
Abstract
BACKGROUND:
Every year, about 50 babies in New York City die from a sleep-related injury. The Bronx County ranked second highest rate of sleep-related infant deaths (SRID) at 0.5 per 1000 among the other boroughs. The highest rate was among blacks and the rate of SRID cases were highest in our population at 0.97 (zip code 10466) among all other Bronx neighborhoods which comprises 77% of non-Hispanic black population. Further, Bronx has the highest preterm birth rate at 9.5%. This quality improvement (QI) project aimed to develop and implement an educational initiative on infant safe sleep (SS) to improve “Safe Sleep Practices (SSP) in a level III neonatal intensive care unit (NICU) for one of the highest risk populations in the country.
METHODS:
Baseline data was collected prior to initiating the QI project. Multiple plan-do-study-act (PDSA) cycles were completed over a 12 month period. Run charts were utilized to identify improvement and guide interventions. These interventions included education for nurses, crib cards, posters, feedback forms, grand rounds and small group discussions.
RESULTS:
Approximately 600 crib checks (CC) were performed over the duration of this project. At baseline, 7% of infants were placed in a SS position in the NICU. Following the QI project, SS position increased to 96% of infants.
CONCLUSION:
Multifactorial interventions significantly improved SS compliance among NICU nurses. Cultivating personal motivation among nurses, consistent empowerment and dedication to culture change by the entire team was crucial for the sustainability of the project.
Abbreviations
Accidental suffocation and strangulation in bed American Academy of Pediatrics Neonatal Intensive Care Unit Crib Checks New York City New York State Perinatal Quality Collaborative Plan-Do-Study-Act Quality Improvement Safe Sleep SS Education Safe Sleep Practices Sleep-Related Infant Deaths Sudden Infant Death Syndrome Sudden Unexplained Infant Deaths
Introduction
Each year in the United States, there are about 3,500 sudden unexplained infant deaths (SUID). These are defined as deaths among infants less than one year old and have no immediate obvious cause. The commonly reported types of SUID are sudden infant death syndrome (SIDS), unknown causes, and accidental suffocation and strangulation in bed (ASSB). Sleep-related infant death (SRID) is another terminology that describes a unique grouping of infant deaths caused by injury or positional asphyxia, ASSB and sudden infant deathsyndrome (SIDS).
Per the 2016 report, the Bronx had the highest infant mortality rate (IMR) of all the New York City (NYC) boroughs at 5.5 per 1000 infants [1] and the highest preterm birth rate at 9.5% [2]. In NYC, SRID accounted for over 80% of infant injury deaths from 2004 to 2011. In a summary report of SRID in NYC, from 2005 to 2012, the Bronx county ranked second highest at 0.5 per 1000 among the other boroughs. The highest rate was among blacks and the rate of SRID cases were highest in our population at 0.97 (zip code 10466) among all other Bronx neighborhoods which consists of 77% non-hispanic blackpopulation [3].
The American Academy of Pediatrics (AAP) defines safe infant sleep practices as supine positioning in a safety-approved crib without positioning devices and free of quilts, comforters and other soft surfaces [4]. In addition, the AAP specifies staff in the NICUs should model and implement all SIDS risk-reduction recommendations as soon as the infant is clinically stable and significantly, before anticipated discharge [5].
In a study designed to explore and describe NICU nurses’ knowledge and practice in the NICU, [6] nearly 95% of respondents identified a non-supine sleep position as optimal for hospitalized preterm infants. Further, only 52% of neonatal nurses routinely provide discharge instructions that promote supine sleep positions at home. Another survey done by Bullock et al. [7] concluded that although nurses no longer place infants in the prone position for sleep, 75% used either the side-lying position or a mixture of side and back positioning. This occurred despite being aware (96%) of the AAP Guidelines and recommendations. Recent studies conducted, [8, 9] concluded that despite the marked drop in the overall incidence of SIDS since 1987, the risk for SIDS among preterm infants remains elevated.
