
Abstract
BACKGROUND:
Spirometric prediction equations are used to evaluate lung function in the clinical setting. However, such equations are not yet available for First Nations populations. The purpose of this study is to derive appropriate spirometric reference equations for a group of Cree First Nations school-aged children and adolescents living in rural Saskatchewan, Canada.
METHODS:
Spirometric data was collected from Cree First Nations cohort living in rural Saskatchewan, Canada. In the baseline survey, 351 children and adolescents participated and of these 134 were identified as healthy non-smoking individuals. The predicted values and Lower Limit of Normal (LLN) of spirometric indices were calculated for school-going children and adolescents (ages 6–17 years for males and 6–14 years for females). The spirometric indices were assumed to follow a Box-Cox-Cole-Green (BCCG) distribution with median,
RESULTS:
Two-sample
CONCLUSION:
This study provides the baseline lung function reference equations for Cree First Nations children and adolescents. This baseline study provides a platform for future studies, which can be conducted to improve the accuracy of the predicted lung function indices for such study cohort.
Introduction
Respiratory diseases are one of the leading causes of morbidity for children (Bulkow et al., 2012). The prevalence of pulmonary diseases is unusually high in indigenous children (McCuskee et al., 2014), and a large number of them require repeated hospitalization and admission to pediatric intensive care unit (ICU) (Banerji et al., 2001). Childhood respiratory problems are associated with chronic lung diseases in adulthood (Singleton et al., 2000). Spirometric data along with age, height, weight and ethnicity are used to develop reference equations, based on statistical methods involving regression analyses (Veale et al., 1997). Such equations are then used to predict lung function values for an individual given his/her age, sex, height, weight and ethnicity.
The ethnicity of the children has an effect on lung function and has been examined by several authors (Azizi & Henry, 1994). For example, the predicted lung function values for African-American children are lower than those for Mexican-American and Caucasian children (Hsu et al., 1979; Hsi et al., 1983; Kirkby et al., 2013). In Australia, Caucasians children have been shown to have higher lung function values compared to Aboriginal children (Watson et al., 1986), and children of European regions tend to have higher lung function values compared to children of Asian origin (Wesley et al., 1989; Johnston et al., 1987). Differences in lung function were also observed between Caucasian, Chinese and Indian populations (Yang et al., 1991). It is evident that ethnic differences in lung function begin in childhood due to different physical stature between different ethnic groups (Yang et al., 1991).
Quanjer et al. (2012) provided all-age multi-ethnic spirometric reference equations that can be used globally for different ethnic groups including Caucasian, African-American, North-East Asian, South-East Asian and Others (people with mixed-ethnicity). The authors considered for an adjustment for ethnicity while modeling lung function indices.
Some studies (Gutierrez et al., 2004; Tan et al., 2011; Karunanayake et al., 2015) on developing spirometric reference equations for Canadians have been conducted. However, these studies were aimed at deriving lung function prediction equations for Caucasian adults living in Canada. Sin et al. (2004) conducted a pilot study to provide lung function values for school-going First Nations children living in Northern Alberta. The spirometric reference equations calculated from Caucasian population living in the United States provided by Hankinson et al. (1999) were used for First Nations children in this study. Observed lung function values were compared with the LLN values for the assessment of airflow obstruction. The authors found that 25% of the First Nations children showed evidence of airflow obstruction. Sin et al. (2004) suggested that asthma is under-diagnosed and under-recognized for First Nations children. Therefore, spirometric reference equations for non-First Nations people may not be appropriate for First Nations people, as the equations may be influenced by ethnicity. Moreover, adult equations cannot be used for children, as lung function increases with age until adulthood and starts to decline with age (Chen et al., 2005). At present, there are no specific spirometric reference equations available for First Nations people in Canada, including children. Coates et al. (2016) provided reference equations for Canadian population which considered including North American Indians, Inuits or Métis, but not First Nations people.
