
Abstract
OBJECTIVES:
To compare the incidence of polycythemia in newborns of women with hypertensive disorders in pregnancy (HDP) with those of normotensive mothers, to determine the incidence of perinatal stress using Apgar scores and to correlate hematocrit with Apgar scores in these newborn.
STUDY DESIGN:
This was a hospital-based comparative study conducted in the University of Port Harcourt Teaching Hospital, Nigeria.
MAIN OUTCOME MEASURES:
Apgar scores of 200 newborns- 100 from mothers with HDP (case group) and 100 from normotensive mothers (control group)- were taken at 1st and 5th minute of birth and cord blood samples collected to determine hematocrit. The subjects were categorized into polycythemic and non polycythemic using a hematocrit ≥65%.
RESULTS:
Eight percent of newborns of women with HDP had polycythemia while none of the controls did. Apgar scores in the case group with and without polycythemia at one-minute were 4.1±1.8 and 6.6±2.1, respectively and at 5 minutes were 6.9±1.7 and 8.5±1.4 respectively. Hematocrit correlated positively with Apgar scores (both at one and five minutes) in cases without polycythemia (r = 0.221, p = 0.034 and r = 0.255, p = 0.014). Hematocrit of polycythemic newborns did not correlate with Apgar scores (r = –0.287, p = 0.491 and r = –0.436, p = 0.281).
CONCLUSION:
The incidence of polycythemia is significantly higher in newborns of women with HDP and these polycythemic neonates had a significantly higher incidence of birth asphyxia. Therefore, birth outcome as determined by Apgar score is influenced by hematocrit.
Introduction
Perinatal outcome is strongly influenced by hypertensive disorder in pregnancy (HDP) with different degrees of fetal injury irrespective of the underlying syndrome [1–3]. Hypertensive disorders in pregnancy, defined as diastolic blood pressure of at least 90 mmHg or a systolic blood pressure of at least 140 mmHg in a pregnant women taken in an interval of at least 6 hours [4], is associated with compromised uteroplacental circulation and creates an unfavorable uterine environment for the fetus due to marked imbalance in maternal homeostasis, pathophysiological changes in placenta and vascular insufficiency resulting in fetal hypoxia [5].
Increased fetal erythropoiesis is frequently seen in conditions associated with hypoxia from placental vascular insufficiency with consequent polycythemia [6–8]. By increasing blood viscosity, polycythemia can impair microcirculatory flow in end organs and can present with neurologic, cardiopulmonary, gastrointestinal, and metabolic symptoms with attendant morbidity and mortality [7, 10].
Placental and vascular insufficiency in HDP remains an important etiological factor of perinatal asphyxia, which further increases the morbidity and mortality associated with the condition [11]. Asphyxia is defined as impaired respiration with associated metabolic acidosis, it is diagnosed using non reassuring fetal heart rate patterns, prolonged labor, meconium-stained fluid, low Apgar score, and mild to moderate academia [12]. The Apgar scoring system, a very useful tool with all the shortcomings in that it does not fully define birth asphyxia, is widely used in the measurement of birth asphyxia [13–15]. A large univariate analysis from Australia revealed that women with HDP, when compared with normotensive women, had increased risk of having neonates with low Apgar scores [16]. In a study in Turkey, the majority of fetal distress and low Apgar scores occurred in babies of mothers with severe preeclampsia, a type of HDP [17].
The treatment of polycythemia and its accompanying blood viscosity can be done with partial exchange transfusion (PET) which is known to normalize hemodynamics and hence improve clinical outcome while decreasing mortality [18].
This study aims to compare the incidence of polycythemia and perinatal asphyxia using Apgar scores in newborns of women with HDP and those of normotensive mothers; to correlate hematocrit (HCT) with Apgar scores in newborns of women with HDP and normotensive mothers. It is expected that the findings of this study will highlight the perinatal morbidity associated with HDP and help stimulate measures to improve the outcome of pregnancy in women with HDP. This will contribute significantly towards achieving the sustainable development goal on reducing neonatal mortality.
Patients and methods
Study design and source
This was a hospital-based comparative cross-sectional study conducted in University of Port Harcourt Teaching Hospital (UPTH) a tertiary hospital in south-south Nigeria.