This project was reviewed and approved as QI by the Institutional Review Board of the Children’s Hospital of Montefiore. The project was carried out over a 12 month period from January 1st 2017 to December 31st 2017.
Methods
Setting
Wakefield is a division of the Montefiore Medical Center. It’s a community hospital that has a 15 bed level III B NICU, catering to the local population with an annual admission rate of 440 neonates.
In September 2015, the Wakefield neonatal service joined the New York State Perinatal Quality Collaborative (NYSPQC) SS improvement project. Through this project, the New York State Department of Health worked with 82 birthing hospitals across the state to improve SSP. Random crib checks (CC) performed over a 4 week period in October 2016 through November 2016 showed 7% of the CC had correct infant positioning per the SS policy. Given that preterm infants [8] and our patient population in general are at greater risk of SIDS, there was an acute need to re-introduce the QI project to educate patient care teams to promote SS in this vulnerable patient population. To improve outcomes and compliance, the QI project was amended to include a new project leader, new interventions and innovations.
A QI model was developed to introduce the AAP guidelines [10] on SSP into the NICU nursing practice in a consistent and sustainable method. The project team included the NICU hospitalist, a neonatologist, the Director of Newborn Services at the Wakefield Division, the Nurse Manager, two nurses and a Nurse Practitioner. The team members met at monthly QI meetings to discuss progress for the duration of the project.
Aims
In January 2017, the primary aim was a 20% improvement in the SS compliance rates (from 7% to 27%) by December, 2017. The second aim was to improve documentation of SS from 50% to 60% by December, 2017. The team was responsible for extracting baseline data, developing initial presentations and education material for the nurses, visual cues for staff as well as conducting question and answer sessions to address barriers for compliance, auditing on a regular basis with the CC tool, chart reviews and distributing crib cards and SS book “Sleep baby, Safe and snug”.
Interventions and implementation
The team initiated the project by identifying key drivers and brain storming possible interventions for each key driver (Fig. 1).

Key Driver diagram.
The key drivers identified were the NICU staff, which included every health care provider that has close contact with the babies, the environment, identification of eligible babies per institution’s SS policy (Appendix 1) and family buy in.
One of the main concerns during these initial deliberation sessions were the suboptimal temperature control in the NICU. The first PDSA cycle consisted of setting up a meeting with the engineering team to discuss how the temperature is regulated in the NICU. Identifying the need for better temperature regulation resulted in more sensors being placed in the NICU to eliminate the wide variations of temperatures throughout the day. This reduced the “over bundling” of the babies which was due to the perceived risk of hypothermia. By eliminating this barrier and providing the nurses with the optimal environment for the neonates, they were able to practice SS per policy.
All nurses in the NICU are required to complete a module on SS and be knowledgeable about the SS policy at Montefiore Medical Center. The module contains information on understanding and reducing the risk of SIDS and other sleep-related causes of infant death. It also teaches how to communicate with parents and caregivers about SIDS, the importance of nurses as role models, challenges of SIDS reduction and other sleep-related causes of infant death. During the initiation of the education phase this knowledge was revisited through a PowerPoint® presentation followed by a question and answer session to refresh knowledge on SS and to identify and solve barriers for noncompliance. We further shared baseline data and photographic proof of recent unsafe sleep environments noted in the NICU as well as population specific data. It was intended to highlight the requirement to make improvements in SSP in the NICU setting and motivate nurses to adhere tothe SS policy.
During the 2nd PDSA cycle, one nurse was given education on SS, adhering to the 1:1:1 test where the change was tested on a small scale i.e. one nurse, one shift, one patient and later scaled up when she shared her knowledge with five other nurses, according to the five times rule which is multiplying the number of encounters or events used in the last cycle by five. In this case, one nurse sharing knowledge and skills with five other nurses who then share with five more in subsequent PDSA cycles.