This analysis is focused on deriving appropriate reference equations for Cree First Nations children and adolescents to improve diagnostic accuracy in the assessment of respiratory disease. The results from this study will be compared with the equations provided by Hankinson et al. (1999) to see if the application of reference equations calculated from Caucasian children and adolescents is appropriate for Cree First Nations people.
Materials and methods
Data source and variables
Lung function data for children and adolescents (ages between 6 to 17 years) from Saskatchewan First Nations Lung Health Project (FNLHP) were used to derive reference equations.
There were a total of 351 children and adolescents (47% males and 53% females), who completed a baseline survey. The survey questionnaire included questions regarding their past and current health conditions, lifestyles, personal and family history of chronic diseases. The clinical component of the study assessed anthropometric measurements (standing height, weight, and waist circumference), blood pressure, pulmonary function testing (FVC, FEV
Literature (Hsu et al., 1979; Burity et al., 2013; Dickman et al., 1971; Miller et al., 1977; Roizin et al., 1993; Wall et al., 1982) suggests that the most important covariates to predict lung function values are height and age. The general recommendation is to calculate prediction equations based on the healthy individuals. Therefore, a reduced dataset of healthy individuals was considered to calculate reference equations for FVC, FEV
Statistical methods
Statistical methods to calulate lung function prediction equations are primarily based on regression models. Lung function values often exhibit a curved relationship with age. For skewed lung function data, the Generalized Additive Models for Location, Shape and Scale (GAMLSS) method is more appropriate to develop prediction equations, as this method does not require a specific distributional assumption for the response. Several authors (Quanjer et al., 2012; Wypij et al., 1993; Stanojevic et al., 2008; Koopman et al., 2011; Rochat et al., 2013) have used Generalized Additive Models (GAM) (Hastie & Tibshirani, 1986, 1990) or the extended version, GAMLSS for the derivation of lung function prediction equations.
GAMLSS is a framework for modelling the response variable (e.g., FVC,
Let us consider the following matrices,
Let
with the transformed response
for
where
Hence, as a simple example, we have assumed that
The shape (skewness) parameter with identity link can be modeled as follows:
where
The GAMLSS package of R was proposed by Rigby and Stasinopoulos (2010), where the Rigby and Statsinopoulos (RS) algorithm can carry out the iterative procedure to maximize the log-likelihood function to obtain the estimate of the models of median, coefficient of variation and skewness of the data.
This section focuses on calculating the Lower Limit of Normal (LLN) of the lung function indices. As described in Quanjer et al. (2012), for spirometric tests, the suggestion is to use 90% (NOT 95%), and two-sided (NOT one-sided) for calculating the LLN. Thus the remaining 10% are equally distributed in the two tails with 5% each side. Use of 90% lead to the fact that 5% of the population are considered to have too low values as opposed to 2.5%, that is, a larger portion of the population (5%) have too low values.
The formula for calculating the LLN (i.e.,
For
Therefore, the formula for calculating lower
Using this formula, the LLN can be calculated for spirometric indices based on the reference model.
The Akaike information criterion (AIC), which was proposed by Akaike (1974) is used for model selection.
