
Abstract
Fetus in fetu (FIF) is an extremely rare condition (1/500,000 live births) in which a fetiform structure is incorporated into the body of its twin. FIF can be a diagnostic dilemma due to its similarity to a teratoma, but identification of FIF is important for subsequent medical and surgical management. We compare two cases of fetal masses diagnosed on prenatal imaging that were later identified as FIF through further radiological, surgical, and pathologic evaluation. We use these cases to illustrate key pre- and postnatal features of FIF and highlight the benefits of prenatal detection and follow-up for postnatal management.
Case 1
A 27-year-old primagravida was referred to Children’s National Health System Fetal Medicine Institute for evaluation of a fetal sacral mass noted on routine prenatal ultrasound (US). A level 2 US at 27 weeks gestation showed an exophytic complex mass comprised of soft tissue, cystic foci, and scattered bones (Fig. 1a). Fetal magnetic resonance imaging (MRI) demonstrated the mass emanating from the sacrococcygeal area with extension into the low pelvis (Fig. 1b). The mass measured 10 cm×6.4 cm×4 cm and contained a structure resembling a lower extremity (Fig. 1c). Imaging studies, diagnostic implications, and management strategies were reviewed with the family by a multidisciplinary team comprised of a fetal radiologist, neonatologist, genetic counselor, and pediatric surgeon.
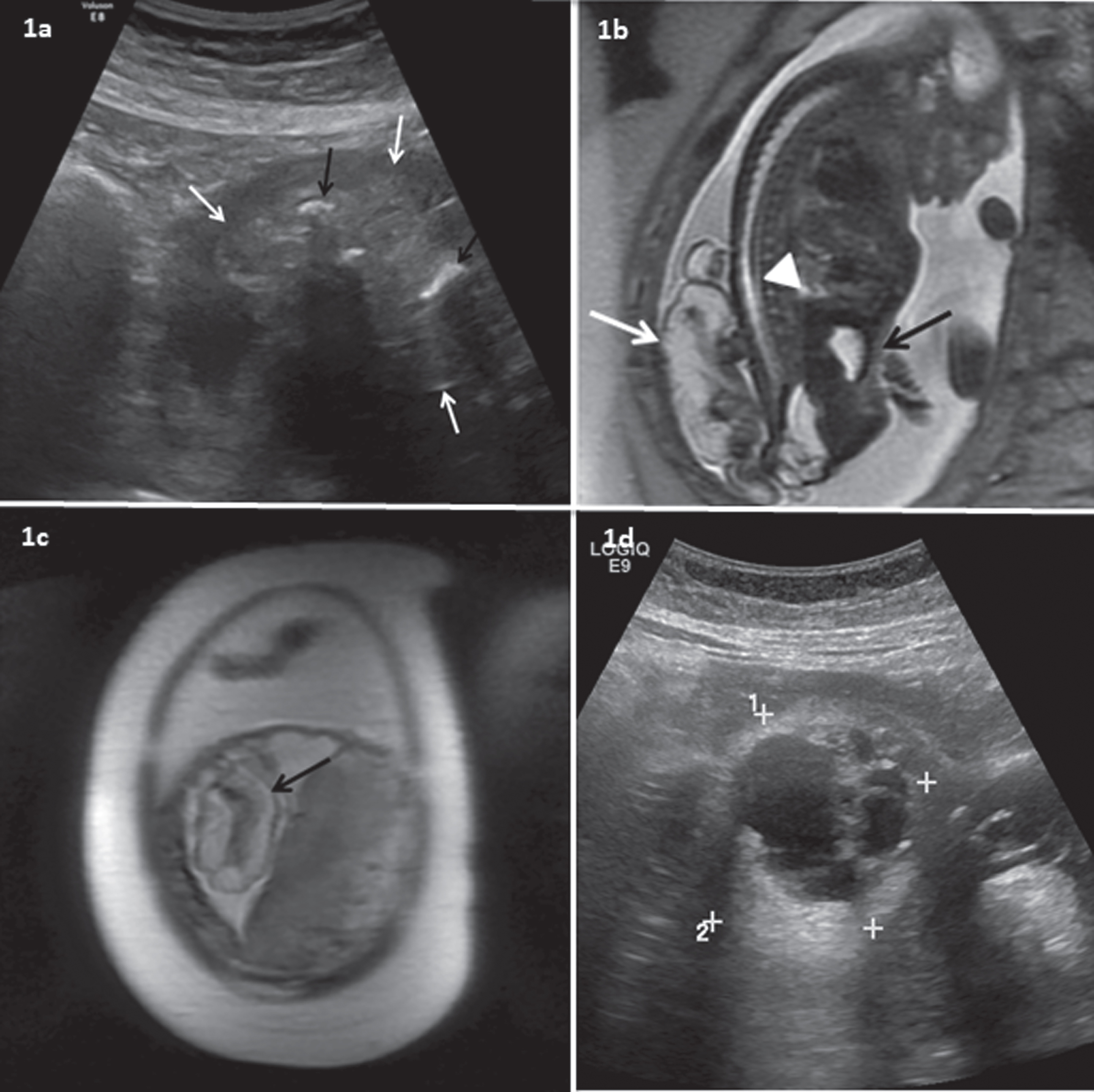
(a) Case 1 at 26 weeks gestation. Transverse US view of the mass (white arrows) with several intra-lesional bones (black arrows). (b) Case 1 at 26 weeks gestation. Sagittal MR image of the fetus demonstrates a complex cystic and solid mass (white arrow) emanating from the coccygeal region, with extension into the low pelvis. The fetal bladder (black arrow) appears unobstructed