
Abstract
BACKGROUND:
The optimal thresholds for identification of preterm infants at greatest risk for adverse sequelae related to patent ductus arteriosus have not been well delineated. Our aim was to determine hemodynamic parameters in the first 24 hours using continuous non-invasive vital and structural measurements to predict which infants required PDA treatment in our institution.
METHODS:
Retrospective secondary analysis of data from infants born 23 to 32 weeks gestational age with cardiac output and stroke volume via electrical cardiometry, cerebral tissue oximetry measurements, mean arterial blood pressure (BP), heart rate, and oxygen saturation and functional echocardiography results at 12 hours of life were recorded when available (93 percent of subjects).
RESULTS:
A total of 292 infants, of which 55 (26±2 weeks, 862±268 grams) were treated for PDA. Treated infants demonstrated increased left ventricular output (p < 0.001) and lower mean BP (p = 0.010). The optimal area under the receiver operating characteristic curve (AUC) for predicting PDA treatment in our all gestations cohort is a mean BP at 15 hours of life of <33 mm Hg (AUC = 0.854, p < 0.001, 95% CI 0.792, 0.916). For infants <28 weeks a mean BP at 13 hours of life of <33 mm Hg (AUC = 0.741, p < 0.050, 95% CI 0.642, 0.839).
CONCLUSIONS:
In our cohort increased left ventricular output and lower mean BP predicted a clinically significant PDA requiring treatment.
Keywords
Abbreviations
patent ductus arteriosus
hemodynamically significant patent ductus arteriosus
intraventricular hemorrhage
N-terminal of the prohormone brain natriuretic peptide
near infrared spectroscopy
tissue oxygen saturation
stroke volume
cardiac output
left ventricular output
blood pressure
peripheral arterial oxygen saturation
Neonatal Intensive Care Unit
area under the receiver operating characteristic curve
Introduction
Early-targeted treatment of patent ductus arteriosus (PDA) in preterm infants continues to be a highly debated topic. Even though the PDA has a greater association with morbidities such as necrotizing enterocolitis, intraventricular hemorrhage (IVH), and bronchopulmonary dysplasia in preterm infants, there is still hesitancy by clinicians as to whether they should treat a PDA. Controversy surrounding the treatment of PDA’s in preterm neonates is based on the lack of consensus regarding the definition of a hemodynamically significant PDA (hsPDA) [1]. Many previously published trials did not have criteria for treatment [2], and trials looking at very early treatment (first 24 hours) have different definitions for treatment criteria [3–6]. The most common criteria used for hsPDA is the presence of at least two of the following parameters: Left atrial/aorta at aortic valve ratio of more than 1.4:1, left ventricle/ aorta at aortic valve ratio of more than 2.1:1, and narrowest ductal diameter >1.5 mm [1]. The optimal threshold for the identification of infants at greatest risk for adverse sequelae has not been well delineated. While several studies of early functional echocardiography have been predictive of which infants have required treatment, the use of early-targeted neonatal echocardiography continues to remain limited in the United States [3].
While there is evidence that prophylactic treatment of PDA can reduce significant morbidities such as IVH [7, 8], this data is now complicated by evidence of high rate of spontaneous closure of PDA’s with lack of significant morbidity [9–12]. Current studies of the N-terminal of the prohormone brain natriuretic peptide (NT-proBNP) or troponin T at 48 hours of age may help predict death or severe IVH as well as neurodevelopment at 2 years of age but are not helpful in “real time” guidance of early targeted treatment [13, 14]. Changes in hsPDA have been shown to correlate with changes in BNP concentrations but the sensitivity of NT-proBNP still remains weak. There is also significant overlap in ranges of NT-proBNP concentrations between neonates with and without PDAs [3, 15].
