
Abstract
OBJECTIVE:
To ascertain the rate of in-hospital supplementation as it relates to early breastfeeding (BF) and early formula feeding (FF) and its effects on BF (exclusive and partial) at the time of discharge for infants born to women with pregestational diabetes mellitus (PGDM).
METHODS:
Retrospective cohort investigation of 282 women with PGDM who intended to BF and their asymptomatic infants admitted to the newborn nursery for blood glucose monitoring and routine care. Early feeding was defined by the initial feeding if given within four hours of birth.
RESULTS:
Of the 282 mother-infant dyads, for 134 (48%) early feeding was BF and for 148 (52%) early feeding was FF. Times from birth to BF and FF (median 1 hr, 0.3–6) were similar, while the time to first BF for those who FF and supplemented was longer (median 6 hr., 1–24). Ninety-seven infants (72%) who first BF also supplemented. Of these, 22 (23%) BF exclusively, 67 (69%) BF partially and 8 (8%) FF at discharge. One hundred seventeen (79%) who first FF also supplemented. Of these, 21 (18%) BF exclusively, 76 (65%) BF partially and 20 (17%) FF at discharge.
CONCLUSION:
Regardless of the type of first feeding, the majority of infants born to women with PGDM require supplementation. Even when medically indicated, in-hospital supplementation is an obstacle, albeit not absolute, to exclusive BF at discharge. Parents should be reminded that occasional supplementation should not deter resumption and continuation of BF.
Keywords
Background
Infants born to women with pregestational diabetes mellitus (PGDM) are at risk for neonatal morbidities including hypoglycemia [1–5] and BF initiation failure [6–8]. Early breastfeeding (BF) or early formula feeding (FF) may facilitate glycemic stability in infants born to women with PGDM and may prevent or correct neonatal hypoglycemia [2–5, 9].
While BF is preferable, maternal complications and/or neonatal morbidities often delays or precludes early BF [9–11] and may lead to early FF and formula supplementation [9, 11–13]. Early BF is predictive of BF at discharge and BF duration afterward [14–17]. Conversely, FF shortly after birth or during the hospitalization is a strong predictor of BF initiation failure and of shorter BF duration postpartum [9, 18–20].
The American Academy of Pediatrics [5] and the Academy of Breastfeeding Medicine [10, 21] strongly recommend exclusive BF for all healthy infants during birth hospitalization and beyond. However, these organizations acknowledge that other nutritional options may be needed to temporarily replace or supplement BF for infants at risk of other morbidities, especially neonatal hypoglycemia [10, 21].
The negative effects of in-hospital formula supplementation among healthy infants have been extensively addressed: some causative factors have been identified, and some remedies proposed [16, 22–24]. Although limited information on in-hospital formula supplementation for women with gestational diabetes (GDM) is available [18, 26], information on women with PGDM remains scarce [7, 27].
Objective
To ascertain the rate of in-hospital supplementation as it relates to early BF and early FF and the effects of supplementation on BF (exclusive and partial) at the time of discharge for infants born to women with PGDM who intended to BF.
Subject and methods
This retrospective cohort investigation was approved by the Institutional Review Board of Wexner Medical Center at The Ohio State University. Hard copy (2008–11) and electronic maternal and neonatal records (2013–16) were reviewed. The transition from hard copy to electronic medical records occurred in 2012; thus, data from 2012 were not collected. Women were diagnosed with PGDM (Classes B-C-D-R-F-H) according to clinical and laboratory criteria using the modified White’s classification [28]. Obese was defined by a body mass index (BMI) of 29–34 kg/m2, and very obese by a BMI ≥35 kg/m2. The study population consisted of women with PGDM who intended to BF and their infants if delivered at ≥34 weeks, a point in gestation at which many infants can feed orally. Pregnancies affected by major or fatal malformations were excluded. Upon arrival to labor and delivery, each woman declared her infant feeding preference (i.e., BF, FF or a combination).