A Safe to Sleep crib card (Appendix 2) based on AAP recommendations was developed as a multi-purpose tool. The clinical staff was responsible for putting the card in all open cribs when an infant met the criteria to be eligible for SSP. This card was to be placed on the crib in a location easily visible to the visiting caregivers, was used to remind medical providers and parents that the infant has started SSP, and as a cue to discuss SSP with parents. The crib card had two sides: one that stated “I am a Safe Sleep Ambassador” which was meant to provide ownership and place personal responsibility onto the nurses taking care of that infant. The reverse was a visual of a baby in correct SSP. At discharge, parents received a handout on SSP and, starting in October 2017, the book “Sleep baby, Safeand Snug”.
A SS poster (Appendix 3) was utilized as a reminder and as guidance to what SS in the NICU should look like. The team identified that there were discrepancies between nurses understanding of what consists of “objects in the crib” and what is considered as acceptable when it comes to napkins under the baby’s head to collect spit up, etc. A poster themed “What safe sleep looks like in the Wakefield NICU” with the picture of an infant in the unit in an acceptable SSP was developed and placed in commonly visible and visited places in the NICU e.g.: above hand washing areas and milkwarming areas.
The team identified discrepancies in the documentation of SS in the electronic medical record (EMR). The key nursing stakeholders provided information to all staff to standardize documentation.
A feedback form (Appendix 4) developed by adapting concepts of the Influencer Behavioral Change Framework [11] was given out to nurses following the first half of the project and at the end of the project.
The team invited national and local leaders in SS promotion and organized grand rounds in the Children’s Hospital which was followed by the speakers conducting small group sessions with the nurses in the NICU. This session emphasized the impact of a sleep related death on a family and was conducted by the Director of Education and training in a prominent foundation that supports parents in managing grief related to SRID. Awareness to local data in SRID, and the value of modeling SSP in the hospital setting was highlighted by a spokesperson from The Citywide Infant SS Initiative.
Measures of improvement are similar to that of the NYSPQC.
Measures of improvement
M1/Crib Check ALL: Percent of infants (%), sleeping or awake and unattended in a crib, in a SS environment.
Only cribs of the SSP-eligible infants were selected for auditing. Multiple audits were conducted by the QI team without a previous warning to the staff nurses.
The following sub measures were obtained to identify specific areas of non-compliance, to identify barriers and solutions: [Ma/Clothes]: %, in a sleep sack or swaddled or in safe clothing; [Mb/Blanket]: %, with blanket over baby tucked in; [Mc/Flat]:%, with the head of crib flat; [Md/Supine]: %, positioned supine; and [Me/No Item]: %, with the crib free of objects.
M2/Education
Percent of medical records with documentation of SS education and SIDS. This data was available in the patients discharge summary in the EMR in the care plan section maintained by the nurses.
An edited version on the NYSPQC crib check tool (Appendix 5) was used for data collection. Medical records of infants discharged from June-November 2016 were analyzed to determine a baseline percentage of medical records, with documentation of SS.
Data collection and statistical analysis
CC were performed six to eight times per month. Data was compiled and calculated on a monthly basis. The denominator was the total crib checks. The numerator was the specific measure, including clothes, blanket, position and loose items.
Run charts were formulated with data from each month and were used to plan and implement further PDSA cycles or continue same.
Results
On average, 50 CC were done each month. The baseline data for M1/Crib check ALL (Fig. 2) measure was 7%. At the end of the project, this number improved to 96%. The most improvement was seen in loose blankets [Mb/Blankets] (Fig. 3) i.e. from a median of 11.5% to 98% and the smallest improvement was seen in objects in the crib [Me/No Item] (Fig. 4), where the noted increase was from 78.5 to 94% by the end of the project. Percentage of cribs with the head of crib flat reached a median of 100% from baseline median of 88.5%. The percentage of babies in a supine position was 41% in January. In February, the numbers increased and remained between 96–100%. The run chart for percent of infants in safe clothing [M1a/Clothes] has been 100% at baseline and during the project. [Mb/Blankets], [Me/No Item] and [M1/Crib Check ALL] run charts show a reduction in compliance in April. They are above 90% from July onwards.