Study population
Two hundred study participants including 100 newborns delivered to women with HIP (case group) and 100 newborns delivered to normotensive pregnant women (control group) matched for gestational age and parity. They were recruited using a systematic random sampling method through the labor wards and theatres.
Demographic data, obstetric history, data on HDP and birth outcomes of their mothers were retrieved from the case notes and documented with the help of a proforma. The newborns cord blood was sampled for hematocrit (HCT) check.
Babies whose mothers had multiple pregnancies, Rh incompatibility, renal or heart disease, diabetes mellitus, history of chronic pulmonary disease or smoking were excluded from the study. The mode of delivery, sex, gestational age at birth and Apgar scores were obtained for each of these newborns.
Ethical considerations
The study was carried out in accordance with the ethical standards of the UPTH ethical committee and with the Helsinki Declaration. Parents or caregivers of the newborns gave their informed consent before recruitment.
Sample collection
Umbilical cord was clamped within 15 second from delivery with no stripping of the cord done and the newborn was held at same level of the mother’s introitus. All subjects had their cord blood sampled and analyzed for HCT which was done manually in duplicates using plain capillary tubes (75 mm long with 1 mm bore and 0.2–0.25 mm wall thickness) spun in a microhematocrit centrifuge and the average taken. The Apgar scores in the 1st and 5th minutes were also recorded. Newborns were considered polycythemic if HCT ≥65 and asphyxiated if Apgar score was ≤6 in the 1st or 5th minute, for the purpose of this study.
Statistical analysis
Data were analyzed using the Statistical Package for Social Sciences (SPSS) software version 16. Results were presented in tables and charts as mean±standard deviation (SD) and percentages. Fisher’s exact test was used to test the association of polycythemia with birth asphyxia. Statistical significance was set at 0.05.
Results
There were a total of 200 newborns; 100 from mothers with HDP serving as the case group, and 100 from normotensive women serving as the control group. The demographic variables (age, parity and gestational age) of both groups of mothers were not statistically different as in Table 1. The gestational age (GA) at birth of newborns of the case group ranged from 28 to 42 week, with mean and modal GA of 37.8±3.1 and 38 week respectively. The GA of the control group ranged from 31 to 42 week with mean and mode of 38.6±2.1 and 40 weeks respectively. The mean GA was statistically significant (p value = 0.019).
Maternal and neonatal demographics
Maternal and neonatal demographics
Legend: GA indicates gestational age, HDP indicates hypertensive disorders in pregnancy, N denotes number of subjects, NA denotes not applicable.
The Apgar scores in the 1st and 5th minutes for the case group ranged from 3 to 9 and 4 to 10 respectively, while that of the control group was 3 to 9 and 5 to 10 respectively. The mean Apgar score in the 1st and 5th minutes for the case group are 7±2 and 8±1 whereas the mean Apgar score in the 1st and 5th minutes for the control group is 7±2 and 9±1 respectively.
The mean HCT of the case and control groups were 49.7±9.3% and 45.40±7.5% respectively. Ninety-two (92.0%) subjects have HCT <65% and categorized as case group without polycythemia and 8 (8.0%) subjects who had HCT ≥65 are categorized as the case group with polycythemia. None of the control newborn had polycythemia. In the case group, the mean HCT of the 92 subjects without polycythemia and the 8 subjects with polycythemia are 49.6±7.9% and 67.5±2.6% respectively, while the mean HCT for the control group is 45.5±7.5%, as in Table 2.
Hematocrit and Apgar scores of the subjects
Legend: Table showing mean values for hematocrit and 1st and 5th minute Apgar for study participants. HDP signifies hypertensive disorders in pregnancy, HCT signifies hematocrit, N signifies number of subjects.
The mean Apgar scores of newborns of case group without polycythemia were 6.9±1.7 and 8.5±1.4 in the 1st and 5th minute respectively while those with polycythemia were 4.1±1.8 and 6.6±2.1 in the 1st and 5th minute respectively. The mean Apgar scores in the 1st and 5th minutes of newborns in the control group are 7.00±1.5 and 8.9±1.0 respectively as illustrated on Table 2.
Thirty three (33.0%) of the newborns of women with HDP had birth asphyxia compared to 35 (35.0%) of the controls. There was no significant difference in the incidence of birth asphyxia between both groups (p = 0.765). Out of the 8 newborns in the case group with polycythemia, 7 (87.5%) had asphyxia while 26 (28.3%) newborns in the case group without polycythemia had asphyxia. Birth asphyxia was significantly associated with polycythemia (p = 0.002) in newborns of women with HDP as in Table 3.