and the spinal cord conus (white arrow head) terminates at the appropriate level. (c) Case 1 at 26 weeks gestation. Coronal MR image of the uterus demonstrates membranes and fluid enveloping a lower leg, ankle and foot (black arrow points to the heel). (d) Case 1 at 36 weeks gestation. Transverse US image of the lesion (calipers) demonstrates mixed cystic and solid areas; the bones were no longer well seen.
Repeat fetal MRI at 36 weeks gestation served as the definitive anatomic study for preoperative planning and showed stable diameter of the broad-based sacrococcygeal mass with multiple septations and minimal vascularity. A large portion of the previously seen external component of the mass with contained bony structures was no longer present (Fig. 1d). The internal pelvic component of the mass remained. The family received additional information about the anticipated surgical plan, expectations for NICU care, long-term prognosis, and follow-up. The patient was monitored weekly through the remainder of the pregnancy for potential complications such as fetal hydrops and maternal mirror syndrome. Of note, fetal echocardiogram demonstrated normal cardiac structure and cardiac output.
The infant was delivered at 38 5/7 weeks gestation by scheduled cesarean section to avoid disruption of the remaining mass. At delivery, a broad based exophytic mass was visualized. This was covered by a thin translucent membrane with a thicker membrane at the edge of the mass (Fig. 2a). Free-floating skin-covered parts resembling a lower extremity were also evacuated from the uterine cavity at delivery. Apgar scores were 8 and 9. The infant, placenta, and additional fetal tissue were transported to our hospital for further evaluation and management.
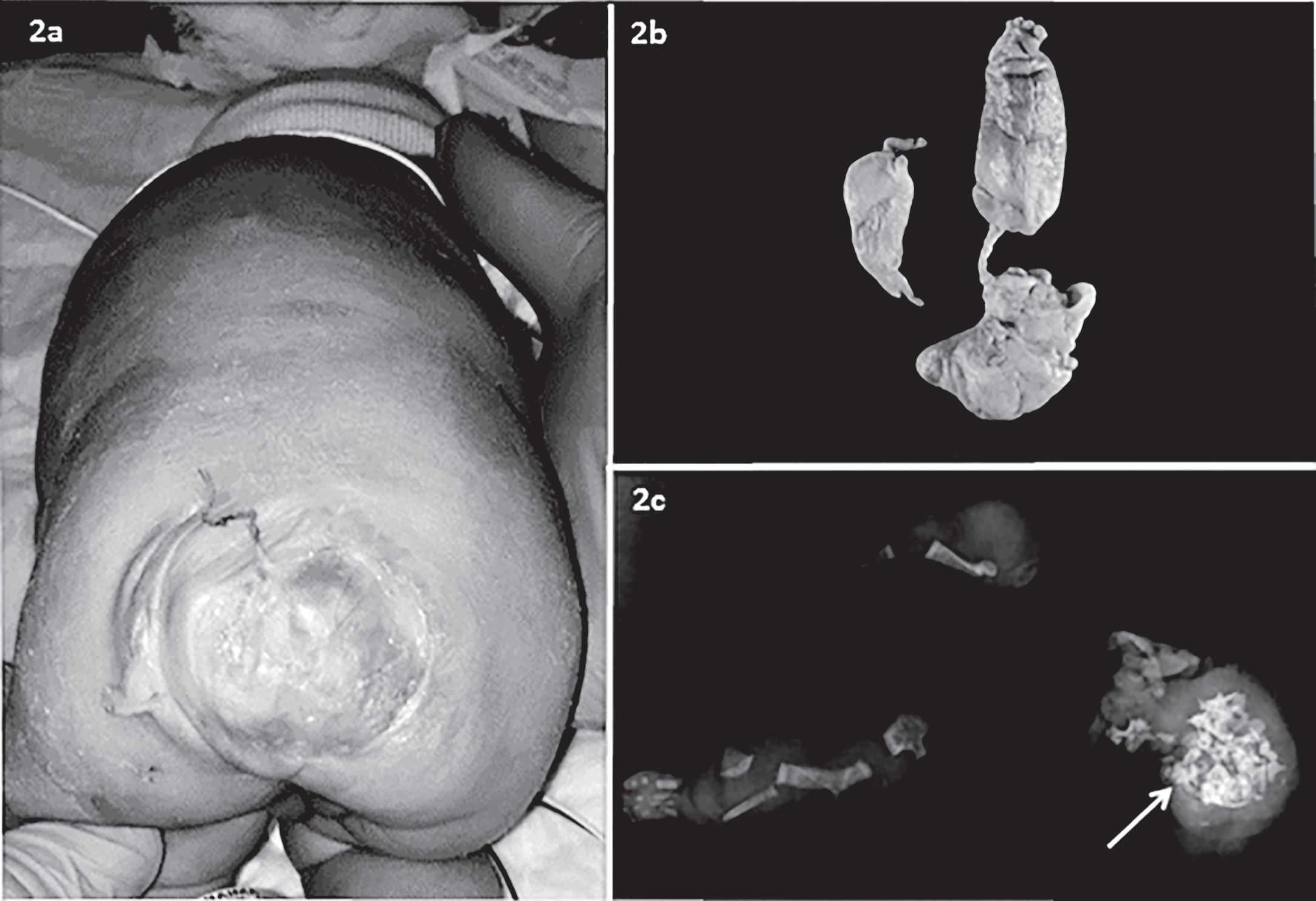
