
Abstract
BACKGROUND:
Despite widespread implementation, limited data exists relating morbidity or adverse outcomes to Car Seat Tolerance Screen (CSTS) result in preterm and low birth weight (LBW) neonates. The objective of this study was to determine longer term post-discharge outcomes of infants who failed a CSTS.
METHODS:
We performed a case control study evaluating outcomes of infants born over one year who failed vs. passed an initial CSTS, utilizing both retrospective medical record review and parental survey data 2–3 years after discharge. Subjects were matched one case of failed CSTS to two controls who passed CSTS based on sex, gestational age, and BW. We performed bivariate analysis of clinical and demographic risk factors comparing those who passed vs. failed CSTS.
RESULTS:
We identified 19 subjects who failed and matched to 37 controls. Cases were significantly more likely to be diagnosed with obstructive sleep apnea (p = 0.027), asthma (p = 0.016), and be treated with albuterol (p = 0.008). We did not find differences in frequency of urgent care visits or hospital admissions between the groups. Although more of the cases were noted to have developmental delays, the difference was not statistically significant.
CONCLUSION:
This is the first study to evaluate longer term post-discharge outcomes of subjects having undergone CSTS. Subjects who failed CSTS had significantly increased incidence of respiratory diagnoses such as OSA and asthma than matched controls by 2–3 years after discharge. Larger studies are necessary to further evaluate these findings, but this does provide data that CSTS may be useful in identifying at risk neonates.
Introduction
Numerous studies have shown that preterm infants are at risk of oxygen desaturation as well as bradycardic events when placed in the semi-upright position in a car safety seat [1–3]. Because of this, the American Academy of Pediatrics (AAP) has recommended performing a Car Seat Tolerance Screen (CSTS) prior to discharge for all preterm infants [4]. This period of observation to assess for desaturation, bradycardia, and apneic events is intended to identify those infants who are not safe to be discharged home traveling in a car safety seat. There is growing data on incidence and predictors of CSTS failure in preterm infants [5, 6], but limited data exists on what a failed CSTS means for the overall health of these neonates.
In addition to preterm infants, infants born low birth weight (LBW, <2.5 kg) have been shown to have poor fit in the car seat [7]. Though testing LBW term infants is not a formal AAP recommendation, the AAP does note in their policy that “important considerations for transportation of preterm and low birth weight infants” exist [4], leading many hospitals to use LBW as an inclusion criterion for testing [8–10]. Term LBW infants have been shown to have similar incidence of CSTS failure as preterm infants [10].
A major concern related to the CSTS is the lack of long term follow up of infants undergoing the test. Despite widespread implementation, very limited data exists relating morbidity or adverse neurodevelopmental outcomes and CSTS result. A Cochrane Review from 2006 sought to assess whether a pre-discharge CSTS prevents morbidity and mortality in preterm infants [11]. They found no randomized controlled trials that evaluated the diagnostic utility of the CSTS and therefore concluded it is unclear whether performing a CSTS is beneficial or could lead to harm related to adverse consequences surrounding discharge assessment [11]. They noted that no data exists to accurately predict that an infant who fails their CSTS will go on to experience clinically significant adverse cardiopulmonary events in the car seat. In fact, due to this lack of evidence, the Canadian Paediatric Society changed their position and stopped recommending routine CSTS testing in 2016 [12].
Additional research is clearly needed to assess the correlation between CSTS failure and future adverse cardiopulmonary events, neurodevelopmental outcomes, and effects on health care utilization. The objective of this study was to determine longer term post-discharge outcomes of infants who failed a CSTS. We hypothesized that infants who failed a CSTS would have increased incidence of urgent care visits or readmissions for respiratory complaints than those who passed.
Methods
We performed a retrospective medical record review and case control study of infants born between January 1, 2013 - December 31, 2013 who were admitted to either the NICU or the newborn nursery (NBN) at the University of Maryland Children’s Hospital, and who qualified for CSTS. We have a birth/admission rate of ∼1600–1700 annually. At our institution, all neonates born preterm (<37 weeks gestational age, GA) or LBW qualify for CSTS testing. At the time of this study, failure of CSTS was defined as a desaturation event <88% , bradycardic event <80, apnea >20 seconds, or respiratory distress in the car seat.