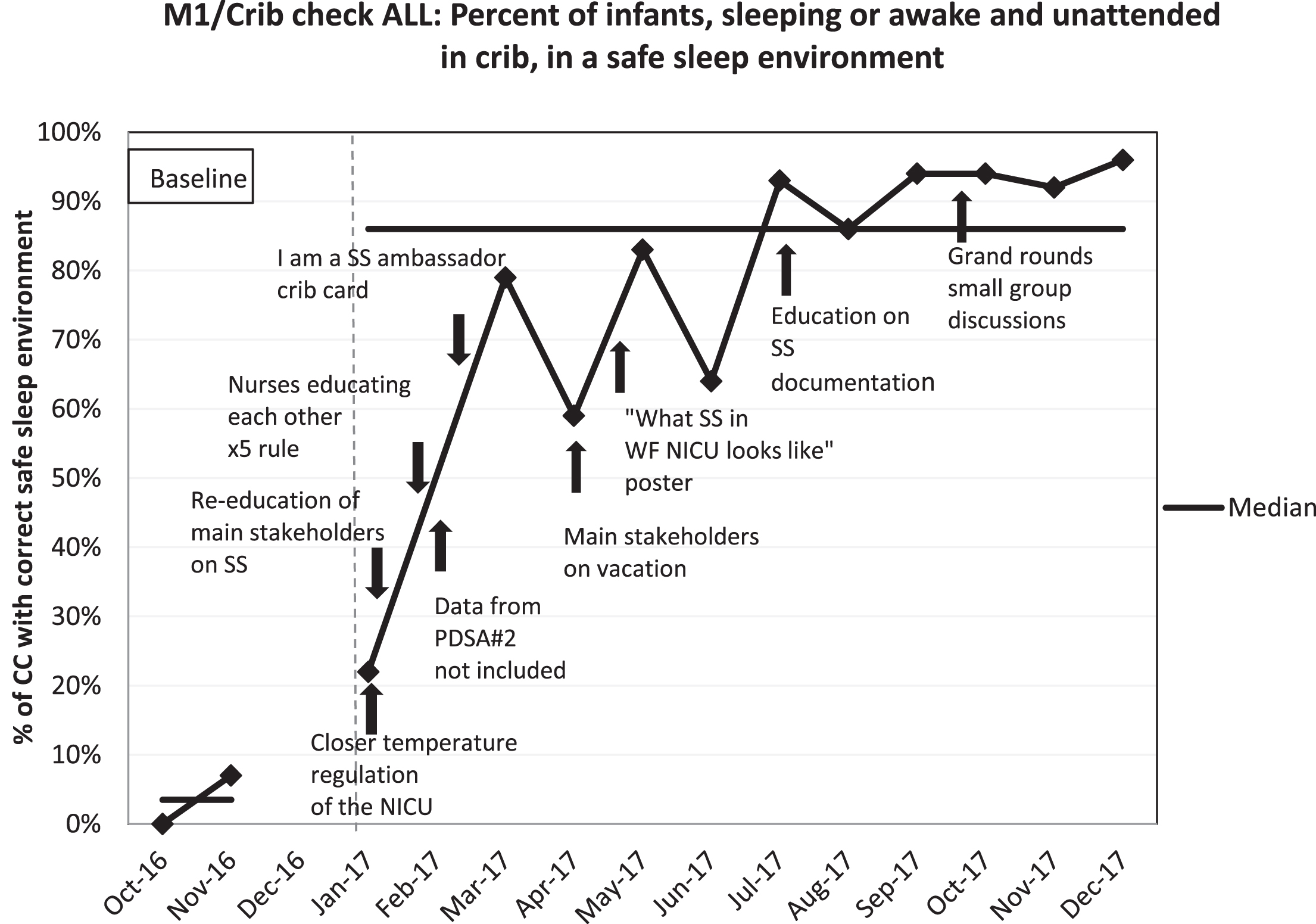
M1/Crib check ALL.