(a) Case 1 at day of life 0. Exophytic sacral mass located approximately 1 cm off midline measuring approximately 5.5 cm×4 cm, covered by a thin translucent ruptured outer membrane. (b) Macerated skin-covered free-floating mass measuring 12.5×5×1 cm evacuated from the uterus at delivery of Case 1 (lower extremity 7 cm, foot 1.5 cm). (c) Radiograph of the pathology specimen evacuated from the uterine cavity of Case 1 demonstrates structures identifiable as lower extremities, including a left foot and phalanges. Jumbled vertebra are seen in the truncal portion of the specimen (arrow).
No postnatal imaging was obtained prior to surgery due to the detailed late gestation prenatal studies. On day 2, the infant underwent complete resection of the sacral mass en bloc with the coccyx to eliminate the risk of further disruption of the mass. Postoperative recovery was complicated by a wound infection and dehiscence, treated with antibiotics and a wound vacuum dressing. Transient postoperative renal injury occurred in the setting of urinary retention, a known complication from mass effect that had been discussed with the family during prenatal counseling. Kidney function improved with temporary intermittent catheterization, and normal bladder function without catheterization was achieved by three months of age.
Placental pathology was unremarkable. The free-floating tissue evacuated from the uterus at delivery showed severely macerated skin covering a grossly recognizable 7 cm left lower extremity (Fig. 2b). Radiography revealed bones of the left lower extremity, as well as a distorted skull and vertebral bodies (Fig. 2c). Pathological examination of the excised mass showed a mixed cystic and solid mass composed of disorganized, mature gastrointestinal, pancreatic, salivary glands, neuronal and glial, cartilaginous, respiratory epithelium, smooth and striated muscle, and adipose tissue.