The summary statistics of the study variables (age, height, FVC, FEV
Summary statistics of the study variables for a sample of 134 Cree First Nations healthy children and adolescents
Summary statistics of the study variables for a sample of 134 Cree First Nations healthy children and adolescents
Suppose that the distribution of the response (lung function) variable
is a
where
Initially we considered several models based on the order
Order,
Comparison of the fitted plots of lung function indices for males with other study; solid curves indicate predicted median lung function based on GAMLSS; dashed curves indicate predicted mean lung function based on the study of Hankinson et al. (1999).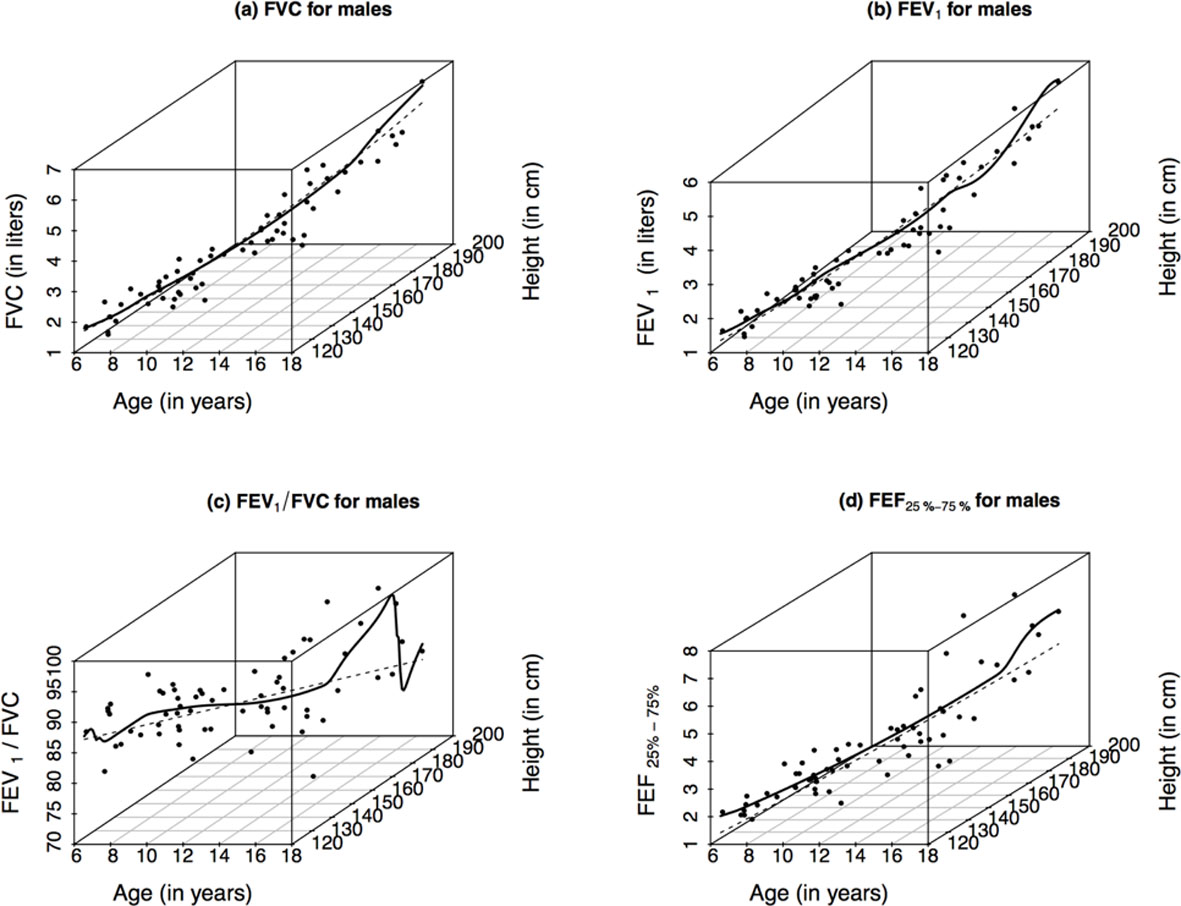
