
Abstract
BACKGROUND:
Dexamethasone is administered to some preterm infants with chronic lung disease to facilitate weaning from mechanical ventilation. Heart rate characteristics (HRC), including heart rate variability (HRV), may be impacted by glucocorticoids and may predict extubation readiness. A commercially available monitor developed for sepsis detection continuously calculates HRV and an HRC index, which are inversely related.
OBJECTIVES:
Determine the impact of dexamethasone on HRV and the HRC index, in relation to extubation success.
METHODS:
We identified 109 preterm infants who received dexamethasone while on mechanical ventilation and had HRC index monitoring data available. Average hourly HRV and HRC index were compared the day before and the day after initiation of dexamethasone in three groups: infants who remained on mechanical ventilation, those who were successfully extubated, and those who were extubated and required reintubation in < 3 days.
RESULTS:
There was a significant increase in HRV and decrease in the HRC index the day after dexamethasone was started (HRV 16.2±0.5 vs 27.6±1.1 ms; HRC index 1.51±0.11 vs. 0.79±0.06 mean SE, p < 0.001). The 63 infants who were extubated within a day of starting dexamethasone had significantly higher HRV compared to those who remained on mechanical ventilation. There was no difference in HRV or its change with dexamethasone in the 45 infants who remained successfully extubated compared to the 18 infants who required reintubation within 3 days.
CONCLUSION:
Dexamethasone improves HRV and lowers the HRC index in preterm infants with chronic lung disease on mechanical ventilation.
Keywords
Introduction
Dexamethasone is administered to some preterm infants with severe lung disease [1, 2] and has anti-inflammatory and other physiologic effects including changes in heart rate variability (HRV), which reflects autonomic nervous system activity [3]. Glucocorticoid effects on HRV have not been well described in preterm infants but have been studied in other clinical scenarios. In human fetuses, maternal dexamethasone or betamethasone administration for fetal lung maturation in the setting of threatened preterm birth has been linked to an acute, transient increase in HRV [4, 5], and in critically ill adult trauma patients with adrenal insufficiency and depressed HRV, glucocorticoid replacement therapy was reported to increase HRV toward normal levels [6]. Although the mechanism appears to relate in part to anti-inflammatory effects, we have previously shown in a mouse model that dexamethasone increases HRV both in the presence and in the absence of an inflammatory stimulus, perhaps through improving autonomic nervous system function [7].
Understanding factors that impact HRV is important in the care of critically ill patients. Normal beat-to-beat variability is characterized by frequent small accelerations and decelerations modulated by sympathetic and parasympathetic input to cardiac pacemaker cells, and reduced HRV is a sign of pathology. In sepsis, for example, HRV is markedly depressed. Our group developed a heart rate characteristics (HRC) monitor as an early warning system for sepsis in preterm infants in the NICU [8–11]. The monitor continuously analyzes the electrocardiogram signal, and a high HRC index reflects three abnormalities: low HRV, increased decelerations relative to accelerations, and low sample entropy [12]. The HRV measurement calculated by the HRC index monitor is variance of the inter-heartbeat intervals, with the two measurements being inversely related. We have shown that low HRV and a high HRC index can occur not only in sepsis but also in other pathologic conditions such as respiratory failure[12–14]. We also observed that many infants given dexamethasone to facilitate weaning from mechanical ventilation had a substantial decline in their HRC index. We performed the current analysis to determine the incidence and magnitude of this response. Further, since low HRV has been reported to be associated with extubation failure in preterm infants, [15] we sought to determine whether HRV or its change after dexamethasone differed in infants who were successfully extubated compared to those who failed extubation.
Methods
Patient population and respiratory support
This study was approved by the University of Virginia Institutional Review Board with waiver of consent for retrospective analysis of deidentified patient data. The UVa NICU is a level 3 unit that admits approximately 100 very low birth weight (VLBW, <1500 grams) preterm infants per year. We searched the hospital Clinical Data Repository to identify all VLBW infants treated with dexamethasone to facilitate weaning from mechanical ventilation from 2004–2012. We excluded infants who had surgery within 2 days of receiving dexamethasone since anesthetic agents and surgical procedures are known to impact HRV.