This study was approved by our Institutional Review Board (IRB). Inclusion criteria included infants who qualified for CSTS. Exclusion criterion was death prior to CSTS performance. We chose subjects born in 2013 so that they would be at least 2–3 years of age at the time of our study, allowing for time to have identified comorbidities that could be associated with CSTS result.
Those infants who failed their initial CSTS were considered the cases and those who passed were considered controls. Cases and controls were determined via retrospective medical record review of infants admitted to our institution in 2013. We attempted to match two controls to each case based on: 1) sex, 2) birth GA, 3) birth weight. We attempted to match GA within one week and birth weight within 100 grams. We evaluated demographic and clinical characteristics such as race, small for gestational age (SGA) status, gestation number, amount of prenatal care (PNC) received, mode of delivery, Apgars, medication exposure, ventilator requirements, bronchopulmonary dysplasia (BPD) diagnosis, characteristics at the time of CSTS (such as age, weight), and discharge medications. We also evaluated the medical record for subsequent problem lists/diagnoses, clinic visits, emergency department (ED) visits, and readmissions. We utilized a regional health information exchange (HIE) in our electronic medical record that provided information on ED visits and admissions from hospitals across the state of Maryland and Mid-Atlantic region to ensure more complete data on follow up. Of note, infants are automatically admitted to our NICU if they are <35 weeks birth GA, <2.1 kg birth weight, or are in any distress.
In addition, we performed a prospective survey of the families of our subjects in 2015–2016. This was approved by our IRB. We attempted to contact a parent/guardian for each subject and obtained verbal consent over the phone for participation. Our survey included questions on: 1) whether their child had spent the night in the hospital and why, 2) whether their child had visited the ED or urgent care or clinic for anything other than a well-child visit and why, 3) if their child has any specific health issues and what those are, 4) medications taken, 5) if their child sees any specialists and why, 6) if their child ever had any difficulty breathing when placed in a car seat, 7) how many non-traveling hours per day their child spends in a seated position (car seats, swings, reclining bouncy seats), 8) if parents recalled the CSTS result of their child, 9) current zip code, 10) enrollment in WIC, 11) any additional information the parent/guardian would like to share with us.
We performed bivariate analysis of clinical and demographic risk factors comparing those who passed vs. failed their CSTS. Continuous, binary, and categorical data were analyzed using T-Test, Wilcoxon Nonparametric Rank Sum, Chi Square, or Fisher Exact Test as appropriate. All analyses were performed using SAS 9.3 (Carey, NC).
Results
In 2013, ∼25% of all births and admissions to our NICU or NBN qualified for CSTS with an overall failure rate of ∼5% . We identified 19 subjects who failed their CSTS in 2013, 13 preterm and 6 term LBW. Eight of the preterm subjects were born <34 weeks. One of the cases could only be matched with a single control based on our criteria so we had a total of 37 controls who passed an initial CSTS. Another case was matched with one control >100 grams from the BW. The case subject was late preterm at 36–0/7 weeks weighing 3625 g who had one control meeting our matching criteria and one who was 36–3/7 with BW 3260 g. A third case could not be matched with both controls within one week of GA – this case was a 2060 g 33–6/7 weeker who had one control who was 8 days more mature at 35–0/7 weeks with BW 1970 g. The remaining cases were matched with 2 controls within 100 grams of BW and 7 days of birth GA. Despite one missing control and two controls who strictly only met two of the three criteria, we found that the groups were well matched [Table 1].
Baseline characteristics of infants who failed vs. passed initial CSTS
Baseline characteristics of infants who failed vs. passed initial CSTS
CSTS, car seat tolerance screen; GA, gestational age; PMA, postmenstrual age.
We found no differences in baseline characteristics between those who passed vs. failed an initial CSTS based on race, mode of delivery, Apgar scores, medications (antenatal steroids, surfactant, caffeine treatment, or postnatal steroids), SGA status, BPD diagnosis, respiratory support requirements, intraventricular hemorrhage, or location of admission (NICU vs. NBN). We did find that those who failed were more likely to be multiples, to have been exposed to maternal general anesthesia, and have inadequate PNC (limited, late, or none). [Table 1] We found no differences between the groups at the time of the CSTS based on age, weight, or postmenstrual age (PMA).