As indicated by scatterplots of Figs 1 and 2, the observed values of the lung function indices increase with both age and standing height. However, the FEV
Comparison of the fitted plots of lung function indices for females with other study; solid curves indicate predicted median lung function based on GAMLSS; dashed curves indicate predicted mean lung function based on the study of Hankinson et al. (1999).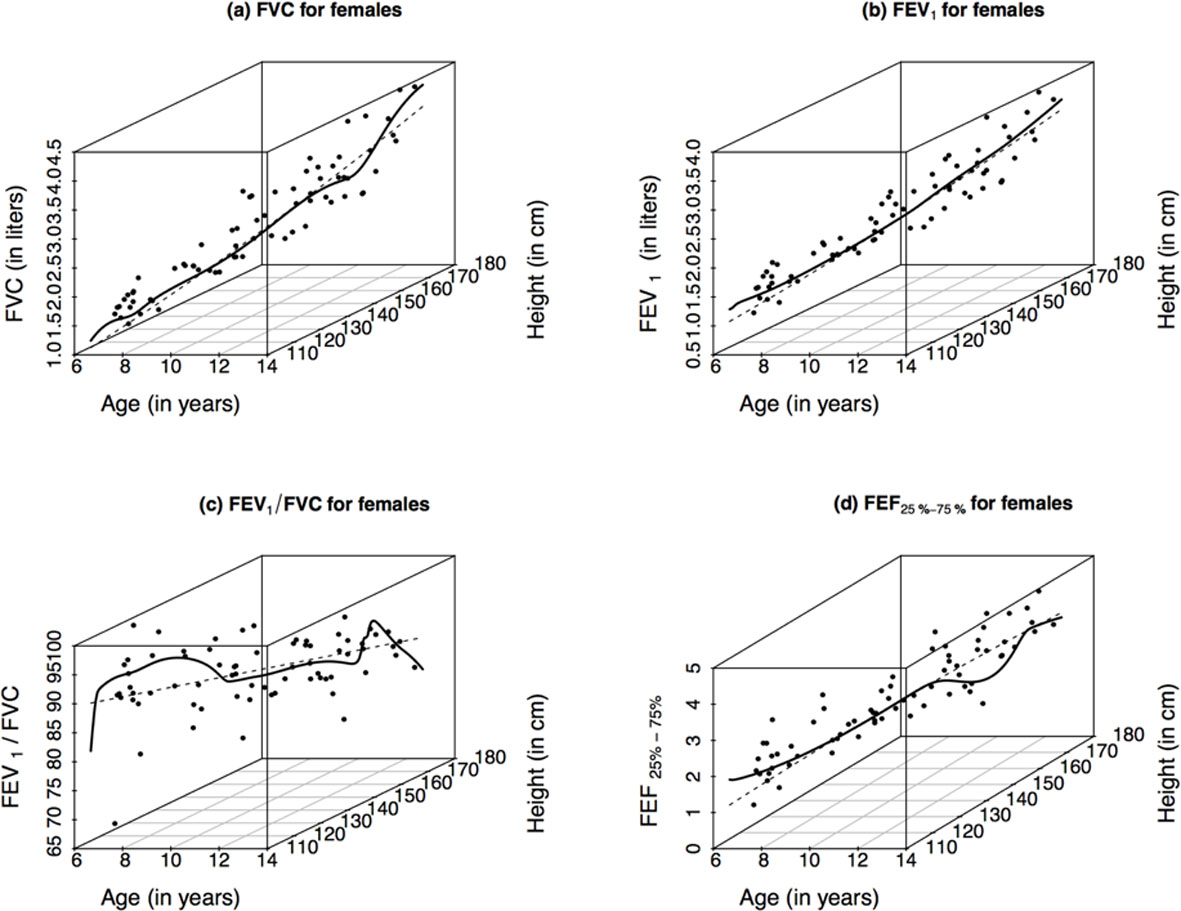
The predicted models for lung function indices of boys and girls are provided in Tables 3 and 4. From the parameter estimates, we can see that the polynomial order for the model of
