
Abstract
OBJECTIVES:
The aim was to achieve 100% effective handover from the critical care transport team to the neonatal intensive care unit (NICU) medical team.
STUDY DESIGN:
All patients transferred from referring hospitals by the critical care transport team to the Level IV NICU were included. Data for each infant was collected prospectively. The percentage of transported patients for which medical team and nursing handover occurred was recorded. A quality improvement project was launched using the Plan-Do-Study-Act (PDSA) tool. We implemented several processes including call from the transport team before arrival and the completion of a transfer of care form on arrival to the NICU. The process measures and the outcome measure of completion of handover were monitored. Run charts of process measures and the outcome measure were analyzed.
RESULTS:
Completion of medical handover increased from 95% (baseline) to 100% after 3 PDSA cycles and this has been maintained for 18 consecutive months.
CONCLUSION:
Medical handover from the critical care transport team to the NICU medical staff has been achieved and sustained for all neonatal transports.
Introduction
Patient handovers are defined as the transfer of information, professional responsibility and accountability between individuals and teams that can occur in three different situations: i) handover that occurs between shifts; ii) handover that occurs with transfer of services within a hospital; or iii) handover that occurs between two institutions, as occurs in external transports of patients [1]. The purpose of an accurate handover is to communicate patient information and enable continuity of care. Inaccuracies or omissions during handover communications are the most prevalent causes leading to delays in medical care, medical errors and adverse outcomes, all of which jeopardize patient safety [1, 2]. Therefore, accuracy and efficiency of handovers are vital to ensure safe and reliable transition in care for patients and reduce adverse outcomes. The Joint Commission on Accreditation of Health Care Organizations has identified patient care handover as an important patient safety goal for all health care organizations [3].
There have been a number of tools developed recently to improve the quality of handover for pediatric patients [4–8], perioperative patients [9–12] and patients transported to emergency departments [13, 14]. These tools use various mnemonics and checklists to improve the quality and accuracy of handover, with the goal of decreasing complications related to inefficient handover [7, 14–16]. Handover accuracy in pediatric patients in children’s hospitals has improved using standardized approaches, which have reduced medical errors and adverse events as well as the number of interruptions during handoffs [5, 8].
There are a number of tools used in quality improvement methodology, such as the value compass [17], process maps, cause-and-effect diagrams (also called fishbone or Ishikawa diagrams), and plan-do-study-act (PDSA) cycles [18]. PDSA cycles are an iterative procedure that uses the scientific method for rapid tests of change aimed at improving a clinical process or outcome. It is an action-oriented way to learn by planning a change aimed at testing a hypothesis, then implementing that test, observing the results and analyzing the data to act on what is learned. The cycle then generates another PDSA cycle and so on.
There are no reports that have studied whether the handover process after neonatal transport routinely occurs and how handover completion between nursing staff and medical staff compares. The purpose of this quality improvement project was to assess whether handover between a critical care transport team and the neonatal staff in the neonatal intensive care unit (NICU) was consistently occurring after several potentially better improvements in this process. The initial objective was to collect data to identify and develop process changes needed to enhance handover from the critical care transport team to the NICU medical team on arrival. The subsequent objectives were to implement and test the process changes. The ultimate goal of this quality improvement project was to achieve 100% effective handover from the critical care transport team to the NICU medical team.
Methods
Setting
All patients transferred by the Penn State Health Life Lion Critical Care Transport team from referring hospitals to the Level IV Penn State Health Children’s Hospital NICU were included. The Penn State Health Life Lion Critical Care Transport team consists of a group of certified flight registered nurses and certified flight paramedics who treat and transport patients of all ages by helicopter and ground critical care ambulance. An average of 195 neonates are transported by this program per year. The Penn State Health Children’s Hospital NICU is a regional quaternary NICU with outborn infants accounting for 40% of annual admissions.
Data for each outborn infant is collected prospectively using a score card linked to the electronic medical record in the admission note from the attending neonatologist. The score card includes 10 quality indicators, including whether bedside report (handover) is given by the critical care transport team to the receiving medical team and nursing staff. Score cards are reviewed monthly and the percentage of transported patients for which medical team and nursing handover occurred is recorded. The initial baseline data collection indicated that medical handover was not occurring 100% of the time. This collection of data was used to develop a change.