We were able to perform a medical record review on all subjects and were able to directly contact a total of 19 families (7 of the cases and 12 of the controls), or 33.9% of the cohort (36.8% of cases and 32.4% of controls) for follow up information in addition to our chart review. One of the case families was unable to complete the full survey and did not give information on CSTS result or WIC enrollment. All of the remaining parent/guardians were aware of the correct initial CSTS result but one. This subject failed their initial CSTS, but the parent reported remembering that the infant had initially passed. Families involved in our survey noted similar time spent in the car seat/semi-upright position (while not traveling) regardless of initial CSTS result [Table 2]. Of note, one subject spent up to 7 hours daily in the seated position, and this was the subject whose parent incorrectly identified their child as having passed an initial CST. Two of the subjects who passed initial CSTS were noted to spend 2 or more hours daily in the car seat. No family was aware of any difficulty breathing while in the car seat position.
Average time spent in car seat/semi-upright position daily per parental report
CSTS, car seat tolerance screen.
We did not find any differences in number of ED visits or inpatient admissions to the floor or PICU. Both groups had median number of ED visits of 1 with a range of 0–6 in the group who failed and 0–7 in the group who passed. Both had a range of 0–2 visits for cardiopulmonary complaints. Those who failed CSTS had a median of zero admissions with a range of 0–1 floor admissions and 0–2 PICU admissions. Those who passed similarly had a median of zero admissions with a range of 0–3 floor admissions and 0–1 PICU admissions. There were no significant differences in terms of neurologic issues, environmental allergies, cardiac diagnoses, gastroesophageal reflux (GER), or genetic disorders between those who passed vs. failed (Table 3). We were able to verify all parental reports of neurologic, cardiac, and genetic diagnoses via chart review. Although the incidence of developmental issues was higher in those who failed, the differences were not statistically significant. We did find that those who failed their initial CSTS were significantly more likely to be diagnosed with obstructive sleep apnea (OSA) and asthma/reactive airway disease (RAD) than those who passed (p = 0.0274 and p = 0.0162 respectively). Those who failed were more often prescribed albuterol (p = 0.0079) and had a trend towards increased prescriptions for inhaled steroids (p = 0.0652). Of note, the 3 subjects diagnosed with OSA include 2 preterm infants (birth GA 32–6/7 and 31–6/7) and one term LBW infant.
Medical and developmental outcomes per record review and parental report
CSTS, car seat tolerance screen; GE reflux, gastroesophageal reflux; MCHAT, modified checklist for autism in toddlers; NS, not significant; VSD, ventricular septal defect.
