
Abstract
Introduction
Diabetic ketoacidosis (DKA) is an uncommon but serious complication of diabetes in pregnancy that can be life-threatening to both mother and fetus [1, 2]. In fact, the reported frequency of fetal loss ranges from 9–36% during an episode of DKA in pregnancy [3–7]. The reported incidence of DKA in all diabetic pregnancies ranges from 0.5–3% depending on the population studied [2–4, 8]. Although seen most commonly in patients with type 1 diabetes, there are increasing reports of DKA occurring in women with type 2 diabetes as well as gestational diabetes[5, 10].
While infection and medication non-compliance are established causes of DKA, pregnancy is also a potent risk factor due to normal physiologic changes and altered metabolic demands [11]. DKA develops due to an absolute or relative insulin deficiency. This perceived starvation causes counter regulatory hormones (such as glucagon, cortisol, and catecholamines) to be secreted which, in turn, leads to increased gluconeogenesis, glycogenolysis,ketogenesis, lipolysis and ultimately worsening hyperglycemia and a metabolic acidemia [12]. Hormones produced specifically during pregnancy—human placental lactogen, prolactin, and cortisol—increase insulin antagonism and contribute to hyperglycemia [12, 13]. In addition, pregnancy is a state of primary respiratory alkalosis with decreased overall buffering capacity [11]. Thus, the production of free fatty acids and ketone bodies can quickly overwhelm the ability to compensate for the acidosis. Finally, there are also a number of obstetric-related clinical conditions that are risk factors DKA. These include hyperemesis gravidarum, β-adrenergic medications used for tocolysis, and antenatal steroids administered for fetal lung maturity [8, 15].
The clinical presentation of DKA in pregnancy can be variable as women often present with non-specific symptoms that are also common in a normal pregnancy such as nausea, vomiting, fatigue, dehydration, or abdominal pain. As such, the diagnosis of DKA in pregnancy is focused on laboratory abnormalities that include hyperglycemia (>200–300 mg/dL), anion gap acidosis (AG >12 mEq/L), pH <7.30, HCO3 <15 mEq/L, and ketonemia or ketonuria [11, 16]. Once identified, DKA is considered an obstetrical emergency and goals of management focus on prompt diagnosis, correction of hypovolemia to increase uteroplacental and renal perfusion, insulin to lower serum glucose, correct acidosis and electrolyte aberrations, and identification and treatment of any underlying causes [12].
Although these treatment recommendations have been recognized as underpinnings of care of DKA in pregnant women, there is little data that establishes the anticipated clinical resolution or recovery time. Therefore, the impetus of our study was to examine the precipitating factors, laboratory abnormalities, treatment strategies, and course of clinical recovery in pregnancies complicated by DKA.
Materials and methods
This is a retrospective cohort study of pregnancies complicated by at least one episode of DKA between October 1999 and June 2015. With the approval of the Institutional Review Board of the University of Texas Southwestern Medical Center and Parkland Hospital, we examined all of the admission and discharge logs from our obstetric acute care unit and queried hospital admission and discharges for ICD-9 codes [648.0X (X = 0,1,2,3,4) and 250.1X (X = 0,1,2,3)] in an effort to identify all admissions for diabetic ketoacidosis in pregnancy.
Upon review, the diagnosis of DKA was confirmed by the presence of at least four of the five following laboratory criteria: hyperglycemia (defined as >250–300 mg/dL) [12, 13], anion gap >12 mEq/L, positive urine or serum ketones, pH <7.3, and HCO3 <15 mEq/L. Serial admissions by the same patient were treated as separate episodes so long as inclusion criteria were met. With rare exception, these women were treated in either labor and delivery or the obstetrical acute care unit which is adjacent to labor and delivery. This unit functions as an obstetric critical care unit and is staffed by obstetric nurses with a nurse-to-patient ratios of 1 : 1-1 : 2. Management within labor and delivery and the obstetrical acute care unit has been described and is coordinated with obstetric residents supervised by maternal-fetal medicine faculty and fellows [17]. Treatment of DKA in pregnancy at our hospital is concordant with the treatment schema recommended by the American College of Obstetricians and Gynecologists, with initial boluses of intravenous crystalloid, insulin and frequent laboratory assessment with correction of hyperglycemia, dehydration, and electrolyte derangements as the cornerstones [16].