During the years of the analysis, the general guideline in the unit was to consider a short course of dexamethasone if an infant was on very high ventilator support and unable to wean, or had previously failed extubation due to moderate to severe lung disease. Dosing was variable, generally in the range of 0.125–0.5 mg/kg/day for several days. For infants who received more than one course of dexamethasone, only the first course was analyzed. Criteria for extubation varied by patient and by clinician but the general guideline was PEEP≤6, mean airway pressure≤12, and FiO2≤50%. Infants were extubated to nasal CPAP. Extubation failure was defined as need for reintubation within 72 hours, and criteria for reintubation were variable but generally included significant respiratory acidosis (CO2> 70) or hypoxemia (more than 20% increase in FiO2) or frequent or severe apnea. The HRC index was not used for clinical decisions about dexamethasone use, extubation readiness, or need for reintubation.
Medical records were reviewed for gestational age, birth weight, day of age and post menstrual age when dexamethasone was started, and ventilatory support.
Heart rate variability (HRV) and heart rate characteristics (HRC) monitoring
HRV is continuously measured in all infants in the NICU by the HRC index monitor (HeRO monitor, Medical Predictive Science Corporation, Charlottesville, Virginia). The monitor was developed as an early warning system for sepsis and, with no additional connections to the patient, takes the electrocardiogram (ECG) signal from the bedside monitor to measure HRC. After filtering out aberrant electrocardiogram complexes representing ectopic beats, the monitor detects R wave peaks. It then runs a validated algorithm to calculate an HRC index, which was developed to be the fold increased risk that an infant will be diagnosed with sepsis in the ensuing 24 hour period [8, 16–18]. The three abnormal HRC that go into the calculation are low HRV, transient decelerations, and low entropy. The time series HRV measurement incorporated into the HRC index is heart rate variance. The HRC index and HRV are calculated hourly from the previous 12 hours of ECG signal. We excluded the date that the first dose of dexamethasone was given (to allow time for the medication to take effect and to account for 12 hour averaging of the HRV and HRC index) and we compared the average hourly measurements the day before and the day after dexamethasone was started.
Statistical analysis
Data are presented as mean (standard error) or n (%), unless otherwise noted. Average hourly HRV and the HRC index were compared before and after dexamethasone and between infants who failed versus those that were successfully extubated, using paired t-tests with two-tailed significance level set at 0.05. The Spearman’s correlation coefficient was calculated before and after dexamethasone for HRV and the HRC index (GraphPad 7, San Diego, CA).
Results
Clinical characteristics
In the eight year period, 110 VLBW infants were identified who received dexamethasone while on mechanical ventilation and had HRV and HRC index data available the day before and after the start date of dexamethasone. One infant developed necrotizing enterocolitis the day after dexamethasone was started and was excluded since NEC is known to affect the HRC index [19]. Clinical characteristics of the 109 infants included in the analysis are shown in Table 1. Sixty-three infants (58%) were extubated within one day of starting dexamethasone, and 18 of these infants (29%) required reintubation within 3 days of extubation.
Clinical characteristics, respiratory support, and HRV change with dexamethasone
Clinical characteristics, respiratory support, and HRV change with dexamethasone
n (%) or mean (SE) are shown. Vent = ventilator; Extub = extubation; HRV = heart rate variability.
There was a significant increase in HRV and decline in the HRC index the day after dexamethasone was started. Figure 1 shows a representative example of hourly values in one infant the day before and after the dexamethasone start date. Figure 2 shows the mean hourly HRV and HRC index in each infant the day before (x axis) compared to the day after dexamethasone (y axis). The Spearman’s correlation coefficient for HRV is r = 0.6339, p < 0.0001 and for HRC index is r = 0.5373, p < 0.0001. The mean HRV increased from 16.2±0.5 ms to 27.6±1.1 ms and the HRC index decreased from 1.51±0.11 to 0.79±0.06 (p < 0.001). HRV increased, on average, 73% after dexamethasone, and 99 infants (91%) had at least a 10% increase in HRV over their prior baseline.