A multi-disciplinary team, consisting of a neonatologist, an emergency physician, and nursing from both the NICU and the critical care transport team, analyzed these baseline data and developed potentially better practices that were tested. Four subsequent Plan-Do-Study-Act (PDSA) cycles were aimed at testing and implementing these process changes with the goal to increase the percentage of medical handovers to 100%. The first change, implemented in August 2012 was that when the medical team was unable to meet the transport team due to unavailability as a result of being involved in the care of another patient or presence in the delivery room, it was the responsibility of the medical team to call the transport team’s communication center and speak with the transport team leader to obtain handover information via phone. When this did not increase the percentage of handovers to 100%, a subsequent PDSA cycle was instituted in April 2013 with a three-component process that included the following: 1) the transport team’s communication center was instructed to call the NICU charge nurse when the team was approximately 10 minutes from arrival; 2) the charge nurse would then notify the medical team to meet the transport team on arrival; 3) if the medical team was called away from the NICU near the time of the arrival, the NICU medical team would call the transport team leader to obtain handover information by phone. In July 2013, a third PDSA cycle was implemented to track performance of the calls made 10 minutes prior to arrival. The fourth PDSA cycle was implemented in order to provide a checklist using a transfer of care form developed and implemented by the critical care transport team in July 2015.
We measured the compliance of the processes during each of the PDSA cycles. Specifically, we measured the number of times that phone calls were not made from the medical team in the NICU to the Life Lion team if they were unable to be met on arrival to the NICU. We also measured the compliance with the 10 minute estimated time of arrival (ETA) call to the charge nurse and we measured the process of completing the transfer of care form. The outcome measure was the percentage of handovers between the transport team and the medical staff that were successfully completed.
This was a quality improvement project, and as such was exempted from the Institutional Review Board approval.
Results
Baseline data revealed that medical handover occurred for 95% ±6% (mean±SD) of transports during the baseline period as shown in Fig. 1. This increased to 97% ±4% after the first process change (PDSA Cycle 1, Fig. 1). After the second and third process changes the handover occurred for 99% ±3% of transports (PDSA Cycles 2 and 3, Fig. 1), and handover has been completed for 100% of all transports during PDSA Cycle 4. As depicted in the run chart (Fig. 2), we achieved 100% completion of medical handovers cycle beginning in January 2015 during PDSA cycle 3. The decreased SD seen during the baseline period through PDSA cycle 4 in Fig. 1 indicates a decrease in the variability in the handover, which is also seen in the run chart (Fig. 2). Transfer of care forms were implemented in July 2015 (PDSA cycle 4) to maintain 100% handover being achieved to the present time. The run chart also shows that the goal for 100% medical handover completion has been reached.
