
Abstract
OBJECTIVE:
To evaluate the effect of oro-and naso- pharyngeal suction (ONPS) on the SpO2 and heart rate (HR) in healthy term newborns delivered by cesarean section, at the first minutes after birth.
PATIENTS AND METHODS:
We conducted a prospective randomized trial. Newborns were randomized to ONPS and No-ONSP groups. Continuous readings of SpO2 and HR were performed during the first 10 minutes, and subsequently at 15, 30 and 60 minutes after birth.
RESULTS:
A total of 84 newborns were evaluated; 42 in ONPS group and 42 in No-ONPS group, with mean gestational age and birth weight±SD of 38.4 weeks and 3533±403 g in the ONPS group and 38.0 weeks and 3575±568 g in the No-ONPS group. The mean SpO2±SD at the first minute of life in the former group was 52.6±7.6% vs 56.1±10.8% on the latter; with no significant difference (p = 0.28). The mean HR±SD at first minute of life was 137±25 in the No-ONPS and 148±13 in the ONPS group (p = 0.02), but no difference was found in the subsequent minutes.
CONCLUSION:
Not performing ONPS in newborns delivered by cesarean section does not affect SpO2 and HR in the first postpartum hour.
Introduction
The transition period after birth in which the fluid in the lung parenchyma and airways must be eliminated to permit the normal lung expansion, is a relatively fast and effective process [1]. Oro and -nasopharyngeal suction (ONPS) is a commonly performed procedure used for the rapid removal of fluid from the upper airway of vigorous and non-vigorous newborns, preventing the aspiration of blood and/or mucus during the first breaths. This may allow a better adaptation to the extra uterine environment [2, 3], but its effectiveness has been questioned in recent years [4].
According to the latest guidelines of Neonatal Resuscitation proposed by International Liaison Committee on Resuscitation (ILCOR) [5] published in 2015, routine ONPS at birth is not recommended and should be restricted to cases of airway obstruction or when Positive Pressure Ventilation is needed [5, 6]. However, these guidelines do not make references to the type of delivery (cesarean or vaginal) and there is insufficient data about the effect of ONPS in infants born by caesarean section [7].
During suction there is a risk of triggering inhibitory reflexes that can alter the normal adaptation of the cardiorespiratory system [1, 8]. Several complications have been described in association with ONPS, such as bradycardia, apnea, decreased SpO2, oropharyngeal mucosal lesions, risk of infection and increased intracranial pressure associated with impaired cerebral blood flow [7–9].
Currently, there is only one study that has explored the effect of immediate ONPS on SpO2 and HR in healthy term neonates born by caesarean section [7].
The hypothesis proposed in the present study is that the absence of ONPS in newborns delivered by elective cesarean section would not have a negative impact on the SpO2 and HR during the first minutes postpartum.
The objective was to evaluate the effect of ONPS on SpO2 and HR in healthy newborns delivered by elective cesarean section, during the first 60 minutes postpartum.
Patients and methods
Study design
This was a controlled prospective randomized trial, carried out in the delivery room of the Guillermo Grant Benavente Hospital in Concepción, Chile; a tertiary referral hospital. The randomization was carried out by using sealed envelopes prior to the delivery. Patients were included within the period stretching from July to October 2012, provided that one of the members of the research team was available to monitor the SpO2 and HR. Informed consent was obtained from one of the parents of each newborn prior to the birth. This study was approved by the Scientific Ethics Committee of the Guillermo Grant Benavente Hospital in Concepción, Chile.
Patients
In this study, we included healthy neonates born by elective cesarean section, with gestational age equal to or greater than 37 weeks, single gestation and without pathological maternal or fetal alterations during the delivery. All the pregnant women received spinal anesthesia for the surgical procedure, maintaining the temperature of the surgical room between 24–26°C. The exclusion criteria were neonates who presented congenital anomalies or chromosomopathies, non-vigorous, amniotic fluid stained with meconium or in those who, based on the antenatal history, anticipated the need for resuscitation. A vigorous newborn was defined as the one with good respiratory effort, normal muscle tone and HR greater than 100 bpm [5]. Infants were randomized into two groups of equal number of patients (n = 42). The study group received ONPS and the control received routine care, without ONPS [6].
