
Abstract
OBJECTIVE:
To compare demographic data, prenatal and postnatal characteristics, laboratory data, and outcomes in a cohort of premature infants with spontaneous ileal perforation (SIP), surgical necrotizing enterocolitis (sNEC) and matched controls.
METHODS:
A retrospective case–control study of infants with intestinal perforation with a birth weight (BW) less than 2,000 grams and gestational age (GA) less than 34 weeks and infants without perforation matched for BW (±150 grams) and GA (±1week).
RESULTS:
130 premature infants were included, 30 infants with SIP, 35 infants with sNEC and 65 control infants. The median age of onset was 5 days postnatal age in SIP versus 25 days in sNEC (p < 0.001) and the peak onset was at 26 weeks corrected GA for SIP and 30 weeks corrected GA for sNEC. Infants with perforation had significantly higher rates of mortality (p < 0.001) and common morbidities associated with prematurity. Administration of corticosteroids and indomethacin did not differ among groups. SIP was more common among infants born to young mothers (p = 0.04) and less common in infants receiving caffeine (p = 0.02). sNEC was less common among infants receiving early red cell transfusion (p = 0.01). Perforation and sNEC trended towards less common in infants receiving inhaled nitric oxide.
CONCLUSION:
SIP and sNEC are distinct clinical entities. Potential protective effects of caffeine, inhaled nitric oxide, and early transfusion should be further studied.
Keywords
Abbreviations:
gestational age
birth weight
spontaneous intestinal perforation
necrotizing enterocolitis
surgical NEC
inter-quartile range
patent ductus arteriosus
bronchopulmonary dysplasia
retinopathy of prematurity
intraventricular hemorrhage
periventricular leukomalacia
C-reactive protein
parenteral nutrition
extremely low birth weight
Introduction
Intestinal perforation is a common and potentially catastrophic complication of very preterm birth. The two major causes of intestinal perforation in premature infants are spontaneous intestinal perforation (SIP, also known as focal or isolated intestinal perforation) and surgical necrotizing enterocolitis (sNEC), with meconium-related ileus [1] and intestinal candidiasis [2, 3] much less common. Distinguishing between these two clinical entities can be challenging. Both are associated with significant morbidity and mortality [4]. Early reports defined SIP as intestinal perforation without pneumatosis intestinalis on abdominal radiograph and sNEC as intestinal perforation with pneumatosis [5, 6]. The primary features that suggest SIP as a different disease process from sNEC include 1) timing of onset (SIP can occur in utero and is mostly seen in the first 1–2 weeks of life, often prior to starting enteral feedings, while necrotizing enterocolitis occurs later with a peak at 30–32 weeks corrected gestational age [7]), 2) clinical presentation (most infants with SIP present with abdominal distention, discoloration of the abdominal skin and either a gasless abdomen or pneumoperitoneum on abdominal X-ray, without prior signs of systemic illness while NEC often presents with episodes of apnea and bradycardia, feeding intolerance, bloody stools as well as abdominal distention and either pneumatosis intestinalis, portal venous air or pneumoperitoneum on abdominal X-ray [8]), 3) histopathology (SIP is characterized by an isolated perforation without surrounding necrosis or neutrophil infiltrate, often accompanied by a focal thinning or absence of the intestinal muscularis propria [9, 10] whereas the characteristic finding in sNEC is inflammation and extensive coagulation necrosis often with evidence of ischemia [8], 4) the role of the intestinal microbiota (this community of microbes appears to play a significant role in the pathogenesis of NEC but not SIP, evidence includes a protective benefit from human milk and probiotics, increased risk with antibiotics, acid-blocking agents, and direct microbial evidence [11] for NEC but not for SIP), and 5) differences in cytokine [12], gene [13] and miRNA expression [14] suggesting marked differences in mechanisms underlying pathogenesis.
SIP and NEC share several common features including an inverse relationship with gestational age (the most premature infants are at highest risk for both diseases), an association with acute chorioamnionitis and placental vasculitis [15] and an increased risk of neurodevelopmental delays [4] and abnormalities on brain MRI scanning [16]. The modified Bell’s classification for NEC remains a useful system with intestinal perforation one of the key distinguishing features between stage 2 and stage 3 NEC (in this paper, we will focus only on NEC with perforation or sNEC). This system does not include SIP as a separate entity distinct from stage 3 NEC prompting a proposed modified classification scheme [17].