Other non-invasive measures such a near infrared spectroscopy (NIRS) and electrical cardiometry have also been explored [16, 17]. NIRS is a noninvasive diagnostic tool that has been used to measure tissue oxygen saturation (StO2) in cerebral and renal tissue to diagnose PDA in premature infants. The presence of a hsPDA has been correlated with lower regional cerebral StO2 and higher fractional tissue oxygen extraction supporting the hypothesis that prolonged ductal patency may have a causal role in substantial and enduring adverse outcomes [16]. Electrical cardiometry is a method of measuring changes in conductivity to determine stroke volume (SV), cardiac output (CO), and other hemodynamic parameters. Studies using electrical cardiometry to measure SV and CO in hemodynamically stable preterm infants were comparable to echocardiography [17].
The purpose of this study was to determine hemodynamic parameters in the first 24 hours using continuous non-invasive vital and structural measurements to predict which infants would develop clinical and echocardiographic criteria for PDA treatment in our NICU.
Design/Methods
This is a retrospective secondary analysis of data from infants born 23 to 32 weeks gestational age. A blinded echocardiogram was performed by a research sonographer (RN) or the PI (AK) using the Vivid E9 cardiovascular ultrasound system with a 12S phased array transducer (GE Medical System Milwaukee, WT) in the first 12 hours of life (6:09 HOL±3:40) as part of prior research protocols [18, 19]. Left ventricular output (LVO) was measured by obtaining the vessel diameter from the parasternal long axis window and VTI from the apical window. Angle correction was applied in this view if the angle of insonation was greater than 10 degrees from the Doppler angle and the outflow tract. Right ventricular output (RVO) was measured by obtaining the vessel diameter and the velocity from the parasternal long axis window in the sagittal plane. Superior vena cava (SVC) flow was measured by obtaining the vessel diameter from the parasternal long axis window in a sagittal plane and the VTI from the subcostal window. The VTI from 10 consecutive cardiac cycles for all measurements were obtained and values were averaged.
The ductus arteriosus was imaged from the high parasternal window with the transducer angled to obtain a view of the ductus throughout its course from the pulmonary artery to the descending aorta. The direction of flow was assessed by placing the pulse wave Doppler range gate in the center of the ductus and recording the flow pattern by spectral Doppler. The direction of flow was categorized as all left to right, all right to left, or bidirectional. If bidirectional, the percentage of right to left flow was calculated by measurement of the time of right to left component over the time of the entire cardiac cycle.
The information from the scans was solely for research and not made available to the clinical team. These methods have been previously described [20]. All images obtained were analyzed and measured offline using EchoPAC software (GE Medical System Waukesha, WI, version 2.0). Subsequent echocardiograms for clinical care were only performed if the infant developed a murmur, persistent hypotension (defined as arterial BP less than gestational age) or significant metabolic acidosis (base deficit > –7).
The CO and SV were obtained using electrical cardiometry (Cardiotronic, La Jolla, CA, iControl software ver 1.0, averaging cardiac measurements every 30 seconds) and StO2 measurements using NIRS (FORE-SIGHT, Casmed, Branford, CT, data acquired through VGA output). Mean arterial blood pressure (BP), heart rate, and peripheral oxygen saturation (SpO2) were recorded from the bedside monitor in the Neonatal Intensive Care Unit (NICU) until 24 hours of life. All data was acquired at 2 second intervals. The StO2 monitoring was achieved by standardized placement of NIRS on the forehead. The CO and SV were obtained via four sensors placed on the head and thorax. Cardiometry and NIRS monitors were placed as soon as possible after NICU admission until 24 hours of life. The recordings were transferred to a secured server accessed only by research staff. The clinicians were blinded to the NIRS, CO and SV data. Averages of the physiologic data parameters for each hour of life were derived for each subject.