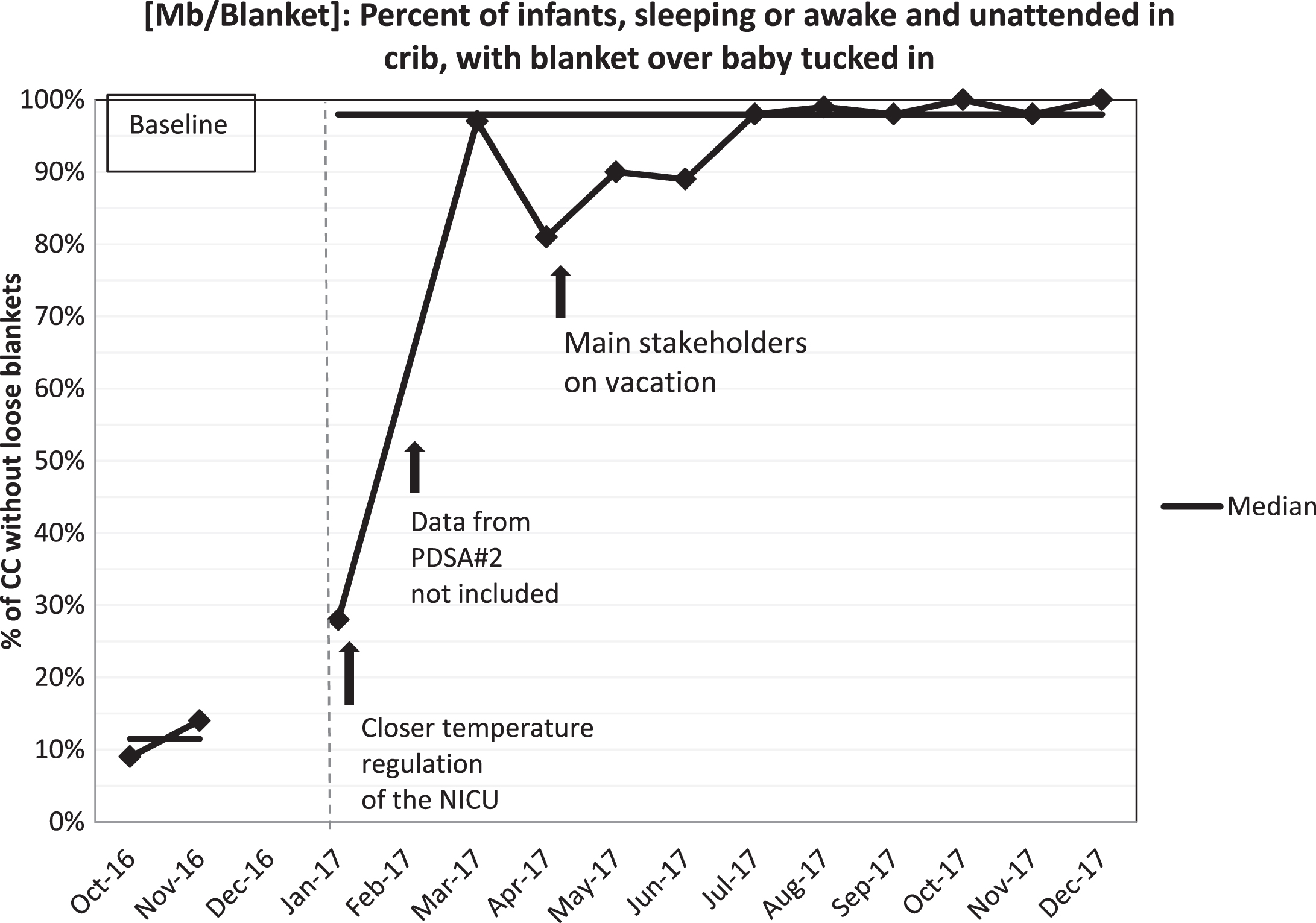
Mb/Blanket.