The aims of our study were to compare demographic data, prenatal and postnatal characteristics, laboratory data, and outcomes in a cohort of premature infants with and without intestinal perforation.
Materials and methods
This is a retrospective case–control study to identify factors associated with intestinal perforation in premature infants and that distinguish SIP from sNEC. Approval was obtained from the University of California Davis institutional review board. Infants were identified from the database of the University of California, Davis Children’s Hospital that was searched for a diagnosis of sNEC, perinatal intestinal perforation or intestinal perforation with a BW less than 2,000 grams and GA less than 34 weeks born between January 1, 2005 and October 31, 2014. Infants with major congenital anomalies, complex congenital heart disease, and congenital intestinal malformations were excluded. For each infant with intestinal perforation, one infant without SIP or NEC was selected. The control infants were matched with the infants with perforation based on birth weight (BW) ±150 grams and gestational age (GA) ±1week. We divided the infants into four overlapping groups: infants with perforation (SIP and sNEC, n = 65), SIP (n = 30), sNEC (n = 35) and controls (n = 65). The demographic data, prenatal and postnatal characteristics, laboratory, surgical interventions, morbidities and mortality were compared. SIP infants were distinguished from sNEC infants based on the intra-operative surgical report and/or histopathology report.
Definitions
Prenatal steroid treatment was defined as at least two doses. Patent ductus arteriosus (PDA) was diagnosed by echocardiogram. Surfactant treatment was defined as one or more doses. Caffeine treatment was defined as one or more doses of either intravenous or oral caffeine citrate (our usual approach is a loading dose of 20 mg/kg followed by 5–10 mg/kg once daily with transition from intravenous to oral dosing when the infant is tolerating 100 ml/kg/d of enteral feeding). Inhaled nitric oxide therapy was defined as any administration of inhaled nitric oxide (NO, our usual approach is to initiate treatment at 20 ppm for premature infants with hypoxic respiratory failure and evidence of pulmonary hypertension on echocardiography). Early onset sepsis was defined as a positive blood culture in the first 3 days of life. Empiric antibiotic therapy was initiated in the first hours of life and was classified into 2 categories:≤3 days or 4–7 days. Indomethacin prophylaxis was defined as administration within the first 24 hours after birth. Bronchopulmonary dysplasia (BPD) was defined as requirement for oxygen at 36 weeks corrected GA. Retinopathy of prematurity (ROP) was diagnosed according to the international classification. Severity of intraventricular hemorrhage (IVH) was based on the criteria of Papile. Periventricular leukomalacia (PVL) was diagnosed by ultrasound or MRI after 21 days of age. Late onset sepsis was defined as a positive culture from blood, endotracheal aspirate, cerebrospinal fluid or urine after 3 days of life that was not deemed a contaminant. Cholestasis was included if the infant received ursodiol.
Statistical analysis
Data were analyzed by using SPSS version 17.0 (Chicago, Illinois, United States). Normally distributed continuous data were expressed as mean±standard deviation and differences between groups were tested by the t-test. Continuous data which were not normally distributed were expressed as median and inter-quartile range (IQR 25–75) and tested by the rank test for differences between groups. Categorical data were analyzed with the Chi-square or Fisher exact test. Statistical significance was set at p < 0.05.
Results
A total of 130 infants were included. 30 infants developed SIP, 35 infants developed sNEC and 65 matched infants had neither SIP nor NEC. Prenatal and postnatal characteristics are shown in Table 1. Prenatal diagnoses and prenatal medical treatment were mostly similar between SIP infants and sNEC infants. However, compared with the control group, infants with perforation were more likely to have younger mothers (RR 1.5, 95% confidence interval 1.1–2.1) and less likely to have mothers with chronic hypertension (RR 0.26, 95% confidence interval 0.072–0.96) with young maternal age remaining statistically significant when comparing SIP infants to controls (RR 2.0, 95% confidence intervals 1.1–3.5). Among postnatal characteristics GA, BW, sex and Apgar scores were similar among groups. As expected there were more outborn infants in the perforation group (both SIP and sNEC) since many of these infants were transferred for surgical evaluation. Markers of acuity of illness in the first days of life (e.g. early onset sepsis, day of first enteral feeding, and administration of surfactant or inotropic medications) did not differ between the control and perforation groups. Administration of inhaled nitric oxide (NO) trended towards being more common in the control group than the perforation group (RR 0.37, 95% confidence interval 0.13–1.04) or the sNEC group (RR 0.096, 95% confidence interval 0.0063–1.5). Early red blood cell transfusion was least common in the sNEC group (RR versus control = 0.43, 95% confidence intervals 0.23 –0.81). Among common treatments of very premature infants initial antibiotic days, indomethacin, corticosteroids, rectal glycerin, and antifungal prophylaxis did not differ between infants with and without perforation, while caffeine administration was less common among infants with perforation (particularly the SIP group, RR versus control = 0.48, 95% confidence intervals 0.28 –0.84). Eight of 30 infants with SIP and three of 35 infants with sNEC had not received enteral feeding before the onset of perforation.