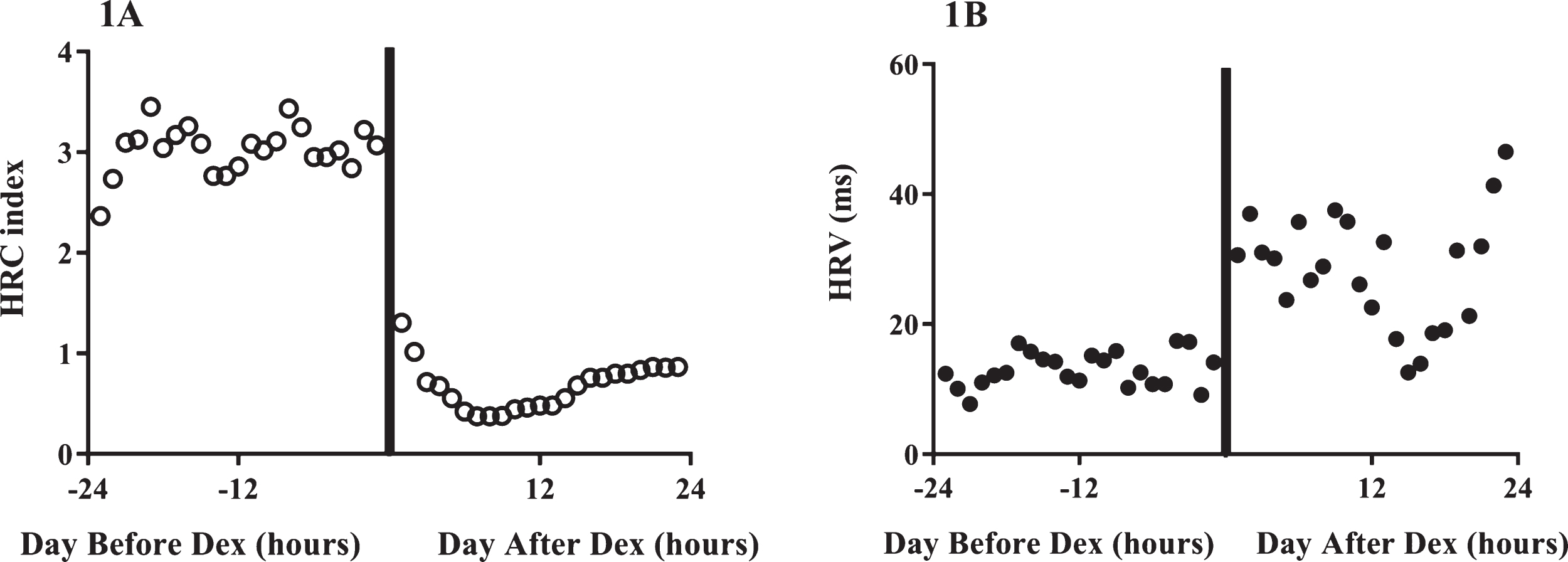
Representative example of the HRC index and HRV before and after dexamethasone. An infant born at 25 weeks gestation received dexamethasone at 34 days of age. The hourly HRC index (open circles, 1A) and HRV (filled circles, 1B) are shown the day before and the day after dexamethasone administration. The solid vertical line represents the dexamethasone start date.