Depending on the condition of mother and infant following delivery, interactions (holding, skin-to-skin contact, BF) were encouraged. Delivery room and postpartum interactions were observed and recorded by the nursing staff. Our institutional guidelines recommend that any symptomatic infant, regardless of the mothers’ class of diabetes, be directly transferred from the delivery room to the NICU. Indications for NICU admission included respiratory distress (respiratory distress syndrome and transient tachypnea of the newborn), prematurity (apnea, severe hypotonia and poor sucking behavior), perinatal depression, birth trauma and neonatal hypoglycemia. Admission for prevention of hypoglycemia was an option for infants whose mothers had poorly controlled diabetes and/or severe illness (i.e., classes D-R-F-H). Asymptomatic infants able to feed were transferred to the newborn nursery for routine care and glucose monitoring. Our family-centered care system has full-time lactation consultants and rooming-in available.
Screening for neonatal hypoglycemia (blood glucose <40 mg/dl) was done via serial point of care testing (Accu-Chek®) or by plasma glucose measurement in the laboratory (Beckman Coulter AU5800, Beckman Coulter Inc., Brea, CA, USA) starting within the first hour of life after the first feeding and every 2–4 hours as needed [5, 13]. The first feeding (BF or FF) was considered early if given within 4 hours of birth. Infants who developed hypoglycemia were promptly BF or FF and those with recurrent hypoglycemia were transferred to the NICU for intravenous (IV) dextrose (4–6 mg/kg/min) treatment [5, 13].
In the context of this study, breastfeeding includes direct breastfeeding or feeding by hand or pump expressed breastmilk. There were no instances of the use of human donor breast milk. BF was defined as initiated if, at the time of hospital discharge, the infant was exclusively BF (all feedings during the 24 preceding hours were BF) or partially BF (BF and FF in combination). Exclusive BF combined with partial BF was considered any BF. In-hospital supplementation was defined by the provision of standard infant formula as a supplement to breastfeeding [21]. Due to the study design, no follow-up information was available on infant feeding practices beyond hospital discharge.
Statistical analysis
Comparisons among patients according to the type of first feeding were made with two-sample t-tests for continuous variables and Chi square tests for categorical variables. Non-normally distributed continuous variables were compared using the Wilcoxon rank sum test. Significance was established at a p value <0.05. Univariate and multivariate logistic regression were used to ascertain the strength of association of early BF or early FF with formula supplementation and BF status at discharge, controlling for maternal variables (age, diabetes class, parity, BMI, race, smoking, mode of delivery, length of stay in the hospital, and infant feeding preference) and neonatal variables (late prematurity, birth weight, fetal growth, macrosomia, gender, place of admission, hypoglycemia, whether infant was discharged with mother, and length of stay in the hospital).
Results
The study population was composed of 282 women with PGDM who intended to BF and whose asymptomatic infants at birth were admitted to the newborn nursery. Gestational age comprised 175 full-term infants, 78 early term infants and 29 late preterm infants. Thirty-seven of 282 women (13%) exclusively BF and 31 (11%) exclusively FF from birth through discharge, while the remaining 214 (76%) supplemented BF with standard infant formula during their hospital stay. Comparison of the demographic and clinical characteristics of women who BF and supplemented with those who did not (data not shown) showed similarities for mother and infant except for a higher rate of cesarean deliveries (63% vs 37%, p < 0.001) and a lower rate of exclusive BF at discharge (20% vs 54%, p < 0.001) among those who supplemented.
Clinical and demographic data related to the initial feeding
The study population categorized by the type of initial feeding (BF or FF) is presented in (Fig. 1). For 134 (48%) of the 282 infants, the first feeding was BF, and for the remaining 148 (52%), it was FF. Women who initially BF their infants were more likely to have delivered vaginally and had a shorter hospital stay than women whose children initially FF (Table 1). Also, infants in the initial FF group were more likely to be preterm or large for gestational age and to have experienced hypoglycemia before any feeding. The time from birth to the first oral feeding showed that 75% of early BF and 71% of early FF infants were fed within 1 hour of birth, 14% of BF and 18% of FF between 1 and 2 hours, and 11% of BF and 11% of FF between 3 and 4 hours. Formula supplementation was given to 97 (72%) of those in the early BF group while BF was initiated for 117 (79%) of those infants in the early FF group.