Prenatal and postnatal characteristics
Prenatal and postnatal characteristics
a: mean (sd). b: median (IQR 25–75).
The distribution of infants according to GA at birth and corrected GA at the time of diagnosis of SIP and sNEC are shown in Fig. 1. As expected, SIP infants were younger and weighed less at the time of diagnosis than sNEC infants with the peak onset of SIP at 26 weeks corrected GA and the peak onset of sNEC at 30 weeks corrected GA. Clinical and surgical differences between SIP and sNEC infants are summarized in Table 2. All SIP infants received laparotomy, 77% had ileal involvement (33% distal ileum, 17% proximal ileum and 27% distal vs proximal ileum not stated). Among sNEC infants who underwent laparotomy, the distal ileum was the most commonly involved area (28%).
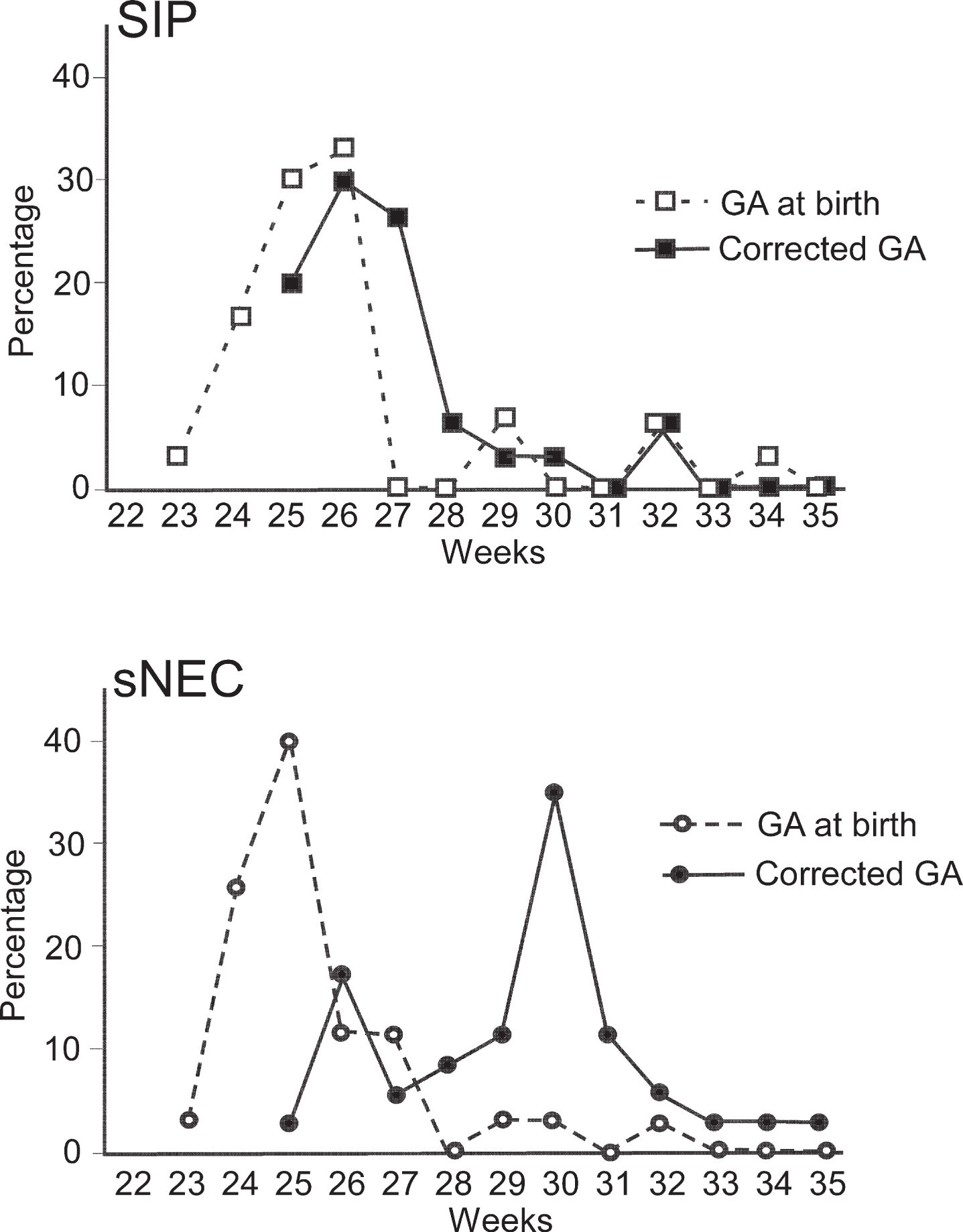
The gestational age at birth and the corrected GA at the time of diagnosis of SIP (upper panel) and sNEC (lower panel).
Clinical and surgical differences between infants with SIP and sNEC
a: mean (sd). b: median (IQR 25–75).
A comparison of common laboratory values between infants with SIP and sNEC is presented in Table 3. SIP infants were more likely to have a higher mean percentage of neutrophils and lower phosphorus on the day of diagnosis while sNEC infants were more likely to have an elevated I:T ratio and C-reactive protein (CRP) level, higher potassium and lower hemoglobin, sodium, chloride and pH. Some of these likely represent differences in corrected gestational age at the time of presentation and the inflammatory nature of sNEC. Hyponatremia has been associated with sNEC and likely represents renal involvement [18, 19].
Biochemical parameters at the time of diagnosis in SIP infants and sNEC infants
b: median (IQR 25–75).