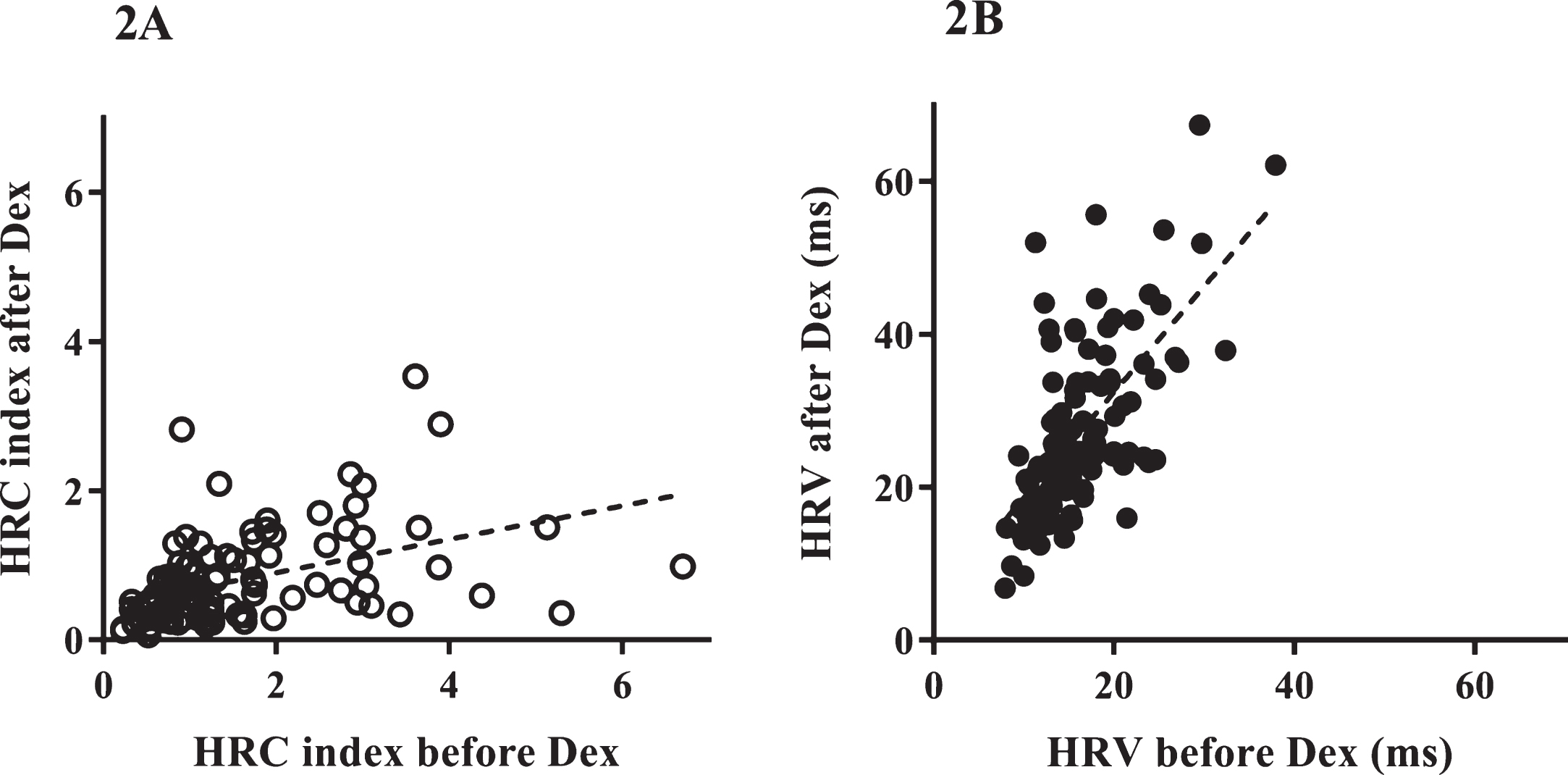
HRC index and HRV for each infant before and after dexamethasone. For each of the 109 infants, the average HRC index (open circles, 2A) and HRV (filled circles, 2B) are shown the day before (x-axis) and the day after (y-axis) dexamethasone was started. There was a significant decrease in the HRC index and increase in HRV after dexamethasone administration (p < 0.001). The Spearman’s correlation coefficient for HRC index is r = 0.5373, p < 0.0001 and for HRV is r = 0.6339, p < 0.0001.