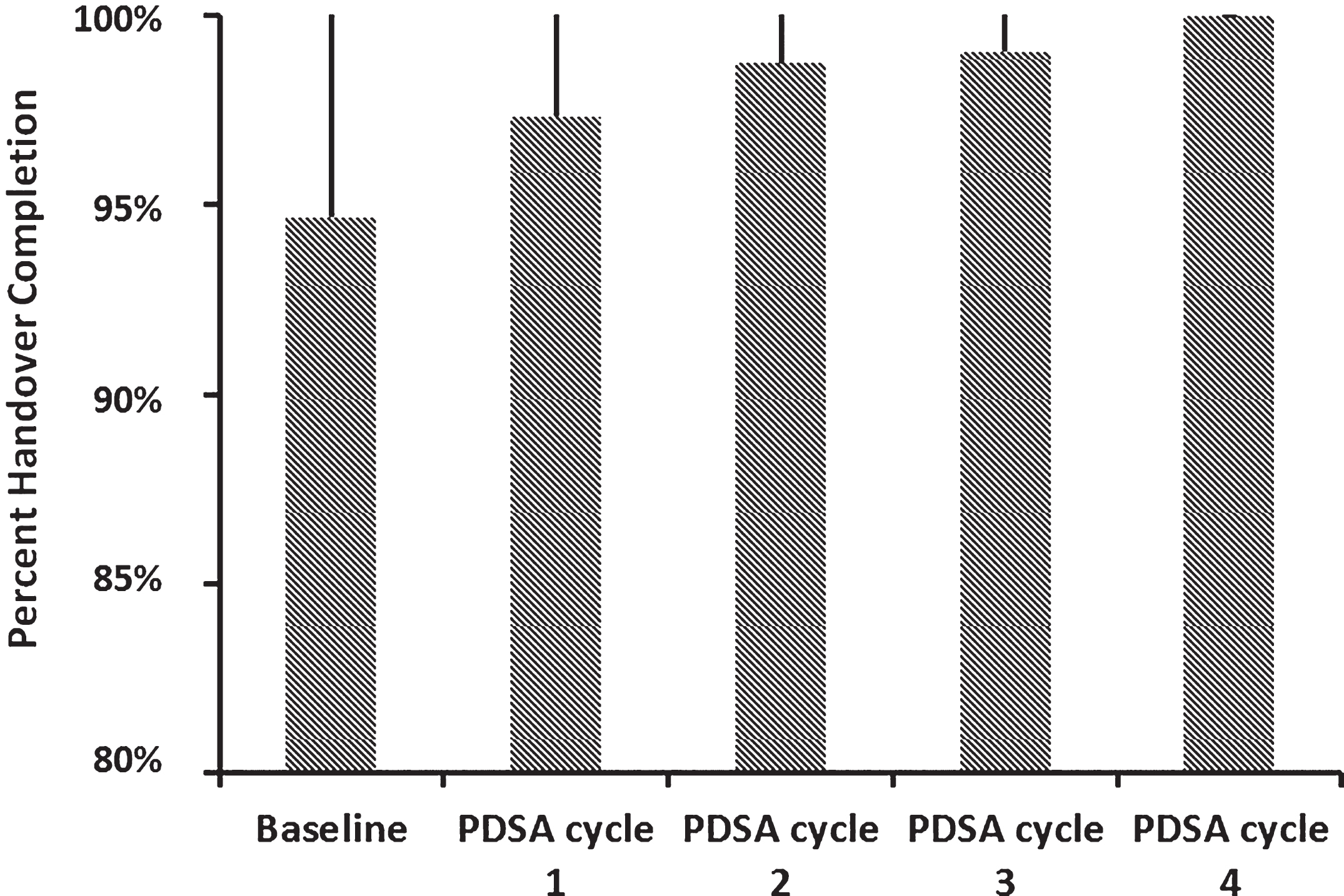
Medical handover completion during the baseline period and subsequent four PDSA cycles. There was an increase in the percentage of transported patients for whom medical handover was completed, and there was a decrease in the variability of handover completion. Data represent the mean±standard deviation (SD).

Run chart of medical (MD handover) and nursing handover completion (percentage of transported patients) for each month from 2012 through December 2016. Handover for all transported patients has been achieved since January 2015. Each PDSA cycle is indicated by the solid arrows, and reinforcing staff education is annotated by the dashed arrows. Medical handover completion is depicted by the diamonds, and nursing handover is shown by the circles.
Nurse handover from the Critical Care Transport Team had historically been completed on all transported infants. Figure 2 also shows a comparison of the medical and nursing handover completions.
The process improvements that were implemented (10 minute ETA call, completion of transfer of care forms) were monitored. Figure 3 is a run chart showing the increase in percentage of transported patients where a 10 minute ETA call was made and in which a transfer of care form was completed. While there is still variability in these processes, we have not seen a decrease in the outcome measure of medical handover completion.

Run chart showing completion of the processes implemented to improve the outcome measure of medical handover. Calls from the EMS Transport Communication Center with a 10 minute estimated time of arrival (ETA call) began in July 2013 and showed a significant increase (diamonds). The implementation of a transfer of care form began in July 2015 and showed an increase in completion with much variability (squares).
Outcomes have improved with several errors and admission assessments occurring prior to PDSA Cycle 2 and no errors in admission assessments after the last 2 PDSA cycles.