As anticipated, mortality and morbidities (including ROP, IVH, PVL, length of PN dependence and transfusions) were significantly higher in infants with perforation. The incidence of BPD was lower in the perforation group, but this difference did not remain when assessing the composite outcome of death or BPD. The mean delta z scores for body weight and head circumference (discharge z score minus birth z score) were significantly higher in infants with perforation consistent with poorer growth (Table 4). There was no significant difference in the mortality rate between SIP infants and sNEC infants. sNEC infants had significantly longer length of hospital stay, length of PN dependence and were more likely to be require home PN than SIP infants.
Mortality and morbidities
PN: parenteral nutrition. b: median (IQR 25–75). a: 4 infants with SIP, 3 infants with sNEC and 9 control infants were transferred back to their birth hospital and therefore measurements at the time of discharge to home were unavailable.
A comparison between early and late onset of both SIP and sNEC is presented in Table 5. The supplemental table presents a summary of all positive cultures.
Comparison between early and late onset for infants with SIP or sNEC
b: median (IQR 25–75).
Intestinal perforation (whether due to SIP or sNEC) is associated with significant morbidity and mortality in premature infants. It is often possible to distinguish SIP from sNEC based on clinical presentation though definitive diagnosis generally requires surgical intervention. Historically, several factors have been associated with SIP including developmental muscular deficiency of the intestinal wall, postnatal indomethacin, postnatal steroids, and infectious agents (Candida and coagulase negative staphylococcal infection have both been implicated) [10, 21]. In contrast, the primary risk factors for NEC include enteral feeding (particularly formula feeding), intestinal dysbiosis resulting in local inflammation and increased permeability leading to bacterial translocation, and developmental vulnerability of innate intestinal defenses leading to a poorly regulated systemic inflammatory response [8]. The critical role of the intestinal microbiota in NEC pathogenesis is reinforced by clinical trials and cohort studies demonstrating a protective effect of probiotics [22].
