
Abstract
OBJECTIVE:
To evaluate the efficacy of gastric lavage (GL) in preventing feed intolerance in babies born through Meconium stained amniotic fluid (MSAF).
STUDY DESIGN:
In this randomized trial conducted at a tertiary care hospital, neonates born of MSAF after 34 weeks period of gestation requiring routine care were randomly allocated to GL with 10 ml/kg of normal saline. The control group did not receive GL. The subjects were monitored for first 24 hours in predefined time epochs. The primary outcome was incidence of feed intolerance which was defined as vomiting or abdominal distension more than 2 cm from baseline measure. Babies were also monitored for potential adverse events due to GL and total duration of hospital stay.
RESULTS:
Baseline parameters were comparable. The incidence of feed intolerance was not significant in the GL group [4.6% vs 9.2%; RR 0.92 (0.29–3)]. There were no adverse events secondary to GL. The duration of hospital stay was comparable between groups.
CONCLUSION:
GL in neonates born of MSAF does not reduce feed intolerance.
Introduction
Meconium is a blackish-green sticky material composed of debris of intestinal cells, lanugo hair, vernix, liquor and bile pigments [1, 2]. Its passage being a developmentally programmed event that occurs postnatally, 98% of healthy newborns pass Meconium within the first 48 hours and for the same reason, most of the cases of Meconium stained amniotic fluid (MSAF) are noted in newborn deliveries at or following 37 weeks of gestation [3, 4].
With a reported incidence of 5.6% to 24.6%, a proportion of infants born through MSAF may swallow Meconium and develop vomiting, retching and possible secondary aspiration due to the chemical irritant effect of Meconium on the gastric mucosa [5]. Such feeding problems are 2.8 times more frequent in neonates born with MSAF, regardless of the consistency of Meconium [6]. Performing gastric lavage (GL) soon after birth could potentially reduce the risk of these complications. However, such a routine practice is not without its attended potential complications such as bradycardia, apnea, vomiting, aspiration, trauma and a slight elevation of blood pressure [6, 7].
Some of the earlier published RCTs on this subject have found beneficial effects of GL [8], while others have not [9–13]. Most of these studies had risk of biases which was confirmed in recent meta-analysis on this subject, which was published after commencement of the present study [14].
With an increase in prevalence of intrauterine growth restriction, perinatal asphyxia, post term pregnancy in the developing nations, the rates of MSAF are higher in these regions where in also exists limitation of resources. Thus establishing the need for GL would translate in optimization of resources and patient outcome. In view of these, the present RCT was designed to assess the need for GL in near term and term babies born of MSAF in reducing the incidence of feed intolerance.
Methodology
Subjects and settings
We conducted this randomized controlled trial from February 2015 to August 2016 at the Command Hospital, Pune. We enrolled term and near term neonates born of Meconium stained amniotic fluid (irrespective of consistency) not requiring resuscitation at birth, when the principal worker was available to follow up such babies for 48 hours post-delivery. The following babies were excluded: born before 34 weeks period of gestation, requiring NICU admissions and those with major congenital malformations. The gestational assessment of the enrolled subjects was calculated from the first day of last menstrual period if mother was sure of dates; else, antenatal ultrasonogram conducted in the first trimester or neonatal assessment by expanded new Ballard score were considered. Parental informed written consent was taken prior to the inclusion of the study subjects and approval from the institutional ethics committee was obtained. The trial was registered with clinical trials registry of India (CTRI/2016/12/007524).
Randomization and blinding
The study subjects were randomly allocated to either of the groups based on the random sequence generated by computer which was done by the statistician who had no direct role in the further conduct of the study. The type of intervention (GL or routine care) was mentioned in a separate chit which was put in a double sealed opaque envelops. Sequential numbers of the study participants was written on envelops. Envelops were kept in the labor room of the hospital. The principal worker and the consultant in charge of the post natal ward were blinded to the type of intervention. The code of intervention was revealed to the investigators only after completion of the study.
Intervention
On the delivery of a neonate born of MSAF, the principal worker was informed telephonically about the case. If it met the inclusion criteria and the principal worker was available for next 48 hours for follow up, the instructions were given to the attending duty doctor/ duty nurse to open up the envelope after taking informed consent of the parents and perform the prescribed intervention. The principal worker was blinded to the nature of intervention.
If the intervention involved no GL, the baby was handed over to the mother. Breast feeding was encouraged and the first feed to the baby was ensured as soon as possible or atleast within the first half an hour. If for some reason, the breast feeding was not feasible within the given time, top feed was administered and reasons for inability to breastfeed were sought and suitably corrected.
For GL, the duty nurses at the labor room and the attending resident doctors were well instructed about the procedure to be performed and the same was ensured at regular intervals during the period of the study. Suitable charts depicting the procedure to be performed were placed at the delivery suite.