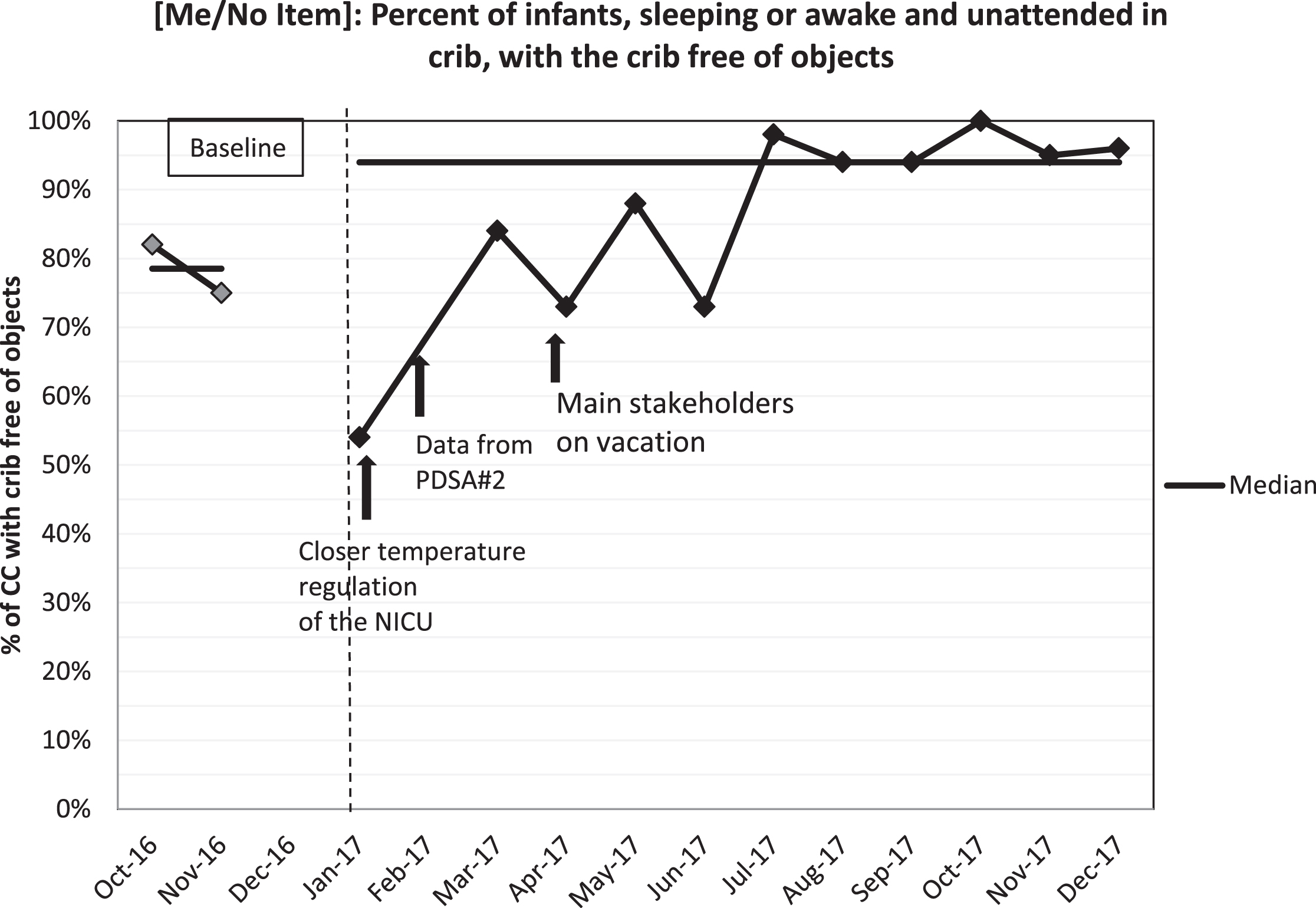
Me/No Item.