Method
After birth, all the newborns were placed under an infant warmer. Pulse oximetry and HR were recorded continuously during the first 10 minutes and at 15, 30 and 60 minutes after birth. The elapsed time was timed with a chronometer that started immediately after the umbilical cord clamping. Oxygen saturation was measured with a Nellcor® N-395 pulse oximeter (Mallinckrodt, MO, USA) with the sensor placed in one of the two lower extremities (postductal saturometry). The pulse oximeter was turned on after the sensor placement in order to increase the accuracy and speed of the pulse signal pickup [10]. The reading of SpO2 and HR values was assessed through visual observation of the plethysmographic curve and the numerical signal of the device [11–14].
In the ONPS group newborns, the procedure was performed immediately after birth; starting with the mouth, then the retro-pharynx and finally both nostrils, using a sterile polyethylene tube of 8 French caliber introduced up to 6 cm, with a negative suction pressure of less than 30 mmHg, for no longer than 15 seconds. The No-ONPS group newborns received only routine care, consisting of cleaning, drying and stimulation [6]. The Apgar score was assigned by the pediatrician or midwife in charge of the care of the newborn during the postpartum evaluation. Subsequently, all the newborns remained in an infant warmer with servo control, maintaining an axillary body temperature between 36.5–37.5°C until completing the study time. No newborns required oxygen or resuscitation maneuvers during the evaluation period or during the 48 hours after birth.
Statistical analysis
Univariate analysis was performed where the mean and standard deviation, minimum and maximum were calculated for the quantitative variables. Bivariate analysis was done to compare the mean arterial oxygen saturation and heart rate according to the groups with and without ONPS. The Shapiro Wilk normality test was performed first. When variables had normal distribution, the homogeneity of variance test was carried out. If this was fulfilled, the t-test was used; otherwise the Welch test was applied. Non-parametric Mann Whitney test was used if the normality test was not met.
The data recording was done in Microsoft® Excel 2010 software. Data was analyzed using the statistical program SPSS for Windows V.11.5 and Stata V.14. The differences were considered statistically significant with p < 0.05.
Results
A total of 84 healthy term infants were enrolled. All the newborns were vigorous and with clear amniotic fluid. The demographic characteristics of both groups were similar (Table 1). The average birth weight of the newborns with ONPS was 3533±403 g, and 3575±568 g in the No-ONPS group. The mean SaO2±SD at the first minute after birth in the newborns with ONPS was 52.6±7.6% and 56.1±10.8% in the No-ONPS group; (p = 0.28). During the second and third minute, a greater saturation was observed in newborns in the N-ONPS group, but also without statistical significance (Table 2). After the sixth minute and until one hour postpartum, saturations were similar between groups. Regarding the HR, the only significant difference was found at the first minute after birth, with the mean value±SD of 137±25 bpm in the No-ONPS group versus 148±13 bpm in the group in which ONPS was performed (p = 0.02). This difference disappeared in the following minutes (Table 3). In both groups oxygen saturation was higher than 95% at 15 minutes, reaching a value higher than 98% at 60 minutes after birth (Fig. 1). No adverse effects were recorded in any of the enrolled infants.
Demographic characteristics of 84 newborns
Demographic characteristics of 84 newborns
NS = Not significant.
SpO2 in healthy newborns by caesarean section with and without oronasopharyngeal suction in the first 60 minutes after birth
NS = Not significant.