For each episode of DKA, a comprehensive evaluation of the patient’s clinical condition included a review of their medical and prenatal record to include maternal demographics, body mass index, type of diabetes and age at diagnosis; severity of disease as indicated by retinopathy or nephropathy; hemoglobin A1c, presenting complaint, current insulin therapy and compliance with therapy; concurrent illness or infection; and other pregnancy complications. Also assessed were initial laboratory studies such as glucose, anion gap, bicarbonate, pH, potassium, creatinine, and urine or serum ketones. The trends of these laboratory values over time were assessed and time to resolution of hyperglycemia, anion gap acidosis, and ketonuria were plotted.
Evaluation of management included the type and amount of insulin and intravenous fluids given over time, and other factors such as gestational age, length of stay, pregnancy outcomes and perinatal complications. Perinatal outcomes of particular interest included hypertensive disease of pregnancy, preterm birth, cesarean delivery, birthweight, stillbirth or neonatal death, neonatal intensive care unit admission, neonatal hypoglycemia or hyperbilirubinemia, and fetal malformations.
Laboratory analytes were measured at epochs of time, including on admission. These values and the time course of recovery to normal were compared between type 1 and type 2 diabetics, and by gestational age (<24 weeks vs ≥24 weeks) using the Wilcoxon rank sum test and a random effects model. Perinatal outcomes in these groups were also recorded, though the small number limits the analysis.
Results
During this 16-year investigation, nearly 223,000 women were delivered at Parkland Hospital, and of these, 14,532 (6.5%) were complicated by diabetes. We identified 33 women who had a total of 40 admissions for DKA for an incidence of 0.2% for all diabetic women during pregnancy. All women had at least four of the five diagnostic criteria on presentation. With one exception, all patients were treated and managed in our obstetric acute care unit as previously described [17].
Selected maternal demographics are presented in Table 1. Two-thirds (69%) of the women had type 1 diabetes and were diagnosed at a mean 15.8 years of age. The average age at presentation was 25 years, and 30% were nulliparous. The cohort was evenly divided among Caucasian, African-American, and Hispanic ethnic groups, with about a third of patients in each category. The average glycosylated hemoglobin of all women on admission was 10%; in a third the hemoglobin A1c was >12%. Almost a fourth of the women also had chronic hypertension.
Selected findings in 33 pregnant women with diabetic ketoacidosis
Selected findings in 33 pregnant women with diabetic ketoacidosis
Data expressed as Mean±SD or N(%). aIncludes only 20 measurements.
Table 2 displays selected admission information and laboratory values. All but one patient had nausea and vomiting as a presenting complaint, and all had ketonuria. Almost half (47.5%) of the admissions were during the first trimester. The mean initial glucose was 380 mg/dL (range 158–776 mg/dL), and only three patients had a presenting glucose <200 mg/dL. An arterial blood gas was performed in 26 of the 40 admissions and the mean pH was 7.27.
Admission and laboratory criteria for 40 episodes of diabetic ketoacidosis in 33 pregnant women
Data expressed as Mean±SEM or N (%). Glucose values are given as a range.
Intravenous fluids, insulin, and potassium were administered to all patients shortly after diagnosis. The average initial bolus was 1.5 L of crystalloid solution (0.9% saline), and over half were given more than 10 units of intravenous regular insulin within the first hour. Within the first 4 hours, they were given an average of almost 3 L of crystalloid, and 21 units of intravenous insulin (range 7–65 units). None of these women required bicarbonate. As shown in Fig. 1, laboratory values normalized quickly with this treatment. Specifically, after 6 hours, the average glucose was less than 200 mg/dL (175 mg/dL), and the anion gap normalized by 8 hours in most women. Resolution of ketonuria took considerably longer and only 6 women had negative urine ketones by 24 hours after treatment began.