Test of association between polycythemia and birth asphyxia in newborns of women with hypertensive disorders in pregnancy and normotensive mothers
Legend: Table showing that polycythemia is significantly associated with asphyxia. N signifies number of subjects.
There is a significant positive correlation between the HCT and Apgar scores (both 1st and 5th minutes) in newborns of the cases without polycythemia, r = 0.221, p = 0.034 and r = 0.255, p = 0.014, (see Table 4, Figs. 1 and 2). There is a negative correlation between the HCT of neonates with polycythemia (cases) and Apgar scores of 1st and 5th minutes but it was not statistically significant, r = –0.287, p = 0.491 and r = –0.436, p = 0.281 (Table 3). There is no significant correlation between HCT and Apgar score in the controls, r = 0.032, p = 0.755 and r = –0.167, p = 0.096 in the 1st and 5th minutes respectively as shown in Table 3.
Correlation between hematocrit and Apgar scores
Legend: Table showing positive and negative correlation of hematocrit and Apgar scores for cases with and without polycythemia respectively. HCT signifies hematocrit, N signifies number of subjects.

Correlation between hematocrit and Apgar in 1st minute in neonates of women with hypertension. Legend: HDP signifies hypertensive disorders in pregnancy, HCT signifies hematocrit.
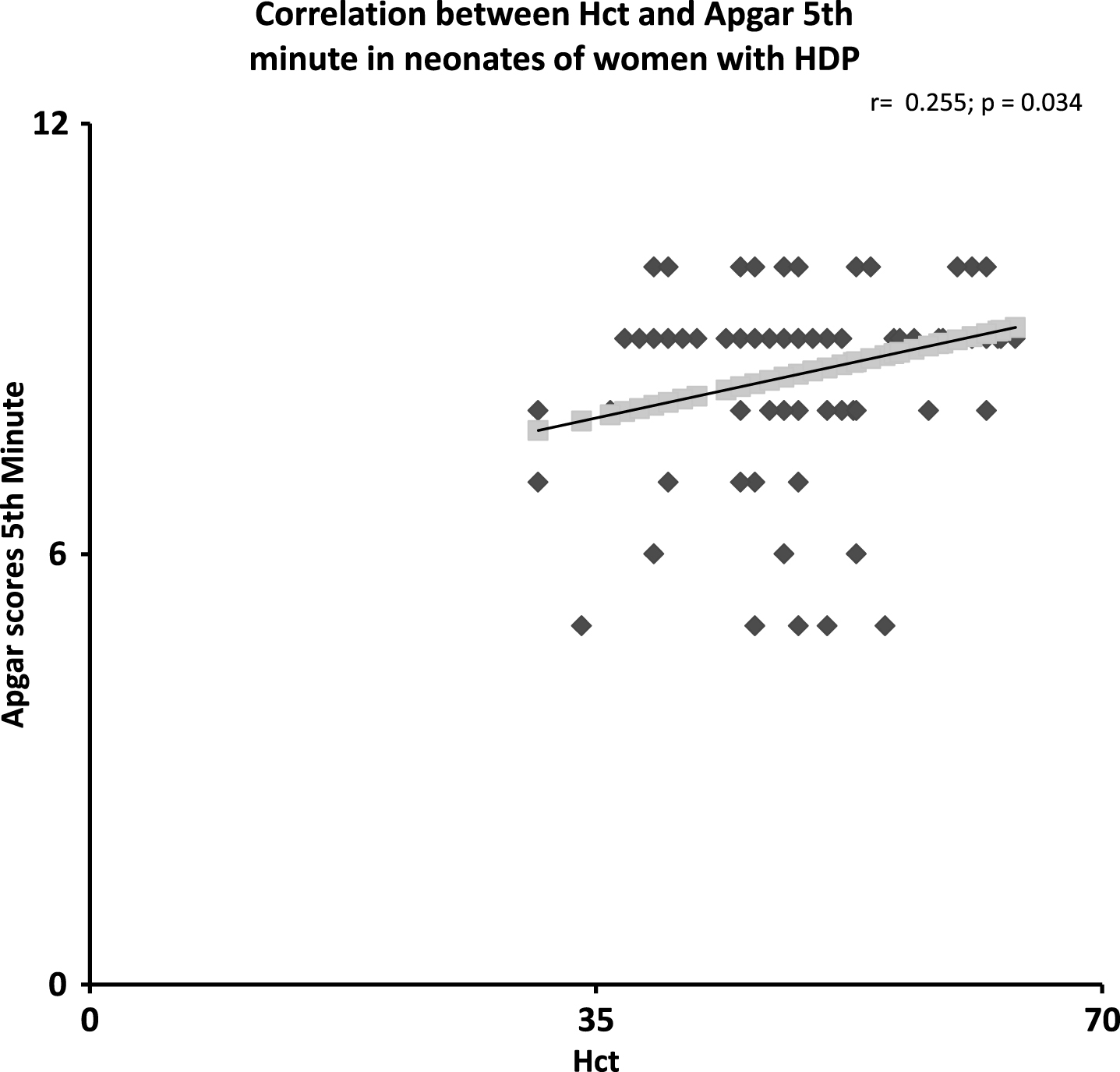
Correlation between hematocrit and Apgar in 5th minute in neonates of women with hypertension. Legend: HDP signifies hypertensive disorders in pregnancy, HCT signifies hematocrit.