The 63 infants who were extubated the day after starting dexamethasone had significantly higher HRV than those who remained on mechanical ventilation (17.6 ms versus 14.4 ms p = 0.002 before dexamethasone, and 31.1 ms versus 22.7 ms p < 0.001 after dexamethasone) (Fig. 3).
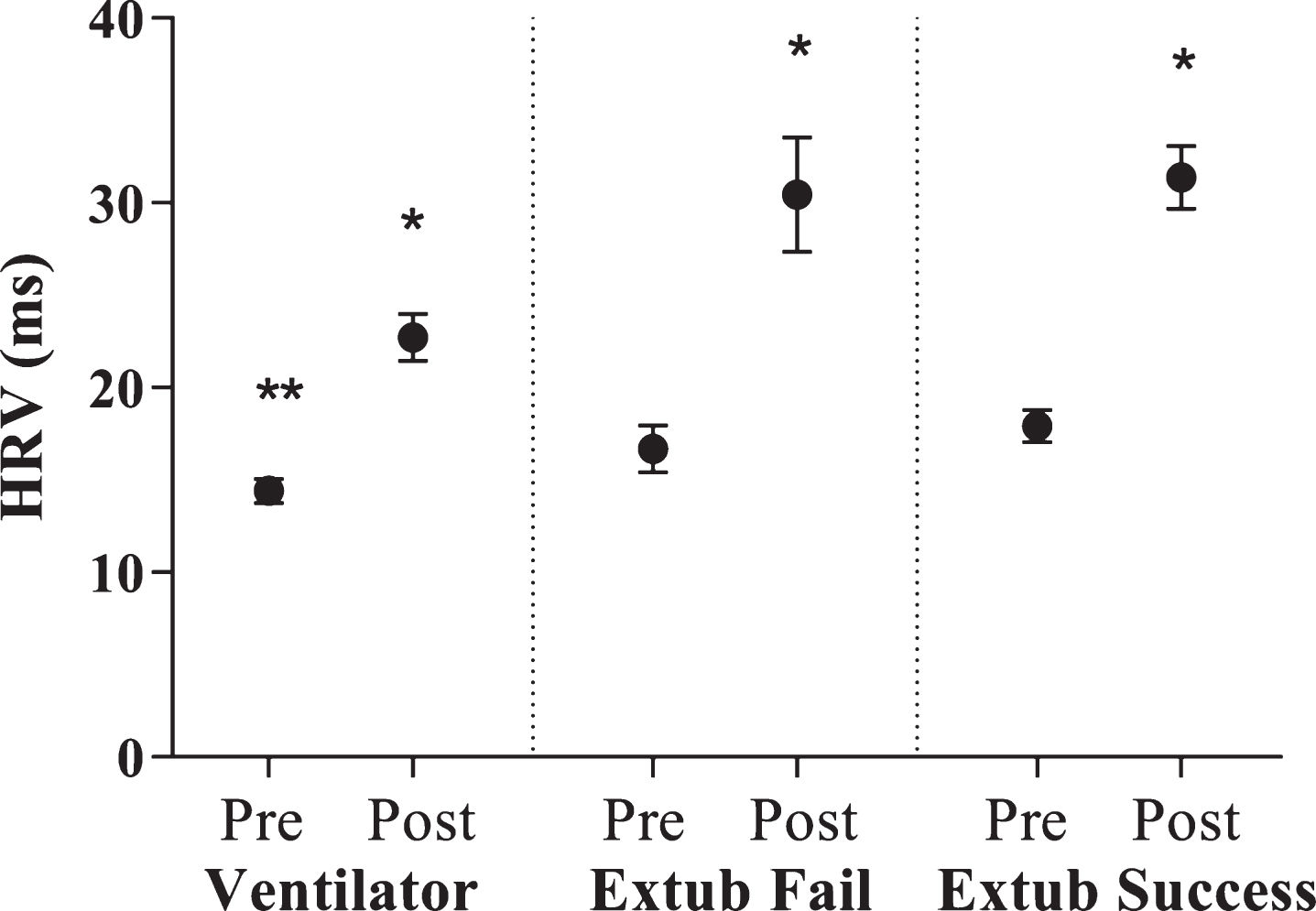
HRV before and after dexamethasone based on respiratory support. The average HRV is shown the day prior (“pre”) and the day after (“post”) starting dexamethasone for three groups of infants. For each group, the HRV increased significantly after dexamethasone (*p < 0.001). The 46 infants who remained on mechanical ventilation had significantly lower HRV than the 63 infants who were extubated within a day of starting dexamethasone (**p = 0.002). Among the 63 infants who were extubated, there was no difference in HRV pre- or post-dexamethasone or in the change in the 45 infants who remained extubated compared to the 18 infants who required reintubation within 3 days.