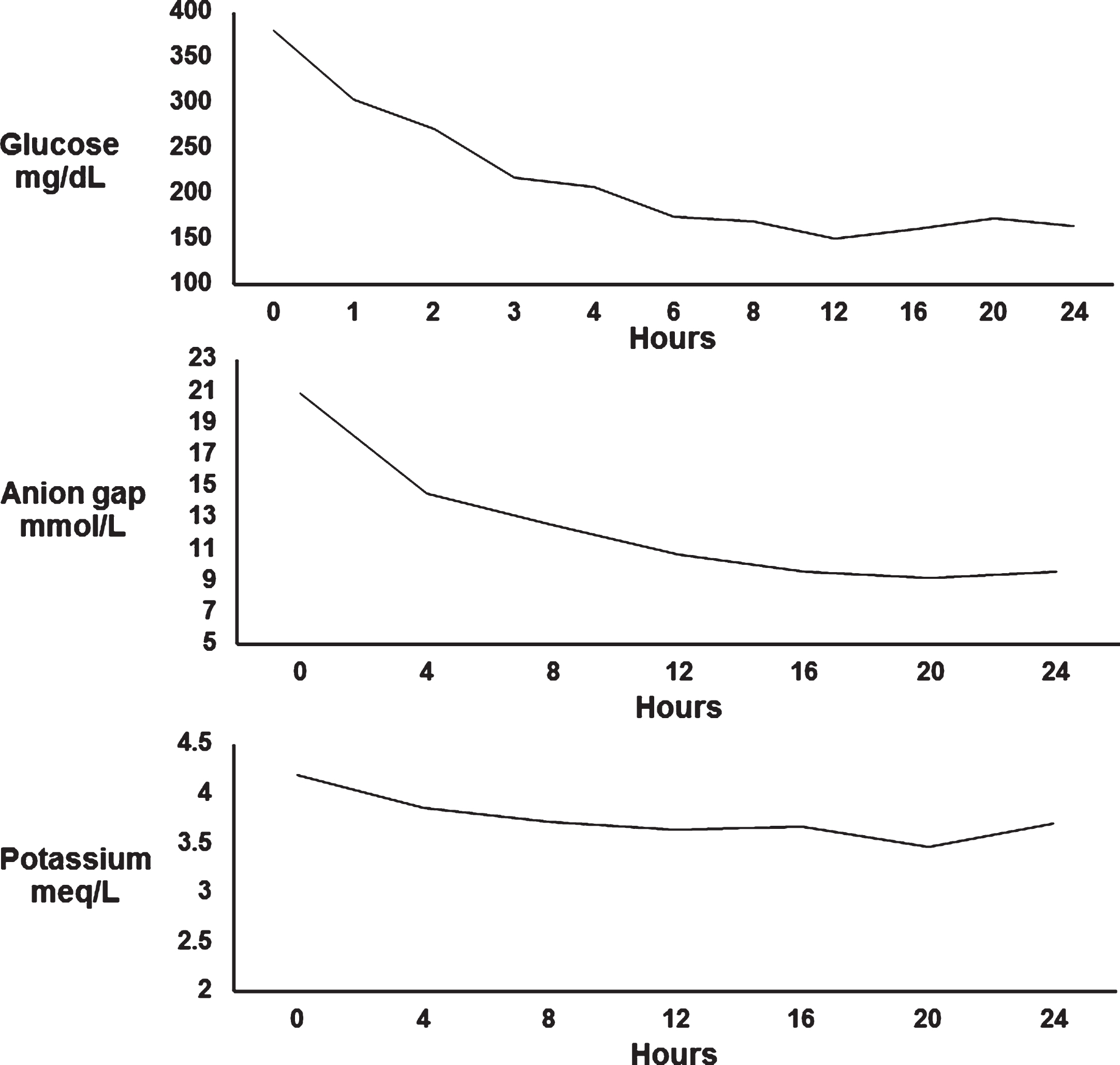
Laboratory trends.
Among the women with type 1 diabetes, the initial laboratory findings and resolution of DKA was similar to that of the whole cohort. Their average glycosylated hemoglobin on admission was 9.4%, with an initial glucose of 350 mg/dL, and an average anion gap of 21 mmol/L. Women with type 2 diabetes had an initial glucose of 458 mg/dL (p < 0.05) and a higher HgbA1c on admission (11.4%; p < 0.05). Although the glucose at the time of admission is significantly lower in the type 1 diabetics, the laboratory recovery was similar in both groups as seen in Fig. 2. There was no difference noted when comparing gestational age at admission (Fig. 3).