Infants that subsequently went on to receive a clinically indicated echocardiogram and treatment for a PDA were compared to those that did not receive treatment. The criteria for treatment included presence of a moderate to large PDA (ductal diameter >1.5 mm) along with clinical symptoms such as significant ventilator support, metabolic acidosis or persistent hypotension. Data analyses were performed using SPSS (Version 22.0) for Windows (IBM, Armonk, New York). The level of statistical significance was established prior to analysis as a P value of <0.05. Descriptive analyses were used to evaluate frequencies and distributions of variables and potential outlier values. Scatterplots were examined to evaluate assumptions of normality, linearity, and homogeneity of variance. The mean and median values were comparable at each level and consistency among standard deviations, suggesting the use of parametric methods for subsequent analyses. Additional post hoc confirmation regarding appropriate use of the measure of central tendency for the 3 values was conducted using non-parametric testing (Kruskall-Wallis and median tests), and these tests led to similar statistical conclusions regarding acceptance or rejection of null hypotheses. Two tailed student T tests were used to compare the overall mean values per hour of heart rate, BP, StO2, SpO2, CO, and SV between preterm treated and untreated subjects. Receiver operating characteristic curves were generated for the entire cohort to evaluate the mean BP for each of the first 24 hours and PDA requiring treatment.
Results
A total of 292 infants were included of which 55 were treated for PDA either pharmacologically (n = 52) or surgically (n = 3). Treated infants were more immature, smaller, and more likely to have low Apgar score, necrotizing enterocolitis, receive a fluid bolus or vasopressors, and be on oxygen at 36 weeks corrected gestational age (p = 0.001, Table 1). The mean time to medical and surgical treatment was 6.97±6.8 and 13.3±8.1 days respectively. In the 93 percent of infants with an early functional echocardiogram there was an increased LVO in treated infants, but no differences in other outputs or ductal diameter (Table 2). Infants who received treatment for a PDA had lower mean BP, CO, and SV in comparison to the untreated infants (Fig. 1). After adjusting for gestational age and birth weight, only mean BP remained significant (p = 0.010). The optimal area under the receiver operating characteristic curve (AUC) for predicting PDA treatment in our all gestations cohort is a mean BP at 15 hours of life of <33 mm Hg, with a sensitivity of 66% and a specificity of 90% (AUC = 0.854, p < 0.001, 95% CI 0.792, 0.916) (Fig. 2). For infants <28 weeks a mean BP at 13 hours of life of <33 mm Hg predicted clinical symptoms for necessitating PDA treatment. (AUC = 0.741, p < 0.050, 95% CI 0.642, 0.839) (Fig. 3).