During the second PDSA cycle data from only one nurse was collected in error. Hence, data from that cycle was eliminated from the run charts. Documentation of SS education (SSE) to parents is done by nurses in the EMR when a baby becomes eligible for SSP in the NICU. Wakefield transitioned to a new EMR system in June 2016. Baseline data was collected from day one of new EMR to end of October, for approximately 150 newborns admitted to the NICU. The median number of charts with documentation of SSE was 50%. This number increased to 62% at the end of the project. Approximately 400 charts were audited. There was a drop in documentation in April 2017.
The feedback form (Appendix 4) given to the participating nurses in June showed that 77% thought the project to be a success, with 85% agreeing that the tools provided (SS crib card/poster) and reminders were useful. Only 54% indicated that it was meaningful to practice SS in the NICU. In November, when the feedback form was redistributed, 100% of the nurses indicated the project was a success with 95% agreeing the tools provided were useful. At this time, 100% of the nurses found it meaningful to practice SS in the NICU.
The majority of the population at Wakefield is non-hispanic black. In NYC, sleep-related injuries remains one of the leading causes of death among infants, with 40 deaths in 2014 and 48 deaths in 2015 at a combined rate of 36.1 per 100,000 live births for 2014–2015. During this time period, premature infants (less than 32 weeks) compared to other gestational ages and infants residing in the Bronx compared to other boroughs had higher rates of sleep-related injury deaths. When considering infant characteristics for sleep related infant injury deaths (deaths per 100,000), the highest were in the black (non-hispanic) population. According to the circumstances found at death scene investigations, 49% were found on their side or stomach, bed sharing was present in 52% and infants were found in sleep locations other than a crib or other SS surface 72% of the time. The locations included adult beds, couch or sofa, and a stroller or car seat. Excess bedding was seen in 68% of the cases.
A recent study by Mathews et al., [12] concluded that African-American infants were more likely to be placed prone and share the bed with a parent. This racial and ethnic disparity was further confirmed in the expansion of recommendation by the AAP task force [5]. The prevalence of supine positioning in 2010 among white infants was 75%, compared with 53% among black infants and parent-infant bed-sharing and use of soft bedding are also more common among black families vs. other racial/ethnic groups.
Multiple studies done in other institutions have established that the hospital setting provides an opportunity for health care workers to model risk-reduction [13–18] where parents are more likely to imitate infant sleep practices modeled by health care providers in a hospital setting [19–21]. Due to the at risk demographics, it was critical for the NICU team to cultivate a culture of safety during the infants hospital stay and to model SS to the parents.
Data collection is a learning process. The data collection tool used to collect baseline data values underwent multiple revisions and was finalized before the first PDSA cycle. Therefore, some of the specific data collected through the final version was not available in the baseline data values that affected the final measure of change. Therefore, it is likely that the baseline data for [Mb/Blanket] (Fig. 3) and [Me/No Item] (Fig. 4) is falsely high as specific and more data collected once the project was implemented were not available in the initial crib check tool.
Another one of the primary lessons learned was standardization of the metrics. This allows for more team players to do multiple roles. In April 2017, two of the main stakeholders were on vacation which is a plausible cause for the dip in SS compliance during that month. The team grew throughout the project to include more members accountable to the process and data collection.
As expected “change fatigue” set in June leading to another dip in the data values. The team proactively managed the situation by empowering the nurses with continued communication and positive reinforcement, re-education, utilizing feedback forms to identify reasons for lack of compliance and by entrusting ownership of the safety of the patients. One significant challenge identified by the team during this time was the decreased number of nurses that believe in the importance of SS while hospitalized in the NICU. This further led to the planning of the grand rounds and the small group discussions. The involvement of national and local leaders in SS increased personal motivation thereby making the practice of SS a personal responsibility for each nurse.