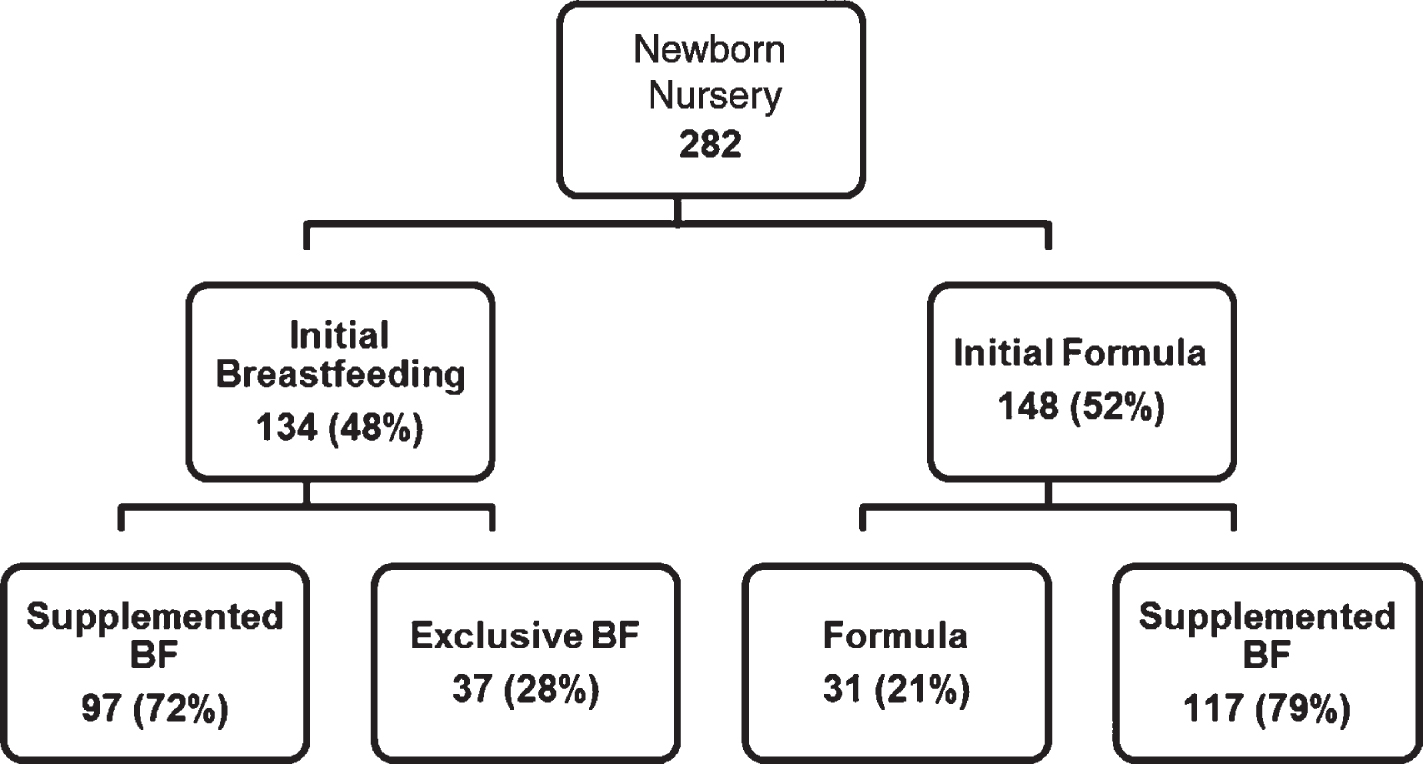
Study population categorized by type of initial feeding.
282 PGDM dyads according to type of initial feeding
p-values are from chi-square test except where noted: *two-sample t-test; **Wilcoxon rank sum test.
The adjusted odds for initially BF (vs. initially FF) were 2.3 times higher for babies born vaginally as compared with infants born via cesarean (aOR2.3; CI95% 1.4–3.8, p = 0.0009). Infants who initiated FF were 3.5 times more likely to have had hypoglycemia before their first feeding (aOR3.5; CI95% 1.8–6.8, p = 0.0001). Exclusive BF at discharge was more common among infants who initially breastfed than among those who initially received formula (44% vs. 14%, p < 0.0001).