This cohort is consistent with previous reports in several aspects. The observed higher rates of mortality and morbidity are consistent with and extend previous observations [4, 16]. Analysis of a large data set suggested two subgroups of premature infants with SIP: 1) early onset SIP (0–3 days of life) was more common in larger, less premature infants who were less likely to have received antenatal steroids or post-natal surfactant or mechanical ventilation and 2) later onset SIP (4–14 days) was more common in extremely low birth weight (ELBW) babies, many of whom had received post-natal glucocorticoids and indomethacin [20]. While the numbers are small, this cohort is consistent with this pattern (Table 5). Several studies have suggested two subgroups of premature infants with NEC: 1) early onset (presenting in the first two weeks of life, mostly in term infants) and 2) late onset (peak onset at 21–32 days of life, predominantly in premature infants) [23, 24]. A more recent study suggested a shift from previous studies with more premature infants with BW >1000 g presenting with NEC in the first two weeks of life and ELBW infants more likely to present at a corrected gestational age of 30–32 weeks [7]. Many of these studies did not distinguish NEC from SIP. In our study, infants with sNEC presenting in the first one or two weeks of life tended to be less premature and less likely to have received antenatal steroids than those with later onset of sNEC (Table 5).
Novel observations from this cohort include the lower percentage of SIP infants receiving caffeine and the trend towards a lower percentage of perforation infants receiving inhaled NO. Associations in a cohort study cannot address causality, but are useful for generating hypotheses such as that these agents may have protective benefits. Caffeine administration was associated with increased risk of NEC in a recent large cohort study [25] and with alterations of many aspects of gastrointestinal function in a rodent mode [26]; however, no association between caffeine and NEC was noted in a multi-center cohort study [27]. Neither of the large cohort studies nor the multi-center cohort study reported the incidence of SIP in relation to caffeine administration. In experimental rat models of NEC, blockade of NO synthase decreases intestinal microcirculatory blood flow [28] and the intestinal cytoprotective agent heparin-binding EGF-like growth factor increases NO production resulting in decreased experimental NEC [29] and improved microcirculatory blood flow [30]. Alterations in growth factor physiology and abundance of NO regulate relaxation of the intestinal smooth muscle. Dysregulation of this delicate balance in favor of vasoconstriction has been noted in both animal models and in confirmed human NEC [31]. While inhaled NO has predominantly local effects, investigation of the possibility of impact of inhaled NO on intestinal circulation, the intestinal microbiota and NEC risk may be of value.
Additional novel observations from this cohort include the younger maternal age and decreased incidence of maternal chronic hypertension in infants with perforation. Maternal hypertension and maternal smoking have both been proposed as risk factors for NEC based on altered placental perfusion and ischemia leading to placental and fetal hypoxia [32], however studies to date on both of these risk factors have been mixed [33, 34]. We find no previous studies reporting alterations in risk of SIP with maternal hypertension or maternal age. A recent similar-sized cohort in Japan did not report any association between maternal factors and SIP [35].
Associations between non-steroidal anti-inflammatory agents and intestinal perforation have been mixed. Indomethacin is frequently administered to premature infants for treatment of a PDA or for prevention of intraventricular hemorrhage. Indomethacin decreases mesenteric blood flow and can cause direct mucosal injury as well as increased intestinal contractility [36]. Early reports of associations between indomethacin and SIP [20] have not been consistently confirmed [37]. A comparison of indomethacin and ibuprofen in premature infants for PDA found no differences in either SIP or NEC [38]. It is possible that non-steroidal agents only increase the risk of SIP in the presence of other factors such as a hemodynamically significant PDA [21]. Our study did not show any significant association between SIP or sNEC and indomethacin or ibuprofen use. Associations between early exposure to postnatal steroids and intestinal perforation have also been mixed [39, 40]. Our cohort did not include any infants treated with dexamethasone in the first 7 days of life and only 4 infants were exposed hydrocortisone in the first 7 days.
One strength of our study is that almost all infants with perforation underwent laparotomy so that histopathologic evaluation was frequently available. Limitations of our study include the small sample size and the retrospective study design. With a long study period of 10 years, there have been practice changes including the utilization of peritoneal drains.
In conclusion, this study confirmed an earlier age of onset of SIP than NEC and increased mortality and morbidity associated with both forms of intestinal perforation, but did not demonstrate an association between indomethacin and SIP. Novel associations include an increase in SIP among infants of young mothers, a decrease in SIP among infants receiving caffeine, a decrease in sNEC among infants receiving early red blood cell transfusion, and a decrease in intestinal perforation among infants receiving inhaled NO.
Conflicts of interest
None declared.