GL was carried out by placing a 8F Nasogastric tube tube after measuring the appropriate length of insertion by measuring the distance from the bridge of the nose to the earlobe and from there to a point between xiphisterum and umbilicus.
The feeding tube was passed along the floor of the nose. In case of difficulty it was tried in another nostril. If the baby gagged or the tube coiled up in the mouth, the tube was withdrawn partly and again it was passed and inserted up to the measured length. It was fixed after confirmation of its proper placement in a butterfly fashion. Confirmation of the proper placement of nasogastric tube was done by “Whoosh Test” where air was injected in the tube, while auscultating the epigastric area, thus confirming its position in the stomach.
GL was carried out by using 10 ml per Kg of normal saline or till the aspirated fluid was clear of meconium. Attempt was made to remove as much of normal saline as possible after this procedure. Post procedure, feeding was attempted as described before.
Outcomes and measurements
The details of patient particulars which included gestation, birth weight, delivery details, Apgar score, type of feed, timing of first feed were noted by the principal worker and they were followed up at 12 hourly intervals for episodes of vomiting till discharge. Feed intolerance was defined as vomiting and or abdominal distension more than 2 cm from the baseline measure. Vomiting was defined as forceful expulsion of milk with effort which occurred after feeding consisting of milk, bile or Meconium. The episode was confirmed by the duty nurse, who recorded the same and differentiated it from regurgitation, which was defined as effortless expulsion of small quantity of milk or curdled milk occurring after feeding.
The babies were also followed up for clinical features of respiratory distress due to Meconium aspiration syndrome, other effects of GL (apnea, bradycardia, local trauma, aspiration). The duration of hospital stay at the time of hospital discharge was noted.
Statistical analysis
The data was entered in Microsoft excel sheet (Microsoft, Redmond, CA). Data analysis was done using Stata 11.0 (Stata Corp, College Station, TX). Continuous data with normal distribution were analyzed by Student’s t-test, whereas non-normally distributed data were analyzed by Mann–Whitney U test. Categorical data were analyzed by Fisher exact/chi-square test. P value of <0.05 was taken as significant. Based on a previous study the incidence of vomiting in the neonate born through meconium stained amniotic fluid was 30% [9]. We expected a 50% reduction of vomiting following GL. To detect this difference between the two groups with power of 80% and p value of 0.05, sample size of 224 was calculated.
Results
Out of 3623 deliveries that occurred during the study period, 486 babies (13.4%) were born through meconium stained amniotic fluid. Of these, 224 patients were enrolled sequentially as per the study criteria and allocated to the two treatment groups. Amongst the babies excluded, the main reasons were: PW not available for assessment of primary outcome (n = 162), babies born at gestational age less than 34 weeks (n = 122). The details of trial flow are depicted in Fig. 1.
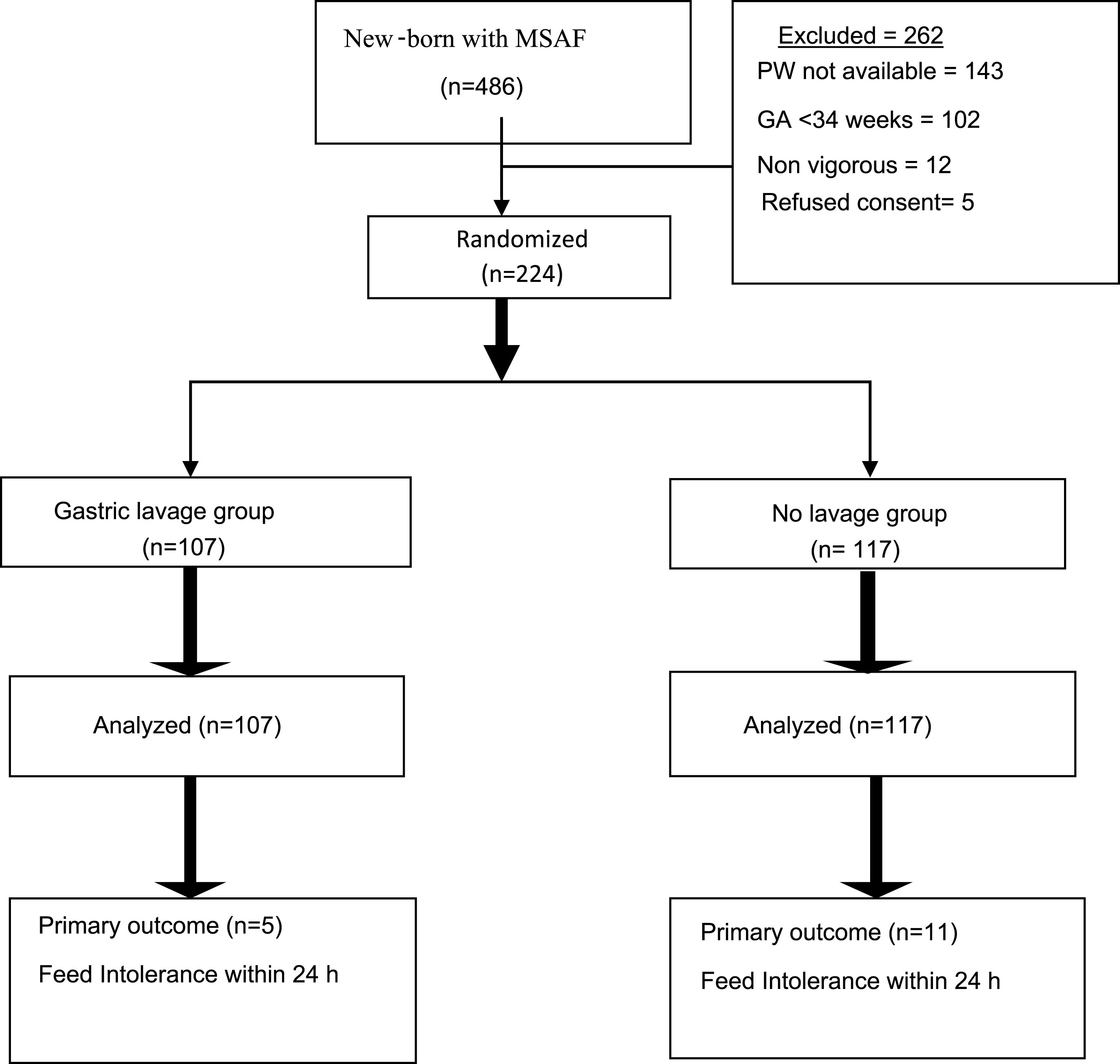