Prediction equations for log(FVC) and log(FEV
) resulting from GAMLSS analyses
Prediction equations for log(FVC) and log(FEV
Prediction equations for
The slope parameters for males were significant (
A comparison among the fitted median curves for FVC and FEV
Height-age adjusted median reference values for FVC and FEV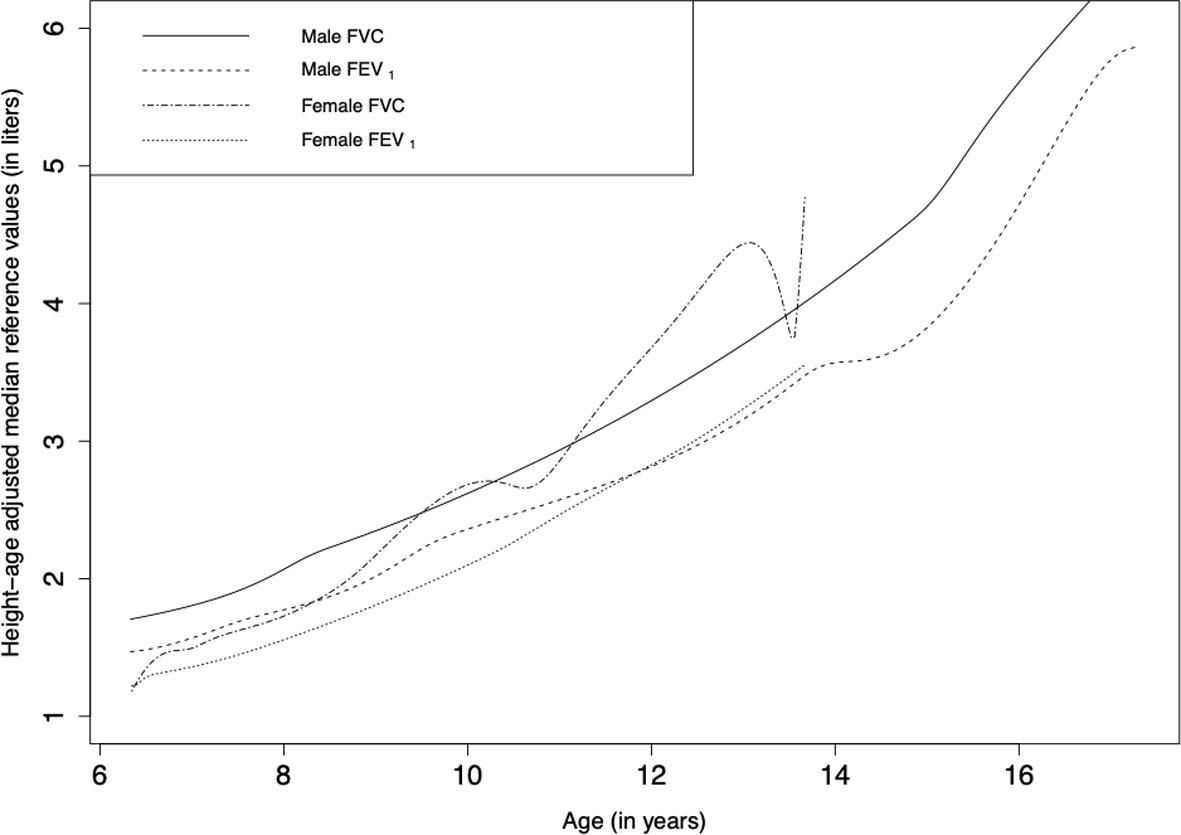
The fitted curves for the lower
Lower Limit of Normal (LLN) for the median of lung function indices (males); solid line represents the height and age-adjusted median curve, dashed line represents the height and age-adjusted LLN curve.