In addition, we assessed median household income via zip code for each subject as a proxy of socioeconomic status. [Fig. 1]. We found similar numbers in the lowest and highest income brackets. Though the groups were similar overall, the median income for those who passed was in the $40K – $60K group while the median for those who failed was in the $60K – $80K bracket. More subjects who passed noted receiving WIC benefits (8 of 11 surveyed, or 72.7%) than those who failed (2 of 7 surveyed, or 28.5%).
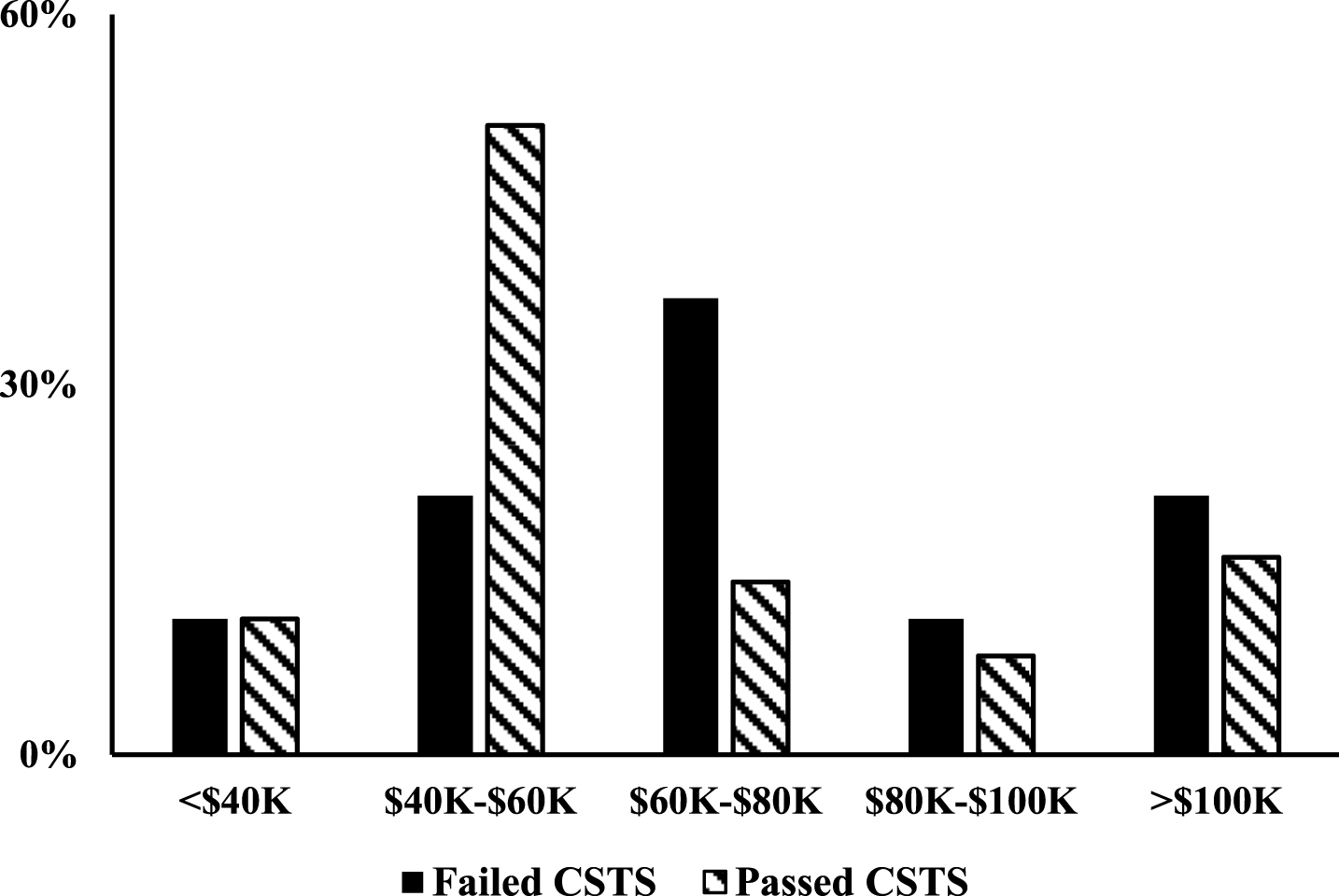
Median Household Income by Zip Code. CSTS, car seat tolerance screen.
In this study, we performed a case control study evaluating longer term outcomes of infants who failed vs. passed an initial CSTS, utilizing both retrospective medical record review and parental survey data. This is the first study to compare post-discharge outcomes of infants who failed CSTS to matched controls who passed. We hypothesized that infants who failed a CSTS would be have increased incidence of urgent care visits or readmissions for respiratory complaints than those who passed. While we did not find this to be the case, we did find that infants who failed their CSTS were more likely to be diagnosed with OSA and RAD/asthma and where more likely to be prescribed albuterol.
The CSTS is a widely implemented yet controversial test. While the goal is identification of safety for discharge in a car seat, the utility of the CSTS to meet this goal is yet unproven. Numerous studies have documented that preterm neonates and those with other comorbidities such as cardiac disease are at increased risk of cardiopulmonary events when placed in a car safety seat [1–3, 13]. However, little data is available on the implications of failure. Shah et al., [9] published one of the rare studies to evaluate outcomes of infants who failed their CSTS. Otherwise healthy preterm or LBW infants at their institution who fail a CSTS in the NBN were routinely admitted to the NICU for observation for 24–48 hrs. Of the almost 150 subjects followed over 6 years, 38% were diagnosed with apnea (including 48% of the preterm and 17% of the term LBW infants). In addition, numerous other comorbidities were diagnosed, including feeding immaturity requiring gavage feeds, immature thermoregulation requiring temperature support, hyperbilirubinemia requiring phototherapy, concern for sepsis requiring antibiotic treatment, hypoglycemia and need for IV fluids [9]. These findings are concerning since the subjects were undergoing routine pre-discharge CSTS from the NBN, were deemed otherwise healthy, and were admitted to the NICU not due to additional clinical concerns but simply due to a failed CSTS. This seems to indicate that the CSTS result is the only factor that helped identify potentially serious comorbidities, many of which required interventions.