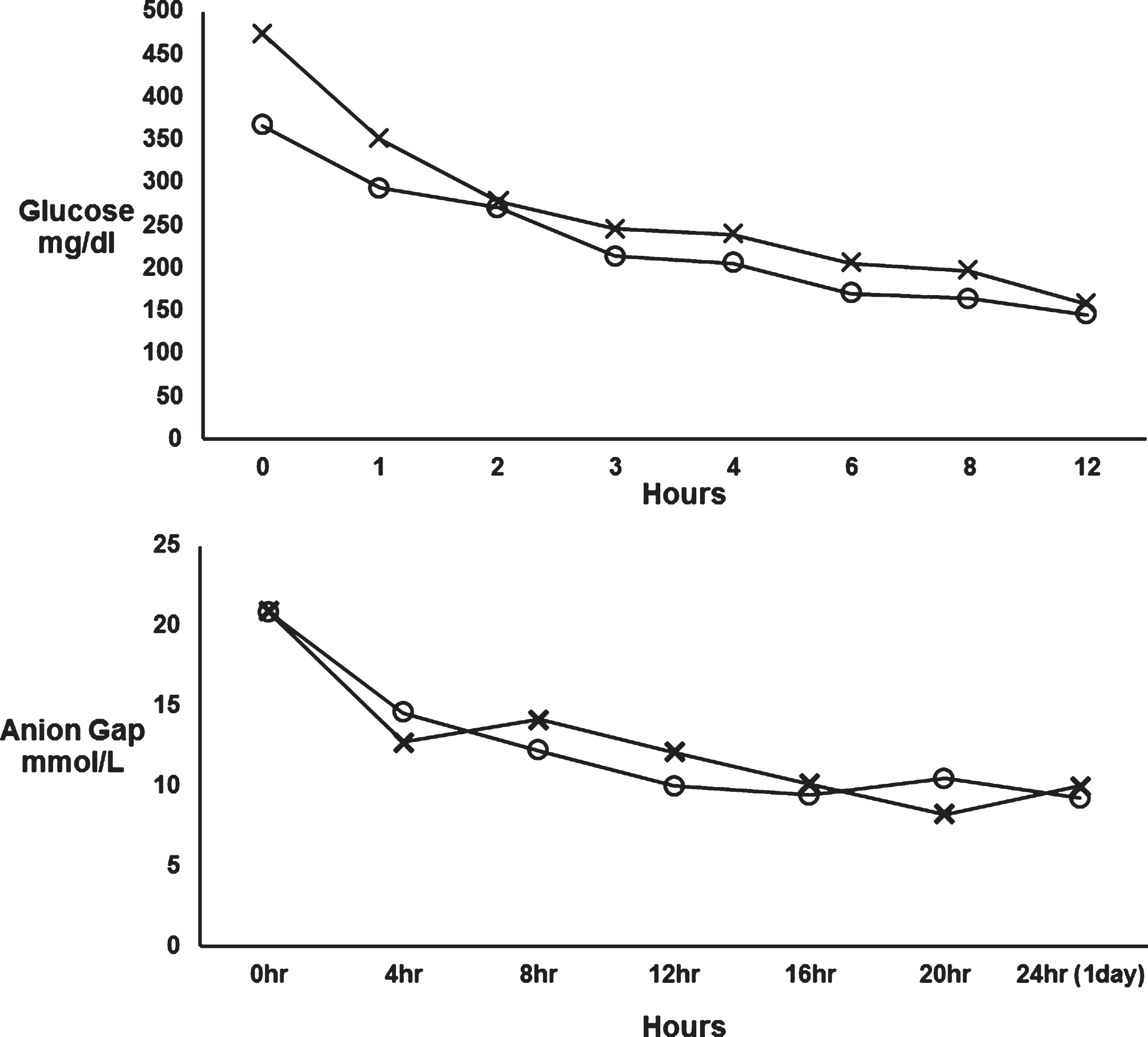
Comparing selected laboratory trends over time in type 1 (O) versus type 2 diabetes (X).