Lower Limit of Normal (LLN) for the median of lung function indices (females); solid line represents the height and age-adjusted median curve, dashed line represents the height and age-adjusted LLN curve.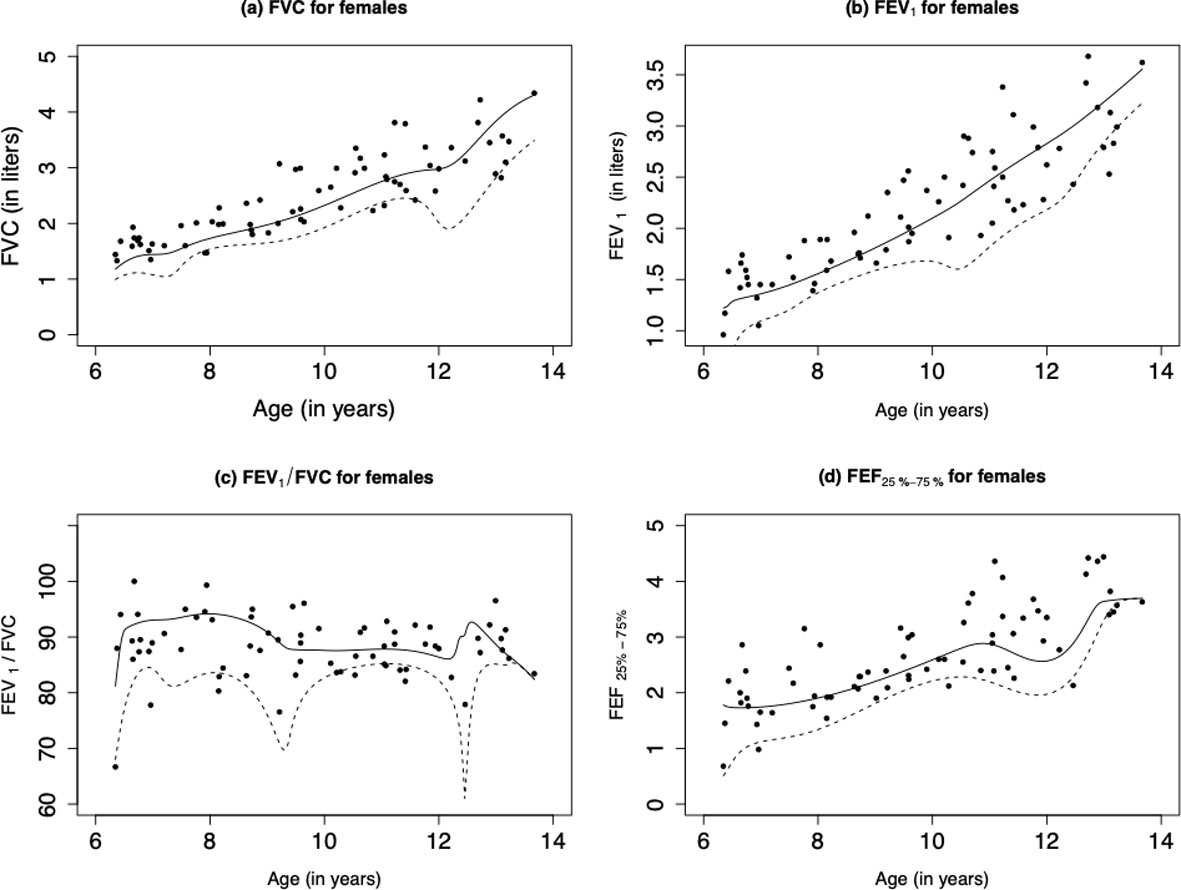
The results from this study are compared with the results from Hankinson et al. (1999). The equations proposed by Hankinson et al. (1999) is different than the results calculated in this study. The fitted plots of the lung function indices based on this study and the one by Hankinson et al. (1999) are given in Figs 1 and 2. Although the predicted curve calculated by Hankinson et al. (1999) fitted the data reasonably well, but it was not able to capture the non-linear relationship between anthropometric measurements and lung function.