A 27-year-old primagravida carrying a male fetus with an intra-abdominal mass seen by prenatal US at 29 weeks delivered at 40 4/7 weeks gestation via cesarean section for failed induction and non-reassuring fetal heart tracing (Fig. 3a). The patient had been followed closely by a Maternal-Fetal Medicine specialist and was not referred for further evaluation until after delivery, as no signs of fetal hydrops or abnormal growth were present. Apgar scores were 8 and 9. Physical examination was normal except for a right lower quadrant abdominal mass felt on deep palpation. Abdominal x-ray and US on day of life 0 demonstrated a calcified mass (Fig. 3b, c). An MRI requiring sedation was obtained on day 1 and revealed a large right-sided retroperitoneal mass measuring 5.2 cm×4 cm×3.8 cm adjacent to, but separate from, the kidney (Fig. 3d). Cardiac echocardiogram revealed a small mid-muscular ventricular septal defect with left to right shunt, a patent foramen ovale, and physiological pulmonary artery branch stenosis, with otherwise normal function. The infant was sent to our hospital on day 3 for further evaluation and management.

(a) Case 2 at 28 weeks gestation. Prenatal transverse US image of the abdomen demonstrating right flank mass (arrow) characterized by mixed cystic and solid areas, scattered dense echogenic foci, and no appreciable vascularity. (b) Case 2 at day of life 0. Abdomen radiograph is notable for scattered hyperdense structures in the mid right abdomen (arrows) corresponding to the bones within the mass noted later by pathology. (c) Case 2 at day of life 0. Sagittal US image of the right mid abdominal mass (white arrows) reveals the complex nature of the fluid and several densely calcified foci located centrally (black arrow), consistent with the organized bony structures noted by pathology. (d) Case 2 at day of life 1. Axial T2 weighted MR image of the abdomen demonstrates a round, predominantly cystic mass in the right abdomen (arrow) with an internal complex soft tissue component. (e) Case 2: Surgically resected skin covered mass measuring 4.3×4.0×4.0 cm with partial membranous capsular sac, fine brown hair, and foot-like appendages (arrows).
Given the broad differential and lack of longitudinal MRI information, tumor markers were obtained. While serum β-human chorionic gonadotropin level was within normal limits, serum alpha fetoprotein (AFP) level was elevated at 37,444 IU/ml. On day 4, the infant underwent resection of the mass for definitive diagnosis. The mass was free-floating in the abdomen except for a vascular stalk connected to the retroperitoneum. Clearly identifiable fetal parts including a foot were visualized within the mass. Postoperative recovery was uncomplicated, serum AFP decreased, and the infant was discharged home two days after surgery.
Pathology demonstrated an encapsulated mass measuring 4.4×4.1×4.1 cm with a stalk containing a single vessel. Underlying the membranous capsular sac was a 4.3×4.0×4.0 cm tan, skin-covered mass covered with fine brown hair with two foot-like appendages attached, the largest of which bore toes with possible toenails (Fig. 3e). The remainder of the specimen was composed of bone (including vertebral bodies), cartilage, gastrointestinal structures, testicular tissue, neuro-glial tissue, and adipose tissue.
FIF, an extremely rare condition (1 in 500,000 live births) first defined in the 1800s, describes an encapsulated, highly differentiated fetiform mass incorporated into the body of its host [1]. As there are less than 200 cases published in the literature to date [2, 3], it is unusual that we had two cases present to our NICU in the span of 6 months. Approximately 90% of FIF cases are diagnosed in children less than 18 months [4–6]. FIF most commonly presents as a retroperitoneal mass (>70%). However, as seen in one of our patients, FIF masses can be located in other sites, such as the cranium, oropharynx, mediastinum, thorax, scrotum, ovary, testis, and sacrum [2, 7]. Vertebral columns and limbs (especially lower extremity) are present in the majority of cases, but other organs including components of the central nervous system, gastrointestinal tract, vessels, and genitourinary tract can also be seen [4, 6].
The definition of FIF, and its overlap with a teratoma, continue to be debated. Historically, FIF was thought to be a well-differentiated mature teratoma [1–3]. However, today the most widely accepted description of FIF is that of a monochorionic diamniotic twin that is incorporated into the body of its partner [1–3]. The theory is that the FIF forms from the unequal division of the blastocyst and is part of the parasitic twin continuum that also includes conjoined twins [2, 3]. However, this mechanism does not account for all reported cases of FIF, such as when there are multiple fetuses with a single host [2]. For such cases, Ji et al. offers an alternative mechanism, suggesting that very early splitting of the zygote could allow for dichorionic, diamniotic twining with the parasitic twin implanting on or being encompassed by the other twin, rather than implanting in the uterine wall [2].
