the moderation of disability acceptance consideration, reducing stigma itself might be insufficient to improve the job satisfaction of people with disabilities. Individual disability acceptance needs to be considered to play an important role in predicting how a perceived change in stigma affects job satisfaction.
Looking more deeply, the differences in reactions to stigma and the pattern of moderation identified here could be explained by the internal valuation/devaluation process closely related to stigmatization and disability acceptance. Stigma toward disability, whether internal or environmental, is formed based on the underlying assumption that disability is an impairment that equates with core personal identity (Martz, 2004; Thoits, 2011). However, acceptance of disability counteracts (or prevents) this devaluation through normalizing disability as only one facet of individual differences, leading to enlarging the value system by focusing on personal strengths and assets (Dembo et al., 1956/1975; Wright, 1983). That is, acceptance is an antithesis of stigmatization characterized by the devaluation of disability. In this vein, if a person with higher disability acceptance is placed in a work environment with higher stigma, this person is more likely to recognize the social and structural devaluation, resist the negative consequences of stigma, and feel dissatisfied. Further, this emotional response appears rather adaptive as it will likely be followed by active coping for change. Wright (1983) suggested that higher disability acceptance is associated with developing an adaptive coping strategy focusing on what the person is capable of. From empirical findings regarding disability acceptance and disability identity, it has been implied that people with higher disability acceptance are more involved in actions for change, such as advocacy, empowerment, and education (Forber-Pratt et al., 2020; Nario-Redmond & Oleson, 2016; Rice et al., 1980; Smith & Muller, 2021).
From a practice perspective, the results of this study indicate that improving disability acceptance should be an important focus of intervention along with reducing stigma to increase overall work satisfaction of people with disabilities. The suggestions for practical applications on how to promote disability acceptance and how to reduce stigma in the workplace can be made based on the previous studies. Participating in the disability community is one of the common factors frequently discussed in facilitating disability identity (Forber-Pratt et al., 2017). Positive interaction among the members of this community leads to a strengthened disability identity through modeling and social learning. Individuals who identify themselves with the community learn and internalize the norms and cultures usually associated with increased empowerment and embracing a positive perspective on disability status (Forber-Pratt & Zape, 2017). Rehabilitation counselors could support the consumers to connect and build a positive relationship with the disability community. Utilizing peer support or self-help group can be a supplemental way to help consumers to make a positive relationship with disability community.
Regarding the interventions on stigma toward people with disabilities, Corrigan and colleagues performed a meta-analysis (2012) on the effectiveness of the strategies to reduce the stigma in the general population. The results presented that direct interaction with people with disabilities was the most effective way to reduce and prevent negative attitudes, and education about disability was the second effective. In addition, a systematic review focusing on the needs of business showed that diversity and inclusivity in the workforce contributed to business profitability by structuring a safe work environment, improving work morale, and promoting a positive reputation of the corporation in the public (Gelashvili et al., 2015; Lindsay et al., 2018). In sum, reducing stigma in the workplace is for the good of the business itself as well as employees with disabilities. Grounded on these findings, rehabilitation counselors can effectively emphasize that reducing stigma helps to meet the needs of employees with disabilities and businesses/employers. In this way, rehabilitation counselors can be collaborators to facilitate an inclusive work culture by helping reduce disability stigma in the workplace.
Several limitations in this study should be noted. First, the relatively small sample size and limited disability type of the participants may limit the generalizability of the research findings. Most of the participants reported that their primary disability is medical, physical, and psychiatric disabilities (depression and anxiety). Given that the effect of disability stigma on job satisfaction was not significant when the disability type was controlled, considering distinctive characteristics depending on the disability types seems an important task for future research. Additionally, the cases were gathered using online crowdsourcing that could limit the participants to virtual employees, but detailed information regarding participants’ employment (e.g., job types, working duration) was not presented. Future studies should gather data from diversified paths, including online and offline, from participants with diverse disability types and job types. Due to the limitation of the cross-sectional study design, causality among the predictors and dependent variables cannot be inferred. A longitudinal study would further delineate the causal relationships among the variables according to the change in disability acceptance. Third, there were limitations in the measurement used in the survey. Although disability acceptance is a comprehensive construct including change in value system, cognitive/psychological flexibility, and behavioral coping style, the measurement utilized in the survey was developed to assess changing value. Finally, 90% of participants identified themselves as White. The sample size of the rest of the racial/ethnic groups consists of only 10%. Such a relatively low representation can cause systemic issues regarding disproportionate socioeconomic status or social capital that might confound the research outcomes when uncontrolled. It limits the generalizability of the research outcomes to the different racial/ethnic groups.
Conclusion
The current research supports the psychosocial importance of disability acceptance as a potential moderator for the disability stigma. It was also independently associated with increased job satisfaction. Overall, the results of this study suggest that recognizing, assessing, and intervening for enhancing disability acceptance may have potential benefits in the field of vocational rehabilitation, which has central goals of reducing stigma in the workplace and increasing job satisfaction of people with disabilities. According to the research finding, if the overall disability acceptance is low increasing job satisfaction would be difficult even when the stigma in the workplace is reduced. However, if the disability acceptance can be increased, it can be expected that decreased stigma can be along with the significant increment of job satisfaction together. That is, efforts to promote disability acceptance need to be accompanied in order to pursue the two major goals of stigma reduction and improvement of job satisfaction. This would eventually contribute to improving the effectiveness and efficacy of the vocational rehabilitation services.
Footnotes
Acknowledgment
The author would like to thank Dr. Brian Phillips and Dr. Allison Fleming for providing the dataset analyzed in this study. The dataset was derived from their longitudinal study, entitled the Participation and Disability Dataset (PDD). The author thanks Dr. Malachy Bishop for providing constructive feedback and revision suggestions throughout the research process.
Conflict of interest
The author declares that no conflict of interest exists.
Funding
No funds, grants, or support were received during the preparation of this manuscript.
Data availability
The datasets analyzed during the current study are not publicly available because they constitute an excerpt of research in progress but are available from the corresponding author on reasonable request.
Ethics statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Human subjects approval for this project was granted by the University of Wisconsin–Madison Institutional Review Board (Social Experience and Employment Survey, no. 2018-0923-CP002).
Informed consent
Informed consent was obtained from all individual participants included in the study.