In our study, we also identified apnea diagnoses in those who failed their initial CSTS. While Shah et al did not differentiate between central and/or obstructive apnea, our subjects all had obstructive apnea on sleep study. Similar to Shah, we found that both populations (term LBW and preterm) had subjects with apnea. Neck flexion and subsequent upper airway obstruction have been hypothesized as major causes of cardiopulmonary events in the car seat [14–18]. Our subjects diagnosed with OSA all underwent polysomnography while supine, which makes car seat positioning concerning since obstruction is likely exacerbated when placed in the semi-upright position and would explain a failed CSTS.
We also found subjects who failed were more likely to have been delivered to mothers who underwent general anesthesia than those who passed. This is the first time this has been evaluated. We looked at this variable since one hypothesis is that maternal medications could cross the placenta and affect the fetus in utero and subsequently the neonate after delivery. It is possible that the mediations used to anesthetize the mother could affect respiratory drive in the neonate. However, all 3 subjects were preterm and had their CSTS many weeks after delivery, making the likelihood of the anesthetic acutely affecting respiratory drive at the time of CSTS unlikely. Perhaps risk factors related to the mother and why general anesthesia was necessary for delivery are more important factors. This should be included in future studies of CSTS outcome to evaluate if this is in fact a clinically important factor.
We found that those who failed had higher incidence of poor PNC (late/limited or none). There are many hypotheses for why there would be a significant relationship between poor PNC and CSTS failure. Perhaps those with limited access to care due to social or financial issues are more likely to have a car seat that is old or not properly suited to a preterm or LBW infant. However, we check that the car seats are appropriate in all infants prior to testing. Perhaps limited to no care leads to poor estimation of GA and subjects may be more immature at birth than we suspect, potentially increasing risk of failure. Interestingly, those who failed tended to live in a zip code with a higher median income than those who passed and were less likely to report receiving WIC benefits. It is possible that there is a bimodal distribution of risk factors for failure, with one group being those who have less access to care and the other being those with higher incomes who may be more likely to have advanced maternal age and IVF pregnancies, increasing risks. However, this data is limited in that we were able to perform a complete telephone survey on <40% of subjects. It is possible that our results are biased, for example towards subjects in a higher socioeconomic status who could afford a phone. In addition, we did not have data on each families’ income, but used the zip code to assess median income. There are wide ranges of incomes even in one zip code, so this may not completely describe the income of each family.
A strength of our study was that we not only evaluated longer term outcomes of those who failed an initial CSTS, but compared these to sex, birth weight, and birth GA matched controls. Previous studies of the CSTS have either given no data on longer term outcomes or only studied those who failed. One limitation is that this study is relatively small size. However, we wanted to perform this study as a pilot to assess feasibility. In addition, data collected by parents during the survey will help inform a larger study on long term outcomes of subjects undergoing car seat testing. As with any retrospective medical record review, a limitation is accuracy of documentation. We improved the robustness of our data collection by: 1) using the HIE to broaden our search for ED visits and admissions at surrounding institutions, and 2) parental report in our survey.
Conclusions
The objective of this study was to determine post-discharge outcomes of infants who failed a CSTS when compared to sex-, GA-, and birth weight-matched controls who passed. Although we hypothesized that infants who failed would have an increased incidence of urgent care visits or readmissions for respiratory complaints, we found no differences between those who failed vs. passed. What we did discover was those who failed were more likely to be diagnosed with asthma, receive treatment with albuterol, and be diagnosed on sleep study with OSA. This is the first study to evaluate longer term outcomes of subjects having undergone CSTS, obtaining data for 2–3 years after discharge. Additional research is clearly needed to assess the correlation between CSTS failure and future adverse cardiopulmonary events, neurodevelopmental outcomes, and effects on health care utilization. But data from this study can serve as the building blocks for future larger studies on the effectiveness and utility of the CSTS.
Financial disclosure
The authors have no financial relationships relevant to this article to disclose.
Conflict of interest
The authors have no conflicts of interest relevant to this article to disclose.
Footnotes
Acknowledgments
The authors would like to thank the Division of Neonatology for their support.