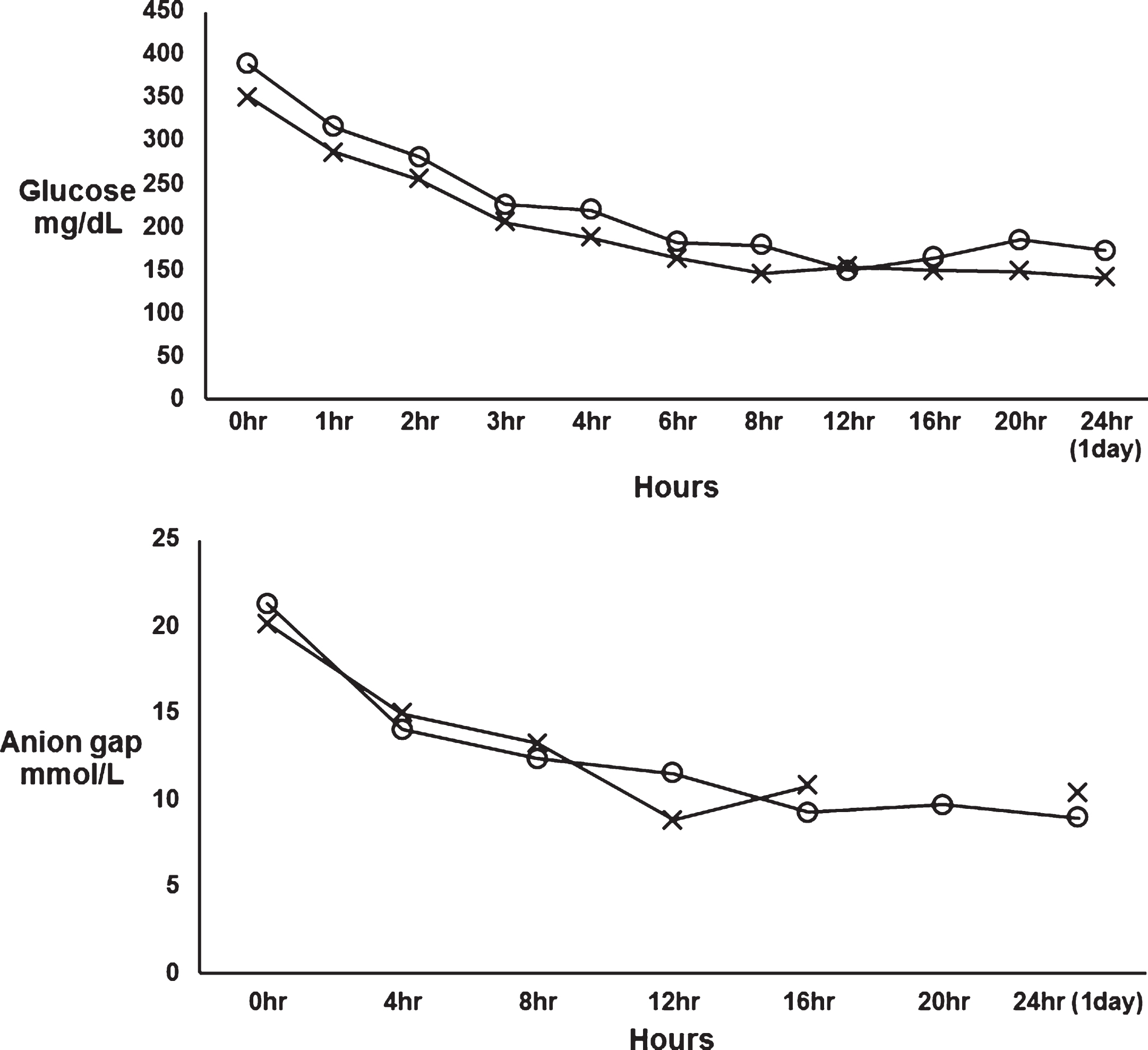
Comparing selected laboratory trends over time in diabetic women admitted at less than 24 weeks (O) versus ≥24 weeks gestation (X).
Table 3 highlights selected maternal and perinatal outcomes. Of the nine women admitted for DKA during the third trimester, eight delivered during the same admission. However, only two of those women delivered in proximity to the episode of DKA. One developed severe preeclampsia and was induced at 34 weeks after DKA had resolved, and another was delivered at 34 weeks for nonreassuring fetal status during an acute episode of DKA. Overall, five women delivered a preterm infant (at 33–36 weeks) due to preterm rupture of membranes, nonreassuring antenatal testing, or severe preeclampsia. Three of these infants were admitted to the neonatal ICU >24 hours. When considering the entire cohort, the rate of preterm birth was 35%, most due to spontaneous preterm labor. There were 3 spontaneous abortions in the first trimester. The one fetal demise at 18 weeks was in a 17-year-old woman who presented with previously undiagnosed, new-onset, type 1 diabetes with DKA. There were three major fetal malformations; one with multiple anomalies while the other two had a congenital heart malformation. All of these infants were admitted to the neonatal intensive care unit for blood glucose monitoring per protocol.
Perinatal outcomes
Data expressed as N (%), or mean±SD. Gestational age is given as range. aIncludes information on 15 deliveries.
When analyzing the outcomes according to type of diabetes (type 1 vs type 2) and by gestational age at admission (<24 weeks versus ≥24 weeks), there were no obvious differences in reason for admission, preterm birth, cesarean delivery, cause for cesarean delivery or neonatal outcomes (data not shown). However, the number of patients is not large enough to allow for adequate evaluation of clinical significance.