The rate of in-hospital formula supplementation was similar among hypoglycemic infants and euglycemic infants [79 of 99 (80%) and 135 of 183 (74%), respectively]. At the time of discharge, infant feeding outcomes of hypoglycemic and euglycemic infants who supplemented were similar (exclusive BF 16% and 22%, partial BF 71% and 65% and FF 13% and 13%, respectively).
Seventy-three of 99 (74%) hypoglycemic infants were treated successfully with repeated oral feeding alone, 8 infants with BF and 65 with formula. Infant feeding outcomes of these 73 infants, and those of 183 euglycemic infants were similar (exclusive BF 23% vs 34%, partial BF 55% vs 48% and FF 22% vs 18%, respectively). Twenty-six of the 99 (26%) hypoglycemic infants who required oral feedings and IV dextrose for correction were transferred temporarily to the NICU. Five infants stayed for less than 12 hours, 1 for one day, 6 for 2 days and 14 for 3 days or longer. At discharge, of these 26 infants one (4%) BF exclusively, 16 (61%) BF partially and 9 (35%) received formula. BF outcomes were similar for the 12 infants who stayed ≤2 days and for the 14 who stayed longer.
Time to first breastfeed and infant feeding at discharge
Of all 214 infants who supplemented, 34% BF within the first hour of life, 34% between 2 and 6 hours and 32% BF later than six hours (Table 2). At discharge, of the 73 infants who BF within the first hour of life, 24% BF exclusively, 66% BF partially and 10% received formula. There were no significant differences in feeding outcomes for infants who first BF within 1 hour of birth, 1–2 hours, 3–4 hours, or 5–6 hours after birth (Fisher’s p 0.99). Women who BF their infants within the first six hours after birth were more likely to BF (either exclusively or partially) at hospital discharge as compared with women who first BF their infants ≥6 hours after birth (OR2.4; 95% CI 1.1–5.5, p = 0.03).
Time to first breastfeed for 214 women who supplemented and infant feeding at discharge
Time to first breastfeed for 214 women who supplemented and infant feeding at discharge
The cesarean rate for the 89 infants whose first feeding was within 2 hours of birth was 53%, and for the 125 who BF from 3 hours on, it was 70% (p = 0.01). Conversely, the vaginal delivery rate declined significantly from 47% to 30% for the two time periods.
Formula supplementation started in 181 of 214 dyads (85%) during the first day, 21 dyads (10%) during the second and 12 dyads (5%) later. Since the median number of formula supplements during the first 24 hours following birth was 4, with a range of 0–10, a comparison was made of 113 IDMs who received ≤4 supplements with 101 who received ≥5 supplements (Table 3). Women-infant dyads who supplemented with formula five or more times in the first 24 hours had longer average hospitalizations, lower gestational age, higher rate of late preterm birth and a higher incidence of hypoglycemia before feedings. Infants given four or fewer formula supplements in their first day were significantly more likely to have early BF, more BF during their first day, and BF exclusively at discharge (aOR 8.4; 95% CI 2.2–31.2, p = 0.002).
Formula supplements during the first 24 hours of life and infant feeding at discharge
Formula supplements during the first 24 hours of life and infant feeding at discharge
p-values are from chi-square test except where noted: *two-sample t-test; **Wilcoxon rank sum test; ***Fisher’s exact test.
All infants in the exclusive BF and exclusive FF groups, as well as 90% of those in the partially BF group, were discharged home by the fourth day of life (Table 4). For infants in the exclusive BF group, the median number of BF increased while the number of supplements decreased from day 1 through day 4. All infants in the exclusive FF group breastfed at least once during the first or second day, and from then on, the frequency of BF declined while the number of supplements increased rapidly. Among infants who partially BF at discharge, the median number of BF and supplements after the second day remained stable.
Breastfeeds and supplements (median, range) during hospital stay and infant feeding at discharge
Breastfeeds and supplements (median, range) during hospital stay and infant feeding at discharge
BFs: Breastfeeds, SUPLs: Supplements, *Kruskal-Wallis p < 0.0001.
The volume (mean and SD) of supplements for the exclusive BF at discharge group was 26±21 ml/kg/day during the first and second day and declined thereafter. For infants in the partial BF group, the volume for the first day was 32±20 ml/kg/day, 41±20 ml/kg/day for the second, 53±25 ml/kg/day for the third and 62±32 ml/kg/day for the fourth day. For infants in the FF at discharge group, volumes for the first day were 57±26 ml/kg/day, for the second 72±25 ml/kg/day, for the third 97±29 ml/kg/day and for the fourth day 101±48 ml/kg/day.