HR in healthy newborns by caesarean section with and without oronasopharyngeal suction in the first 60 minutes after birth
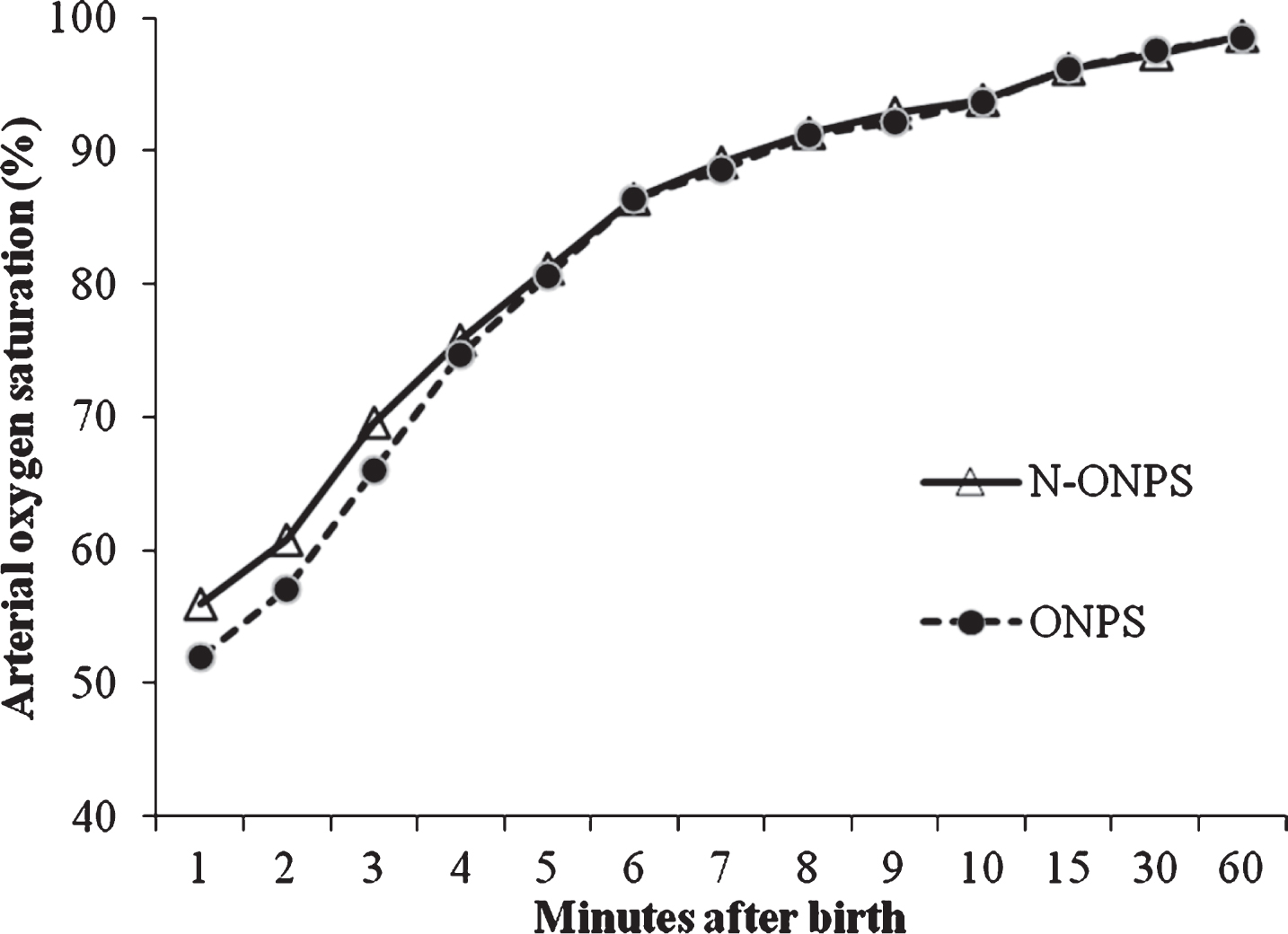
Arterial oxygen saturation in infants born by elective cesarean section with ONPS. versus No-ONPS in the first 60 minutes after birth.