This study is the first to report improved handover communication for neonatal transports using pragmatic quality improvement tools. We have shown that completion of handover between the critical care transport team and the medical staff in the NICU can be achieved with 100% compliance rate. Complete and accurate transport handover communication in transports is vital to ensure safe and reliable transition in care for these patients. While handover of information from the critical care transport team to the NICU nursing staff had been occurring for all transports, we believe that handover to the medical team is crucial so that first-hand information about the patient and the smooth transfer of responsibility can occur at all levels of patient care. This concept is supported by studies of perioperative handover from the operating room to the intensive care unit [2, 12]. We have shown that the discrepancy between handover completion to nursing and to medical staff can be eliminated. There are no published studies of which we are aware that have addressed this comparison between nursing and medical handover during neonatal transport. One study addressed differences in communication, specifically interactive questioning, during handover based on level of training and between disciplines (nursing staff, medical staff, nurse practitioners) and found that less experienced clinicians had more interjections and fewer clarifying questions as well as collaborative questioning of the accuracy of information during the handover process compared with more experienced clinicians [19]. Physicians stated more action critiques (statements that an inappropriate action had been performed) than nurses during handover [19].
In addition, we have shown how improved communication between teams can occur through the use of a 10 minute estimated time of arrival call from the transport team and the completion of a transfer of care form on arrival to the NICU, both of which have contributed to the improvement in the outcome measure of completion of medical handover. There is only one previous article studying communication in handover in a pediatric transport service [20]. This study revealed that process mapping, which resulted in a standardized system for notification of the physician of patient arrival, and scripting a transport handover would improve communication during handover [20]. In addition, they found that overall staff satisfaction improved with a revised handover process [20]. That paper did not report, however, on the actual completion of handover occurring between the medical transport and medical team in the NICU.
Much of the literature related to handovers address the issues of handover from surgery to intensive care both in the adult and pediatric populations [9–12]. Many factors contribute to inaccurate handover including human factors (interruptions, distractions, fatigue) and poor communication due to stress, haste and inattention and underlying relationships between health care providers [21, 22]. While reducing work hours may decrease stress and fatigue, this has the unintended consequence (balance measure) of increasing the number of handovers and hence potentially increasing risk to patients. Addressing these factors to improve handover communication has been the subject of much research. Strategies include creating an environment where individuals involved in handover feel safe to participate and question, standardization of the process using simple processes and tools (mnemonics, checklists), avoiding interruptions during handovers, direct communication without the use of intermediaries, and use of a read back process. Many of these strategies have been taught and implemented with improvements in both the handover process and the outcomes of reducing adverse events and medical errors [2, 15]. Using similar strategies have improved handover between paramedics and emergency department staff [23]. Delay in handover from emergency medical services to emergency physicians can result in adverse outcomes as well as keeping first line responders from their service in the community. Handover delays were found to be relatively common in Australia, being most prevalent in large urban hospitals in winter [24].
Limitations of our study are that we did not routinely monitor the duration of handovers or any interruptions to the handover process. In addition, we did not systematically monitor adverse events related to handover incompletion early in the process. We did, however, use convenience sampling to assess inaccuracy of information and effect on adverse events and showed a decrease in those events after the most recent 2 PDSA cycles.
In the pediatric literature, much of the information has focused on handover tools and reduction of errors in pediatric patients during shift change handovers. This is the first report of medical completion of handover communication for neonatal transports. We conclude that implementing very simple and effective methods as outlined in this report resulted in 100% effective transfer of information between a NICU critical care transport team and NICU medical staff. Future efforts will be directed at assessing the duration of handovers, interruptions of the process as well as accuracy and completeness of the process.
Disclosures
The authors have no conflicts of interest to disclose. This was a quality improvement project, and as such was exempted from Institutional Review Board approval.
Footnotes
Acknowledgments
The authors thank the staff of the neonatal intensive care unit and the staff of the Life Lion Critical Care Team for their commitment to provide the safest and highest quality of care to the infants transported to the Penn State Health Children’s Hospital.