Study Flow. MSAF: Meconium stained amniotic fluid.
The baseline variables were comparable between the study groups (Table 1). The overall feed intolerance occurred higher in the no-lavage (9.2%) than the GL group (4.6%), though this was statistically not significant [RR 0.92 (0.29–3)]. When analyzed as per time epochs, maximum such episodes occurred between 2–12 hours and were not statistically significant. None of the babies in either group had any significant abdominal distension or any complications related to the procedure of GL such as nasal trauma, apnea, bradycardia or any event necessitating intensive care. The duration of hospital stay also matched between the groups (Table 2).
Baseline variables of the study groups
Outcome of the study
Our study demonstrates that GL does not significantly reduce incidence of feed intolerance amongst babies born of MSAF, though the trend (4.6% vs 9.2%) suggests an decrease in chances of this outcome in the intervention group, similar to previous studies [9, 13]. A recent meta analysis on this subject, which was published after the commencement of the present study has shown that GL reduced the incidences of feed intolerance (RR: 0.71 (95% CI 0.55 to 0.93, p = 0.01). However, this beneficial effect was lost when studies with low risk of bias in random sequence generation [RR: 0.81 (0.60 to 1.09)] or allocation concealment [RR: 0.66 (95% CI 0.43 to 1.03)] were considered. None of the studies had reported any adverse events related to the procedures, mortality or duration of hospital stay [14]. The results of our study are similar to those reported in the meta analysis.
The strengths of our study are a robust study design that was conducted at a tertiary care center, registered with CTRI, India. Our study adds to the existing evidence on the subject, despite the fact that the meta analysis suggested that a total number of 3000 neonates born of MSAF would need to be enrolled to answer the research question, suggesting a multicentric trial. The main weakness of our study was its limited follow-up only for 24 hours. Besides, we did not assess the effects of consistency of meconium stained liquor with respect to the outcome - as previous studies have not found it as a significant factor for the outcomes [6]. Though major plausible side effects of GL were monitored, we did not objectively document other associated physiological effects such as changes in arterial blood pressure or disruption in feeding behavior.
To conclude, our study has demonstrated that routine gastric lavage in vigorous babies born through MSAF for prevention of early feed intolerance is not required in contrast to the current practice at many centers. Feeding problems are observed in only a small proportion of all vigorous neonates born through meconium stained amniotic fluid and are usually self-limited. Performing GL routinely in all infants born through MSAF might also delay initiation of breast-feeding and mother-infant bonding, besides the procedure itself being time consuming, involving human and material resources. Importantly, this procedure does not prevent or reduce the incidence of feeding problems or secondary meconium aspiration and hence should not be performed in these infants.
Conflicts of interests
None to declare.
Funding
Nil.