In the 45 infants who were successfully extubated compared to the 18 infants who required reintubation within 3 days, HRV was not significantly different the day before or the day after dexamethasone administration (before 17.9 ms versus 16.7 ms p = 0.45, and after 31.4 ms versus 30.4 ms p = 0.78) (Fig. 3). The change in HRV after dexamethasone was also not significantly different in the infants that were successfully extubated compared to those that failed (79% increase versus 88% increase, p = 0.58). The HRC index was inversely proportional to HRV and also not significantly different between infants with successful versus failed extubation.
Discussion
Dexamethasone is used in the NICU in some infants with moderate to severe lung disease. We found that preterm infants on mechanical ventilation treated with dexamethasone experienced a significant increase in beat-to-beat heart rate variability (HRV), as measured by a heart rate characteristics (HRC) index monitor. Infants who were extubated after dexamethasone was started had significantly higher HRV than those who remained on mechanical ventilation. Among infants who were extubated, there was no significant difference in HRV or its change after dexamethasone between those who remained off mechanical ventilation compared with those who required intubation within 3 days.
HRV is measured as part of a heart rate characteristics index using a monitor that serves as an early warning system for sepsis. Since the HRC index is monitored in many NICUs, it is important to understand the impact of common medical conditions and medications on the score. We previously reported that lung disease and respiratory decompensation can lead to a high HRC index [12–14], which may in part reflect low HRV due to lung inflammation, respiratory acidosis, or hypoxia.
Our finding of improvement in HRV with glucocorticoid therapy is consistent with other reports in the literature, including short-term increases in fetal HRV reported following maternal antenatal corticosteroid treatment [4, 21], and normalization of HRV in septic adults treated with steroids [6]. In studies in a mouse model, we found that HRV was significantly depressed after administration of an inflammatory stimulus (Escherichia coli lipopolysaccharide), and that dexamethasone treatment blunted inflammatory cytokine expression and shortened the duration of HRV depression. Although steroid-mediated improvement in HRV is likely due in part to suppression of inflammation, in our mouse studies we found that dexamethasone dramatically increased HRV even in absence of any inflammatory stimulus [7]. We speculate that the mechanism may relate to upregulation of both adrenergic and cholinergic signaling [22, 23].
We found that infants who remained on mechanical ventilation after starting dexamethasone had significantly lower HRV (and a higher HRC index), likely reflecting more severe lung disease. Among the 65 infants who were extubated, there was no significant difference in HRV or its change after dexamethasone in those who remained off mechanical ventilation compared to those infants who failed extubation. In contrast, another group has reported in a prospective study that HRV was significantly higher in infants who were successfully extubated compared to infants who required reintubation [15]. This may reflect the difference in timing of HRV measurement (immediately prior to extubation versus over the prior day) or it may be due to differences in clinical variables such as gestational or postmenstrual age or level of ventilatory support, which have a major impact on extubation success.
Conclusion
In preterm infants on mechanical ventilation, dexamethasone administration led to improvement in HRV as reflected by a decrease in a continuously monitored HRC index. Larger studies would be needed to determine whether HRV or the HRC index can be used in conjunction with other clinical variables to predict extubation readiness in preterm infants.
Disclosure statements
The authors have no financial relationships or conflicts of interest to disclose.
Footnotes
Acknowledgments
The authors have no contributors.