Discussion
To the best of our knowledge, this is the first study to provide specific spirometric reference equations for Cree First Nations children and adolescents living in Canada. Well established reference equations provided by Hankinson et al. (1999) for Caucasians is not applicable to the studied population making specific equations necessary. They were calculated using an advanced statistical algorithm, GAMLSS (Rigby et al., 2019), where polynomial bases were considered to capture the non-linear relationship between lung function and anthropometric measurements. Increasing the order of the polynomial bases leads to over parametrization of the models, even though it captures more non-linearity of the data. Therefore, polynomial order ranging from one to five were examined to identify the most efficient model for the lung function indices. Akaike Information Criteria (AIC) showed that polynomial order ranging between one to four are more useful to model the spirometric indices for First Nations children and adolescents’ cohort. This is an advanced approach for modelling lung function indices, which was used to develop the GLI multi-ethnic reference equations by Stocks et al. (2012); Langhammer et al. (2016) and Cooper et al. (2017).
The models of lung function in females had higher order of polynomial bases compared to males, since the observed values of spirometric indices for females exhibited a more curved nature compared to males. The predicted values for females and LLN for FVC and FEV1 were lower until the age of 9 when compared to males. Previous studies have shown that maternal smoking during pregnancy has an adverse effect on lung function (Balte et al., 2016; Zacharasiewicz, 2016; McEvoy & Spindel, 2017), which is more prevalent in female subjects compared to their male counterparts (Tager et al., 1995). In our study, 36.2% of the mothers reported to have smoked during their pregnancy, which may explain differences observed.
We speculate that the irregular shape of FEV
Another factor that must be taken into consideration is that household smoking rates were high in the study sample. In this study, approximately 40% of households were exposed to second-hand smoking. Thus, obtaining a healthy sample with no smoke exposure was challenging in this population. As such, there is possibility that children included in this analysis, although non-smokers, were not indirectly exposed to significant amounts of second-hand smoke.
There is tremendous diversity among First Nations peoples in Canada. As such, the results from this study may not be generalizable to other First Nations groups in Canada.
Conclusions
We have provided a tentative baseline spirometric reference values (FVC, FEV
Footnotes
Acknowledgments
Ms. Rifat Zahan takes responsibility for the integrity of the analysis and contents of the manuscript. The First Nations Lung Health Project was funded by a grant from the Canadian Institutes of Health Research “Assess, Redress, Re-assess: Addressing Disparities in Respiratory Health among First Nations People”, CIHR MOP-246983-ABH-CCAA-11829. The First Nations Lung Health Project Team consists of: James Dosman, MD (Designated Principal Investigator, University of Saskatchewan, Saskatoon, SK Canada); Dr. Punam Pahwa, PhD (Co-Principal Investigator, University of Saskatchewan, Saskatoon SK Canada); Jo-Ann Episkenew, PhD (Co-Principal Investigator (deceased), Former Faculty of Indigenous People’s Health Research Centre, University of Regina, SK Canada), Sylvia Abonyi, PhD (Co-Principal Investigator, University of Saskatchewan, Saskatoon, SK Canada); Co-Investigators: Mark Fenton, MD, John Gordon, PhD, Bonnie Janzen, PhD, Chandima Karunanayake, PhD, Malcolm King, PhD, Shelly Kirychuk, PhD, Niels Koehncke, MD, Joshua Lawson, PhD, Greg Marchildon, PhD, Lesley McBain, PhD, Donna Rennie, PhD, Vivian R Ramsden, RN, PhD, Ambikaipakan Senthilselvan, PhD; Collaborators: Amy Zarzeczny, BA, LLM; Louise Hagel, MSc, Breanna Davis, MD, John Dosman, MD, Roland Dyck, MD, Thomas Smith-Windsor, MD, William Albritton, MD, PhD; External Advisor: Janet Smylie, MD, MPH; Project Manager: Kathleen McMullin, MEd; Community Partners: Jeremy Seeseequasis, BA; Raina Henderson, RN; Arnold Naytowhow; Laurie Jimmy, RN. We are grateful for the contributions from Elders, community leaders, School Boards, School Principals, teachers that facilitated the engagement necessary for the study, and, all parents and children who donated their time to participate. Training support was also provided by Western Regional Training Center (WRTC) for Health Services Research (HSR).