According to Charles Duhigg, author of the book “Power of Habit”, scientists proved that habit formation is a three step loop consisting of a cue, a routine and a reward. When a habit emerges, the brain stops fully participating in decision making. This effort saving instinct is an advantage that allows the brain to conserve its mental effort when performing basic behaviors. Following every feed, i.e. every three hours, the nurses are to put the baby back in exactly the same way each time. To practice SS effectively, consistently, and sustainably it was necessary for the team to help the nurses form the habit of SSP. At the beginning of habit formation, constant cues are an important component, once a habit is formed; it becomes automatic and does not require a lot of thought or reminders. Providing visual cues and reminders were found to be useful during this project. The team was consistent with rewarding the nurses with praise whenever SSP goals were achieved and with emphasizing their significant contribution to build a culture of safety. The challenge during this project was to help the staff form the habit of making the crib correctly every time, and to establish the new norm. By the end of July, the SS rates increased to 93% without the introduction of further reminders and remained > 90% throughout rest of the project duration. The team learned even though habit change or new habit formation among a team of individuals can be challenging, it can be done with constant reminders and cues, early in the process.
In the first month of initiation of the new EMR, documentation of SSE was 82%. It seems that this fell out of favor within the next few months prior to the project initiation, likely due to the nurses being overwhelmed with the complexities that occur with learning a new EMR system. Following the initiation of the project the median increased from 50 to 62%. Even though the project objective was fulfilled, the hospital mean was below average for that of the NYSPQC hospitals, for 2017 (90%). One of the reasons indicated was the lack of understanding and standardization of documenting in the specific patient care plan in EMR. Future direction includes re-education of SSE documentation and working with the IT department to include an order in EMR to document SSE to be acknowledged by the nurses. The team will continue to audit patient records to affirm improvement and assist nurses in reaching goals for SSE documentation.
Consistency among all team leaders was a key element in this successful project. Addressing all staff concerns patiently, while acknowledging the common team goal of providing safe care to patients, helped minimize any attitudinal barriers.
This project offers one institution’s multifaceted approach to the implementation of the AAP recommendations for infant SS positioning that addressed not only the physical factors but also the psychological factors that affect a culture change. One of our main strategies was habit formation and eliminating psychological and emotional factors that may contribute to overcoming resistance to change.
Future directions include formulating a handout for parents with data specific to our population to bring the gravity of this subject into perspective. The team believes bringing the data “closer to home” would make parents more alert to the harshness of the situation here in the Bronx and seriously consider practicing SS at home. In February 2019 Montefiore Wakefield Hospital received the New York State Perinatal Quality Collaborative (NYSPQC) Safe Sleep Project’s 2017 Quality Improvement Award in recognition of the hard work and dedication of our facility’s staff to improve safe sleep practices for infants.
Limitations
The baseline data were collected over 2 months prior to the project. Even though this may seem like a short duration of data collection, we had enough evidence that we needed to intervene sooner rather than later to improve SSP in the unit.
Balancing measures identified were concerns of hypothermia and reflux which would lead to prolonged hospitalization if the infants were placed in SS position. We were unable to reliably measure if our project made a difference in the rates of reflux or hypothermia in our patients. Even though data was collected both during the day and night shifts, the percentage collected during the night was much higher and the number of CC were more consistent. The team decided to use only the data from the night shift to avoid wide fluctuations in the number of CC done every month.
Conclusion
Multifactorial interventions significantly improved SS compliance among NICU nurses. Including data specific to the community in the education of the patient care team, gives better perspective of the problem at hand. Cultivating personal motivation among nurses, consistent empowerment and dedication to culture change by the entire team was crucial for the sustainability of the project.
Funding source
No external funding.
Potential conflict of interest
The authors have indicated they have no potential conflicts of interest to disclose.
Financial disclosure
The authors have indicated they have no financial relationships relevant to this article to disclose.
Footnotes
Appendix
Acknowledgments
The authors would like to acknowledge the nursing team, PCAs and nursing leadership at Wakefield NICU, particularly to nursing team leaders: Wilhemina Laryea, RN, MPH and Estela Pascua, RN for their significant contribution to this project and tireless efforts to distribute knowledge and skills among the staff. Sincere gratitude to the team leaders, Ann Nguyen, MD, Patricia Greene, NP, for their thoughts, ideas and support in data collection and the parents of the NICU babies for their acceptance and understanding of the importance of SSP. The authors commend the entire patient care team at Wakefield for their determination and commitment to be SS ambassadors.