The diagnostic criteria for FIF and its differentiation from a teratoma have also evolved over time. FIF and teratomas share many features, including location and a history of multiple gestations [7]. There are even case reports of FIF and teratoma both presenting in the same individual [3]. While Willis proposed in 1935 that the diagnosis of FIF requires the presence of an axial skeleton, Gonzalez-Crussi proposed a more liberal definition of FIF which requires highly developed organogenesis organized around a vertical axis [1, 6–8]. The lack of a spinal column on diagnosis does not preclude the possibility that one existed at a previous stage of development that allowed for the presence of neural cells in other organs [7]. Spencer later proposed that FIF requires at least one of the following characteristics: (1) is enclosed within a distinct sac, (2) is partially or completely covered by normal skin, (3) has grossly recognizable anatomic parts, (4) is attached to the host by only a few blood vessels, and (5) is located in a known site of conjoined twinning [9]. Both of our cases meet all FIF diagnostic criteria.
Historically, most cases of FIF were diagnosed postoperatively following identification of a calcified abdominal mass on US or radiograph [10]. The first prenatal diagnosis of FIF was reported in 1983 [11], but even with technological improvements, prenatal US diagnosis of FIF remains a challenge due to nonspecific appearance of a cystic and solid mass [10, 12]. While FIF should be suspected on prenatal imaging when an anencephalic, acardiac well-encapsulated cystic mass with calcified components is seen, differentiating it prenatally from a teratoma, meconium pseudocyst, and neuroblastoma can be difficult [5]. Fetal MRI is making prenatal diagnosis of FIF more feasible [10, 14].
In both of our cases, fetal masses were initially identified on routine prenatal US. In case 1, fetal MRI helped narrow the differential diagnosis; in case 2, the differential diagnosis based on US remained broad at the time of delivery. In particular, differentiating between teratoma and FIF prenatally may change postnatal management, reducing additional imaging and laboratory tests, potentially altering the timing of excision, and allowing for multiple opportunities to prepare families for anticipated complications. In contrast to the malignant potential of teratomas, the vast majority of FIF are benign [15]. As in both of our cases, early surgery may still be required due to mass effect, risk from mass rupture, or diagnostic uncertainty [3, 16].
Case 1 had a unique feature of partial mass rupture prior to delivery. The apparent “regression” of the previously seen external component of the mass on repeat fetal MRI in the third trimester was, in retrospect, documentation of this in-utero event. Recognition of this phenomenon, and the ability to detect it by serial fetal imaging, is important to delivering obstetricians who must be aware of the possibility of retained fetal tissue, which can increase the risk for maternal infection and hemorrhage.
In addition to using prenatal imaging of fetal masses for diagnosis, repeat MRI during the third trimester can optimize surgical planning by clearly delineating the size and location of the mass and its proximity to other organs, as illustrated in case 1 [10]. Lack of late fetal imaging may subject the newborn to anesthetic and contrast agent risks, as in case 2, even if a prenatal mass is noted [11, 13].
Finally, multi-disciplinary collaborative care in a fetal center enhanced communication between providers and with the family, and afforded coordinated expertise for this rare condition. This included specific prenatal monitoring for potential pre- and postnatal complications, such as mass expansion leading to compression of surrounding tissues and organs which can lead to abdominal distension, intestinal obstruction, jaundice, respiratory distress, and hydronephrosis [6, 17]. Increased risk of hydrops fetalis due to mass vascularity may present urgently and prenatal evaluation by pediatric specialists can facilitate the diagnosis and care of this event for both the mother and receiving NICU. Multidisciplinary prenatal counseling and early introduction of the family to the newborn’s care team in case 1 allowed for continuity and managed expectations, facilitating the family’s understanding of complex surgical plans and consent processes.
As these cases highlight, management differed when evaluation was arranged through a fetal medicine program compared to a postnatal referral. A coordinated, multi-disciplinary approach can optimize patient care by providing the opportunity for delivery and surgical planning, detailed anticipatory counseling, and streamlined postnatal management.
Disclosure statements
The authors have no financial disclosures or conflicts of interest to declare. The IRB of our institution determined that this did not meet the definition of human subject’s research and thus IRB review and approval was not necessary.
Footnotes
Acknowledgments
We would like to thank Dr. Mikael Petrosyan of Children’s National Health System and Dr. Eric Jelin of Johns Hopkins University Hospital for their contributions to the surgical management of these patients.