The incidence of pregnancies complicated by diabetes continues to rise across the world [29].Thus, it may be anticipated that maternal and neonatal morbidities and poor BF outcomes among women with PGDM will remain a challenge [3, 7–9]. Low rates of exclusive BF and high rates of partial BF during hospital stay and at discharge for women with PGDM have long been recognized [2, 30]. Among healthy women and those affected by complex pregnancies, the recognition that early FF and in-hospital formula supplementation were strongly associated with low exclusive BF at the time of discharge and with shorter BF duration post-partum renewed the interest of clinicians and investigators in this subject [12, 32].
The benefits of early BF over early FF on BF initiation rates among infants born to women with PGDM who intended to BF demonstrated here are in line with previous reports [9]. By common sense definition, in-hospital formula supplementation must follow initial BF or later BF occurrences. Thus, it is valid to categorize as supplemented, infants whose initial feeding was formula followed by any number of BF before receiving FF again. The beneficial effects of initial BF on BF initiation at discharge, albeit not as dramatic, are still recognizable among infants who supplemented formula. Smoking during pregnancy, primary cesarean section, hypoglycemia before feedings, large for gestational age infants and admissions to NICU were identified as stronger predictors of FF as a first feeding among infants born to women with PGDM [9].
Current AAP guidelines for healthy infants recommend exclusive BF during hospitalization and continued BF for at least one year following hospital discharge [5]. Information about early BF, BF initiation and BF duration for healthy populations is abundant [12, 32]; however, similar data regarding women with PGDM remain scarce [15, 33]. The ABM strongly endorses exclusive BF and discourages unnecessary formula supplementation among healthy term and late preterm infants, but provides specific examples of mother-infant dyads who, due to illness, would benefit from supplementation [10, 21]. The rate of in-hospital formula supplementation in healthy mother-infant dyads [12, 34–38] range from 16 to 65%. Among women with GDM, formula supplementation ranged from 61–79% [25, 40], and among those with PGDM, it ranged from 50–72% [6, 27]. The high rate of supplementation among women with PGDM is likely a result of maternal morbidities (i.e., obesity, cesarean deliveries, delayed lactogenesis, complications of labor and delivery, difficulties with lactation) and neonatal morbidities (i.e., preterm, early term, macrosomia, hypoglycemia, hyperbilirubinemia) [41]. Considering the incidence and severity of maternal and neonatal morbidities affecting women with PGDM, the high supplementation rates reported here were not unexpected.
Time of first feeding (BF or FF) is important because many critical maternal and neonatal physiological interactions occur during the first hours after birth (i.e., skin-to-skin contact, early BF) [33, 43]. In normal as well as in complex pregnancies, certain hospital practices may delay infant feeding (i.e., cesarean section, eye prophylaxis, vitamin K administration and, relevant to this study, blood glucose monitoring). While some of these practices may be postponed, others may be unavoidable in women with PGDM whose infants are at risk of hypoglycemia [1–3, 44].
BF during the first hour of life among healthy populations has been considered a strong predictor of BF initiation and BF continuation after discharge from the hospital [22]. However, recent data showed that in the US, BF within an hour of birth was accomplished by 64% of healthy term infants [41], whereas worldwide, it was accomplished by only half of healthy term infants [45]. Thus, it is not surprising that women with GDM were less likely than women without diabetes to BF during the first hour [40]. In 2011, Sparud et al. [15] reported that 55% of 109 type 1 diabetic mothers breastfed within two hours after birth as compared to 87% of healthy controls. Our data showed that 89 of 214 women with PGDM (41%) who later supplemented, breastfed during the first two hours. Interestingly, rates of exclusive BF and any BF at discharge were similar for infants who breastfed any time during the first six hours, while those who BF after six hours had lower rates of exclusive BF and higher rates of exclusive FF. The association of cesarean delivery with delays in mother-infant contact (namely BF) among women with PGDM and other high-risk obstetrical conditions has been previously reported [8, 46].