Although ONPS is no longer recommended in vigorous neonates [5, 6], regardless of the route of delivery, this procedure is still routinely performed in many institutions, especially in those infants whose delivery is via cesarean section. In infants born by elective cesarean section, there is frequently an absence of labor, so the series of hormonal changes that occur in normal labor that facilitate the absorption of the pulmonary fluid do not occur [15, 16]. This is compounded by the absence of the compression of the thorax that normally occurs during the passage of the fetus through the birth canal [16]. Therefore, in these cases, ONPS may be helpful for the elimination of pulmonary fluid from the upper airway allowing adequate gas entry into the lungs, favoring oxygenation and ventilation [17]. Several studies have reported deleterious effects during and after ONPS such as vagal stimulation with consequent bradycardia or apnea, irritation of the airway mucosa and increased risk of infection, concluding that it is not a risk free procedure [1, 9].
In the present study, no statistically significant difference was found in the SpO2 of infants born via elective cesarean section undergoing ONPS in comparison to those who did not undergo this procedure. It should be noted that in the No-ONPS group, no infant required any type of oral, nasal or pharyngeal aspiration during the first 48 hours of birth.
Most studies published so far, regarding the usefulness of the ONPS aspiration have been carried out in term pregnancies delivered vaginally [1, 18–20]. Carrasco et al. [18] concluded that ONPS was not beneficial, demonstrating lower SpO2 levels in the first 6 minutes of birth in the group of newborns with ONPS and a longer time in achieving a normal range of saturation (>92%) compared to newborns who did not receive ONPS. It should be noted that the neonates evaluated in this study were all born by vaginal delivery, different from the present study in which all neonates were born by cesarean delivery. In another study published by Estol et al. [1] with 40 healthy term infants delivered vaginally with or without ONPS, respiratory mechanics was analyzed by a computerized pneumotachograph and no significant differences in pulmonary dynamic compliance and total lung resistance at 10, 30 and 120 minutes after birth were observed. They concluded that ONPS in healthy newborns is not necessary, because the amount of fluid extracted by the ONPS is small in comparison to the total pulmonary fluid present at birth, which is mostly eliminated by normal physiological mechanisms. The mechanisms that allow the clearence of lung fluid during labor are diminished in newborns delivered via cesarean section, but the data available has not shown clear evidence to support the benefits of ONPS in these neonates [7].
In the latest international consensus of neonatal resuscitation published in 2015 [5, 6], airway suction maneuvers are not recommended. However, in these recommendations there is no mention about the way of delivery, in circumstances that in the majority of published data, the population studied are children born via vaginal delivery [1, 19]. is the guidelines only emphasize that repeated and/or prolonged suction maneuvers can delay the initiation of necessary and beneficial resuscitation measures in a compromised child at the moment of birth [5, 20].
So far, the only work published regarding the effect of postpartum ONFS in children born by elective cesarean section is the one by Gungor et al. [7], which showed that newborns without ONPS present a SpO2 significantly greater between the 2nd and 6th minute postpartum in relation to neonates with ONPS. This was consistent with the results obtained from pH and PO2 measurements in umbilical cord samples. This result differs from our study, in which we found no significant difference in SpO2 between both groups, evaluated up to 60 minutes after birth. In relation to HR, it was significantly lower in the No-ONPS group, a difference similar to that found in the first minute of our cohort. This result can be explained by the tactile stimulus produced at the moment of the maneuver on the first minutes after birth. It should be noted that all caesarean section cases enrolled in the study by Gungor et al. [7] were performed on pregnant women who received general anesthesia, which could influence the results.
In conclusion, no statistically significant differences were found in SpO2 during the first postnatal hour in newborns delivered by cesarean section who received ONPS in comparison to those in whom ONPS was not performed. A lower HR was observed in infants without aspiration only at the first minute after birth.
The results of this study do not support the routine use of ONF aspiration in healthy term newborns delivered via elective cesarean section.