There are several important findings from this study that describes 16 years of experience in caring for women with DKA in pregnancy at our hospital. First, the frequency of DKA in our pregnant diabetic population is considerably less than previously reported. Second, although two thirds of these women had type 1 diabetes, DKA can be found in all variants of disease—including gestational diabetes. In most cases, these women had preexisting poor glycemic control as evidenced by the markedly elevated glycosylated hemoglobin measurements. Third, nausea and vomiting was nearly universal in pregnant women presenting with DKA. Finally, aggressive intravenous fluid and insulin therapy resulted in relatively rapid clinical resolution of DKA with overall improved perinatal outcomes compared with prior reports [3, 11].
The frequency of DKA in our pregnant diabetic population of 0.2% is substantially lower than the reported 0.5–3% [2–4, 8]. This difference is likely due, at least in part, to the high proportion of Hispanic patients in our obstetric population. Type 1 diabetes, the most common type of diabetes in those with DKA, is much less prevalent in Hispanics compared with other races and ethnicities [18]. Moreover, the incidence of type 2 diabetes is increasing with the rise in obesity, and Hispanic women are among those most affected [19]. Indicative of this, 10 women in this series had type 2 diabetes that preceded the onset of DKA. Interestingly, though the women with type 1 diabetes presented in DKA with lower glucose values, the resolution of hyperglycemia and anion gap acidosis was not different among women with these two types of diabetes.
Ideal management of DKA has been widely reported, and our approach was certainly not unique. These women were cared for in an acute care unit, either on Labor and Delivery, or rarely, in the medical intensive care unit. Aggressive and early intravenous hydration along with intravenous insulin was given as outlined in Practice Bulletin No. 60 of the American College of Obstetricians and Gynecologists [16] as well by others [11–13, 20]. This management rapidly corrected hyperglycemia and acidosis resulting in satisfactory perinatal outcomes. For example, the reported fetal mortality during an episode of DKA has been reported as high as 36% [3–7], compared with our experience of only one fetal demise in this cohort.
Initially, intravenous crystalloid boluses of 1–2 liters were given in conjunction with an intravenous insulin bolus of 10 units within the first hour. This was followed by 500–1000 mL per hour of crystalloid for the first 2–4 hours, and an intravenous insulin infusion at 2–6 units/hour, depending on the serum glucose. Laboratory studies such as a chemistry panel, electrolytes, creatinine, anion gap, complete blood count, and urine or serum ketones should be measured on arrival and every 1-2 hours initially. Our experiences indicate that routine arterial blood gas measurements are not necessary for diagnosis or management of DKA.
A thorough investigation for an underlying infection or other etiology should be pursued concurrently with initiating treatment, but should never delay treatment. In our cohort, nausea and vomiting was nearly universal as a symptom of DKA, especially in patients in the first trimester and with a prior diagnosis of diabetic gastroparesis. In these women, nausea and vomiting commonly resulted in failure to take maintenance insulin as prescribed. Other concurrent symptoms of normal pregnancy such as fatigue and abdominal pain may make the diagnosis of DKA and identifying underlying causes difficult. Thus, vigilance for the early diagnosis and determining the underlying etiology of DKA are paramount. Management should include input from a maternal-fetal medicine specialist, internist, endocrinologist, or intensivist with suitable experience.
Other things to be considered during the resuscitation and treatment phase are maintenance of intravenous access, treatment of any concurrent infection, and fetal monitoring in later pregnancy. During these acute episodes, the fetus will also be acidemic and usually exhibits a nonreassuring heart rate pattern. This can manifest as poor beat-to-beat variability and decelerations in heart rate tracings, as well as late decelerations with any contractions. The decision to deliver the fetus expediently should be weighed carefully and avoided if possible, because with treatment of the maternal condition, fetal status will improve as well. Delivery should be reserved for fetal conditions that do not improve despite maternal improvement or deteriorating maternal status despite adequate treatment [3, 20–22].
This study is limited by the fact that it is an observational, retrospective cohort study, and differing treatments were not compared. While the cohort size is limited, this is the largest, most recently collected case series to date to our knowledge. Our approach to management of these women is standardized with and verifies currently published recommendations. Using these guidelines appropriately ensures the best chance for favorable maternal and neonatal outcomes.
Disclosures
There are no potential or actual disclosures to report.
Footnotes
Acknowledgments
There are no further acknowledgments at this time.