Neonatal hypoglycemia and in-hospital formula supplementation
Another important benefit of BF during the first hours is the prevention and/or treatment of hypoglycemia in infants at risk [1–5, 13]. While the preventive value of either type of early feeding is still debatable, several publications from our institution established that about two-thirds of cases of neonatal hypoglycemia among infants of diabetic mothers may be corrected with oral feedings alone [2, 13]. The therapeutic effect of repeated feedings, whether BF or FF, is rewarding because it prevents the unavoidable mother-infant separation that occurs during IV dextrose treatments. We hypothesize that hypoglycemia documented before the first feeding may prompt healthcare providers to start formula supplementation in circumstances when the mother is not available, able or ready to BF. Unfortunately, maternal inability to BF and the subsequent initiation of formula supplementation may undermine the mother’s sense of self-efficacy so critical for BF initiation and BF continuation [26, 47].
Bentley et al., in 2017 [24] reported that neonatal hypoglycemia increased the risk of formula supplementation in women with diabetes. Our data show that formula supplementation was similar among hypoglycemic and euglycemic infants. In an early study of 108 women with type 1 diabetes, Sparud et al. [15] reported that neonatal hypoglycemia was not a predictor of BF at two or six months. More recently, we observed that exclusive and any BF at the time of discharge was similar among hypoglycemic and non-hypoglycemic infants. The observation that BF at discharge was different among infants whose hypoglycemia was corrected orally versus those who received IV dextrose, highlights the negative effects of maternal-infant separation [44, 49]. Until glucose gel becomes widely used and proven to be beneficial, early feedings remain the first line for prevention or treatment of hypoglycemia [2–4, 9].
Rate of supplements (frequency)
The number of formula supplements given to healthy infants during their hospital stay seems to be an independent predictor of BF initiation and duration. In 2010 Bunik et al. [34] reported that infants of healthy women given less than 3 supplements on the fourth postpartum day were more likely to BF at 1 month (OR 7.7; CI 95% 2.4–24.3), at 3 months (OR 3.1; CI 95% 1–9.8) and at 6 months (OR 8.1; CI 95% 1–1.65). A few years later, in a landmark study, Chantry et al. [12] noted that the number of in-hospital formula supplements given to healthy infants remained a significant predictor of BF cessation by day 60 (OR 9.8; CI 95% 5.0–19). In the present study, we noted that women who BF within the first 6 hours and who supplemented less than 5 times during the first 24 hours were more likely to exclusively BF and less likely to FF at discharge. The pattern of in-hospital formula supplementation during the first few days of life and infant feeding at discharge have relevance because identifying women with PGDM who are less likely to exclusively BF is paramount for appropriate and targeted BF support [24].
Although we do not have data on feeding outcomes after discharge, we share the optimistic view that partial BF at the time of discharge may indicate a continued effort to re-establish exclusive BF post-partum [24]. After all, BF at discharge was found years ago to be an independent factor associated with BF at discharge [15].
We, like others, found no predictive value in the volume of supplements during the first two days following birth and BF outcomes [12]. Recommendations to limit the volume of supplements while attempting to BF seems reasonable because emptying the breast as much as possible has well-known physiologic implications [10, 40].
Limitations of this investigation are those inherent in all retrospective designs and the lack of follow-up information regarding infant feeding after discharge. Also, the definition of BF initiation at discharge may be applicable only to women with complex pregnancies for whom early mother-infant contact may be delayed. The strength of this investigation rests in the size of the high-risk obstetrical and neonatal population and the fact that the data were obtained directly from hospital records, not via post-delivery maternal questionnaires. Identifying women and their infants who are less likely to exclusively BF at discharge following formula supplementation is important for targeted BF support [24].
Conclusion
The majority of infants born to women with PGDM who intended to BF are at risk for neonatal hypoglycemia, early FF, in-hospital formula supplementation and exclusive BF failure. Even when medically indicated, in-hospital formula supplementation is an obstacle to exclusive BF at discharge. Parents and healthcare providers should be reminded that temporary formula supplementation need not deter resumption and continuation of BF. Additionally, the high rate of partial BF during the hospital stay may identify women who are still striving toward exclusive BF after discharge and who, with specific support and encouragement, could achieve their original goal.