Hypertension is one of the commonest medical complications in pregnancy with both maternal and fetal/neonatal sequelae leading to increased morbidity and mortality [2, 19]. One of the fetal effects is that on hematological parameters, particularly hematocrit (HCT) [8, 10]. Placental insufficiency associated with hypertensive disorders in pregnancy (HDP) causes fetal hypoxia, thus stimulating erythropoietic activity leading to relative increase in their hematocrit [9, 20].
We observed a statistically significant positive correlation between HCT and Apgar scores in both 1st and 5th minutes in the cases without polycythemia, but a negative correlation between HCT and Apgar score in both 1st and 5th minutes in the case with polycythemia. This supposes that perinatal wellbeing and birth outcome improves with increasing HCT but not to the point of polycythemia. However, there is paucity of data on correlation between HCT and Apgar score of newborns of hypertensive mothers. In the work by Salari et al., [21], they found there was no effect of HCT on Apgar score. This could be because the increase in hematocrit they observed was artificially induced by late cord clamping and was not due to intrauterine hypoxia which equally imparts on Apgar score. Hanoudi in a related study observed that there was no correlation between HCT and Apgar, but he excluded women that were prone to intrauterine hypoxia, e.g. mothers with diabetes mellitus, hypertension etc. [22]. He also used only neonates not at risk of asphyxia, that is neonates with Apgar scores >7.
In the subgroup of the cases that had polycythemia, there was a negative correlation between HCT and Apgar score (1st and 5th minutes), though it was not statistically significant. This could be because just a few of the neonates had polycythemia, if this study was carried out in a larger population of subjects it could have been significant since hypoxia which is thought to cause polycythemia in these subjects, has an inverse relationship with Apgar score [23]. Uterine hypoxia causes increased erythropoiesis through increased production of erythropoietin which may lead to increase in blood viscosity and hence further decrease oxygen delivery to the fetus causing low Apgar score. Hematocrit has a linear relationship viscosity up to a HCT of ≥65% (polycythemia) when it becomes exponential [24].
There was no correlation between HCT and Apgar score in the controls which is similar to the observations Salari et al., [19] and Hanoudi [22]. In this group of neonates, there was no intrauterine hypoxic event.
Polycythemia in the newborn is a risk factor for neonatal jaundice which if not diagnosed early and appropriately managed may be complicated by kernicterus [25]. Identification and proper management of polycythemic newborn will further reduce the perinatal morbidity associated with HDP.
Conclusion and recommendation
The incidence of polycythemia is significantly higher in newborns of women with HDP. Though the frequency of birth asphyxia did not differ significantly between newborns of women with HDP and normotensives, polycythemic newborns of women with HDP had a significantly higher incidence of birth asphyxia. Therefore, birth outcome, as determined by Apgar score, is influenced by hematocrit and improves with rising hematocrit up to 65% beyond which there may be birth asphyxia.
We recommend that neonates of mothers with HDP should have their hematocrit checked and anticipatory management of neonates with low Apgar score and HCT in the polycythemic range to reduce the morbidity and mortality from HDP.
Conflict of interest
Nothing to declare.