Demographics
Demographics
Echocardiogram results

Hemodynamic changes in the first 24 hours in infants that developed patent ductus arteriosus requiring treatment compared to those that did not require treatment.
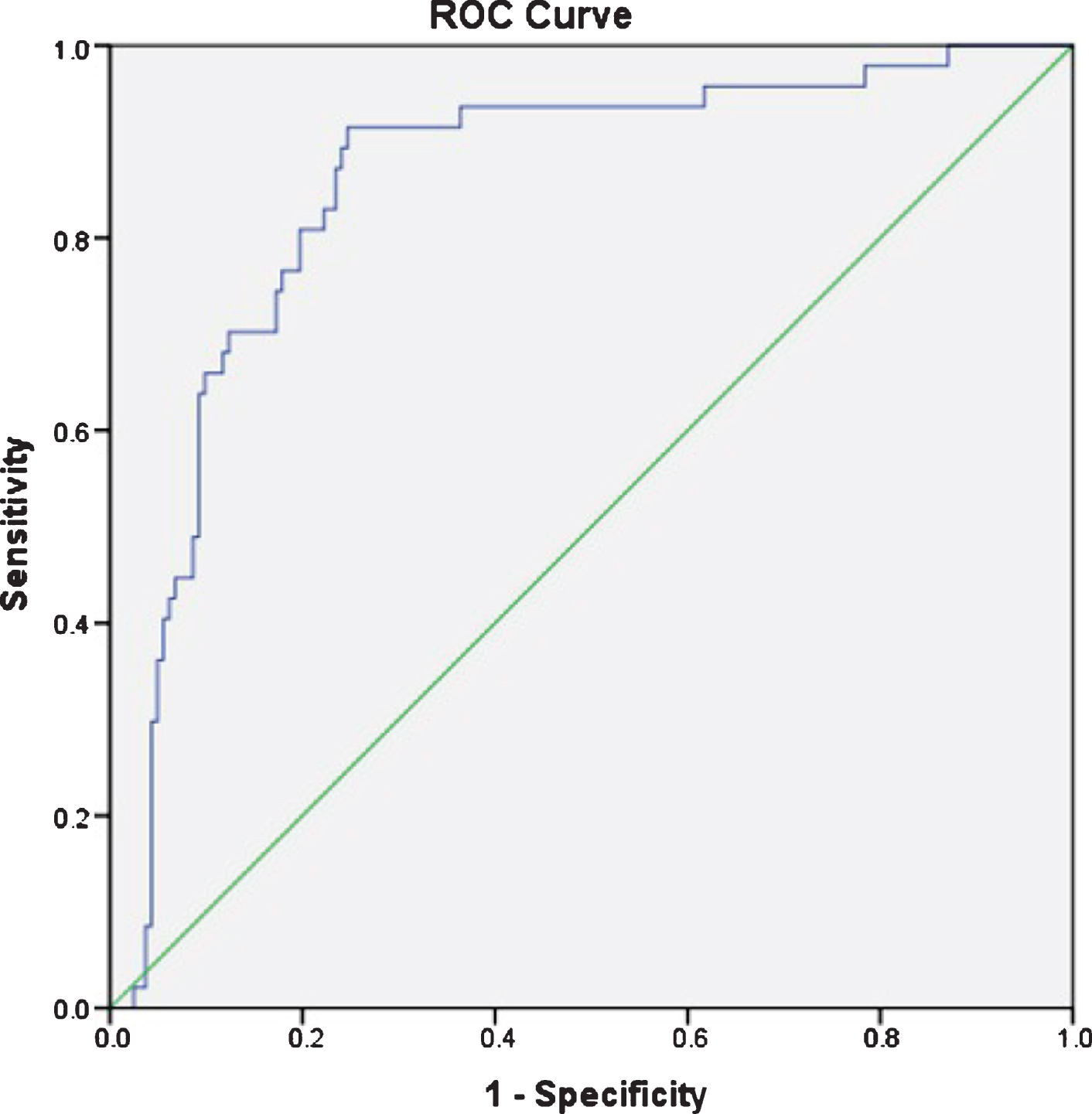
Receiver operating characteristic curve for mean blood pressure <33 mm Hg at 15 hours of life for all subjects.
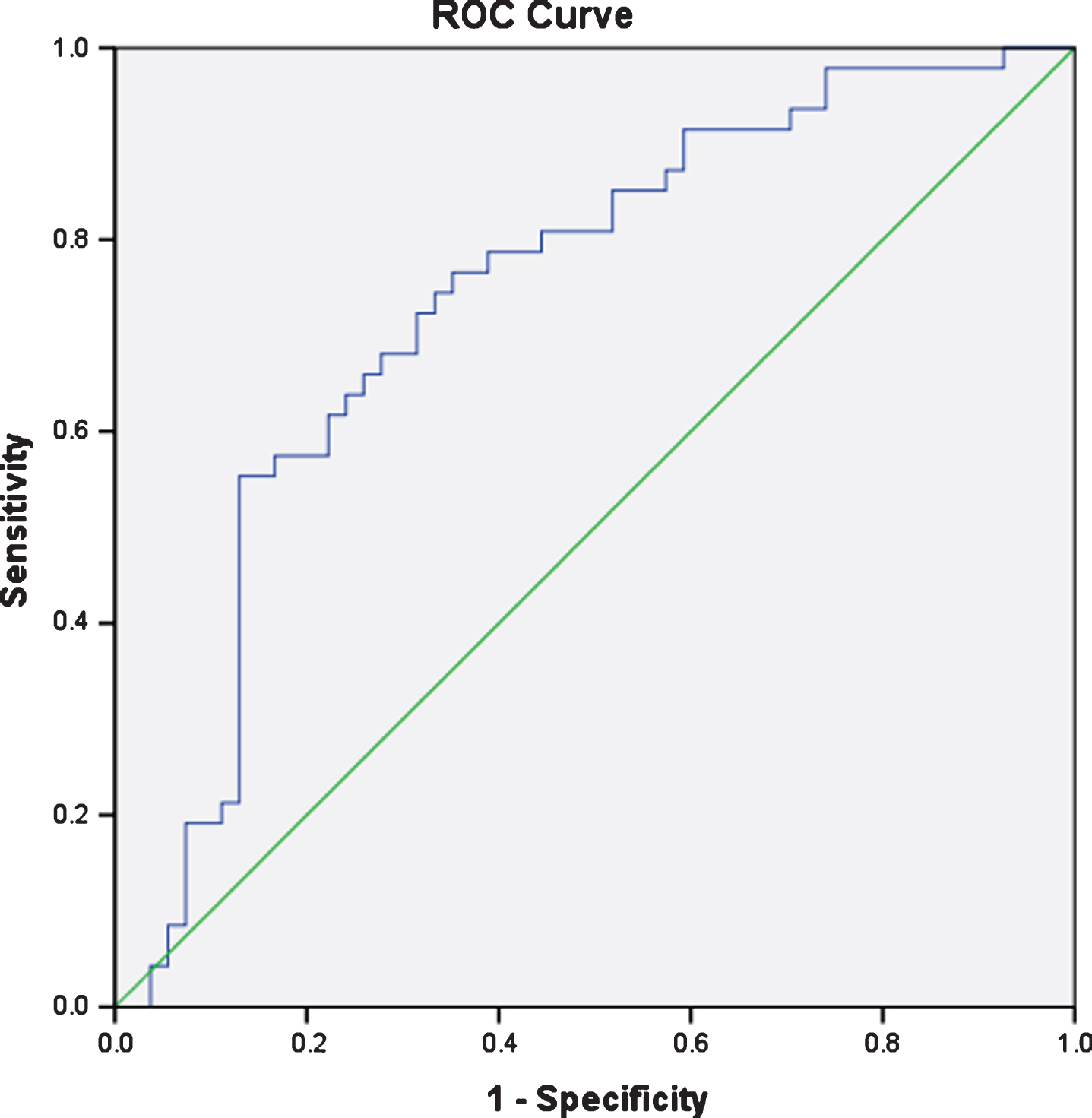
Receiver operating characteristic curve for mean blood pressure <33 mm Hg at 13 hours of life for subjects <28 weeks gestational age.
Diagnosis and treatment of hsPDA remains a challenge. The efficacy of pharmacologic treatments is much higher when giver earlier [21], however given that a large number of PDAs close spontaneously, clinicians would prefer to only treat those that are likely to remain persistently open. We compared prospective data such as electrical cardiometry and NIRS, as well as physiologic parameters from the patient bedside monitor, to predict whether a premature infant would receive pharmacological or surgical treatment for PDA. In this cohort, increased LVO and lower BP in the first 24 hours were associated with development of a PDA requiring treatment.
Echocardiography has been the gold standard for direct assessment of PDA diameter and shunt pattern but inter-observer variability can create discrepancies in measurements taken [3]. Standardization of diagnosing PDA via echocardiography was attempted using ductal staging by Sehgal et al. [22]. Individual parameters of ductal features (Transductal diameter and ductal velocity), magnitude of ductal shunts, and features of myocardial performance (E/A ratio and isovolumetric relaxation time) were graded from 1 to 3 depending on the magnitude of severity. Of these parameters, ductal diameter was the most important factor for determining therapeutic intervention [23]. It has been shown that ductal diameter greater than 1.5 mm at a mean of 19 hours after birth predicted later clinically apparent PDA that required treatment in a cohort of extremely premature, ventilated newborns [24]. The mean time for our scan was 6 hours. We did not find a difference in the ductal diameter in our cohort, and this may be due to the earlier timing of our scans. While we demonstrated that infants that required treatment had lower cardiac output and stroke volume by electrical cardiometry than non-treated infants, this association was no longer present when we adjusted for birth weight. However, we did demonstrate an increased LVO (milliliters per kilogram per minute) at 6 hours in infants that developed a clinically significant PDA. An increased LVO does correlate with a significant ductal shunt [25]. The largest limitation of any echocardiographic measurements is that extensive training is required before these measures can be obtained in a clinical setting [22].
NIRS is a noninvasive tool with which the regional StO2 of the underlying tissue can be measured. While NIRS was lower in infants requiring PDA treatment, there were no differences in NIRS once we adjusted for gestational age and birthweight. The data on NIRS is variable which can be influenced by the timing and location of the NIRS when evaluating the PDA. Chock et al., [16] studied 35 infants <29 weeks gestational age with hsPDA compared to a non-significant PDA and found cerebral StO2 was not significantly different, but found a lower renal StO2. Lemmers et al., studied 20 infants <32 weeks gestational age diagnosed with PDA at 41 hours of life (range: 17–76 hours) treated with Indomethacin case matched to infants without PDA. Infants with PDA receiving treatment had significantly lower cerebral StO2 62±9% compared to infants without PDA 72±10% (P < 0.05) [26]. A recent study utilizing cerebral and renal NIRS in preterm infants and a postnatal age of 77 hours (IQR:70–107) did not show any difference between infants with a hsPDA, non-hsPDA and no PDA [27]. Cerebral NIRS may be limited by the presence of cerebral autoregulation, whereas abdominal NIRS may be more affected by a late significant PDA [16]. Although promising, NIRS and Electrical Cardiometry are understudied and were not clinically significant in determining hsPDA in our study.
Arterial hypotension due to a PDA may be a reasonable marker to determine whether an infant requires treatment. A recent comparison of two different treatment strategies of prophylactic indomethacin compared to withholding treatment until at least the first week demonstrated a lower incidence of a moderate to large PDA a 1 week of age, less vasopressor-dependent hypotension, and less need for respiratory support compared with the conservative treatment approach [23]. This data along with our study suggest that an early-targeted treatment may not only decrease the incidence of an early PDA in this population, but may also help with other comorbidities. In our cohort, a mean BP at 15 hours of life of <33 mm Hg had a sensitivity 66% and specificity of 90% for predicting PDA treatment. While a mean BP of 33 may seem high for our cohort, several studies suggest that this may not be the case. While targets for treatment for hypotension may be based on gestational age [28], the majority of newborns will achieve a BP target of 33 by 15 hours of life [29]. Lemmers et al found infants with a hsPDA identified at mean 41 hours of life had a lower mean BP 33±5 mm Hg as compared to infants without a PDA 38±6 mm Hg (P < 0.05) and mean BP remained significantly lower 6 hours after the start of Indomethacin treatment [26]. Other cohort studies have looked at hour specific norms in extremely low birth weight (600 grams) infants with mean BP of 32 and 34 and 6 and 12 hours respectively [30]. Another cohort study of infants 23–26 weeks showed the mean BP of 33 at 15 hours to be close to the 75 percentile [29].
Our study is limited since these variables were not pre-specified outcomes from our prospective data collection. However, to our knowledge this data is one of the largest cohorts with detailed early hemodynamics. We also realize that our criteria for treatment for PDA may be different than other institutions so our data may not be generalizable to all centers. Future studies are needed with hour specific blood pressure targets for early PDA treatment.
Funding source
None.
Conflict of interest
The authors do not report any conflicts of interest.
Financial disclosure
There are no financial disclosures to report.