
Abstract
OBJECTIVE:
Both preeclampsia and neuraxial anesthesia can alter placental perfusion, potentially affecting the neonatal status. The objective of our study is to quantify the association between type of neuraxial anesthetic and short-term neonatal morbidity among preeclamptic patients undergoing cesarean delivery.
METHODS:
We performed a secondary analysis of a prospective observational cohort study. Women with singleton gestations and a diagnosis of preeclampsia who underwent cesarean delivery with neuraxial anesthesia were included in the analysis. Short-term neonatal morbidities, defined as neonatal intensive care unit (NICU) admission, arterial cord gas pH ≤7.2 and 5-minute Apgar <7, were compared based on type of neuraxial anesthetic.
RESULTS:
A total of 4100 patients were included in the analysis, 1696 (41.4%) received spinal anesthesia 1848 (45.1%) received epidural anesthesia and 556 (13.5%) received a combined spinal-epidural (CSE). Antepartum and intrapartum characteristics significantly differed between the groups (p≤0.02). After adjusted analysis, spinal anesthesia was associated with reduced odds of NICU admission, compared with epidural or CSE (OR; 95% CI: 0.79; 0.63–0.98, 0.71; 0.53–0.94, respectively). Spinal anesthesia was also associated with lower odds of a 5-minute Apgar <7 compared with epidural anesthesia (OR 0.59; 95% CI; 0.43–0.83). We found no association between type of anesthesia and arterial cord pH ≤7.2. In stratiifed analysis by gestational age, no association between the type of neuraxial anesthesia and neonatal outcomes was noted among term infants, but associations persisted in preterm infants.
CONCLUSIONS:
Among women with preeclampsia undergoing cesarean delivery, spinal anesthesia may be associated with reduced short-term neonatal morbidity in preterm infants, compared with epidural or CSE.
Introduction
Preeclampsia and cesarean deliveries are common occurrences in obstetrics with preeclampsia affecting 3.4% of all pregnancies in the United States and cesarean deliveries accounting for 32.8% of all births in 2010 and 2011 [1, 2]. Similarly, neuraxial anesthesia is commonly used with 67.6% of labors and >95% of planned cesareans using neuraxial anesthesia [3, 4]. Despite these common obstetric occurrences, there is limited literature regarding their combined impact on neonatal outcomes.
Both preeclampsia and neuraxial anesthesia affect vascular tone and therefore may alter placental perfusion and impact fetal well-being. Preeclampsia is associated with sympathetic hyperactivity and damage to endothelial pathways in the setting of reduced intravascular volume [5]. These factors are thought to make women with preeclampsia especially vulnerable to sympathetic blockade-induced hypotension in the setting of spinal anesthesia, a complication which occurs in 64–100% of pregnant women undergoing cesarean [6, 7].
Neuraxial anesthesia is currently recommended for women with preeclampsia who require analgesia for labor and cesarean section [8]. The safety, efficacy and similar hemodynamic effects between the various neuraxial techniques in patients with preeclampsia demonstrated by several trials are the basis for these recommendations [9–12]. However, the small sample sizes limit the ability of these studies to detect differences in neonatal outcomes [9–12]. In the largest randomized trial comparing spinal versus epidural anesthesia at time of cesarean delivery in patients with severe preeclampsia, there were no differences in neonatal outcomes; however, this study was too small (N = 120) to detect differences in neonatal outcomes [12]. Thus, it remains unknown if the type of neuraxial anesthesia in patients with preeclampsia affects neonatal outcomes or if there are differential effects on the neonate that result from the type of neuraxial anesthetic to prevent unnecessary neonatal complications.
The objective of our study is to quantify the association between type of neuraxial anesthetic and short-term neonatal morbidity among preeclamptic patients undergoing cesarean delivery. We hypothesized that due to the vascular hyperactivity in patients with preeclampsia, the more rapid spinal-induced hypotension anesthesia would decrease placental perfusion and increase short-term neonatal morbidity, compared with epidural anesthesia or combined spinal-epidural anesthesia (CSE).
Methods
We performed a secondary analysis of a multicenter prospective observational study of primary and repeat cesarean deliveries conducted by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) Maternal-Fetal Medicine Units (MFMU) Network. Over a 4-year period, 19 U.S. academic centers participated in this cesarean registry. In 1999–2001, all women undergoing cesarean delivery or attempted vaginal birth after prior cesarean had data collected. In 2001 and 2002, only repeat cesarean deliveries and attempted vaginal births after prior cesarean had data collected [13]. Dedicated research nurses at each center abstracted information regarding medical and obstetric history, intrapartum course and infant outcomes from the maternal and infant charts. Full details of the methods of the original study have been previously reported [14]. The IRB at the University of North Carolina at Chapel Hill approved this secondary analysis.
Women with singleton gestations at ≥24 weeks, who underwent primary or repeat cesarean delivery, had a diagnosis of preeclampsia and received neuraxial anesthesia were included in this analysis (Fig. 1). Preeclampsia was determined via documentation in the clinical record, which was abstracted by trained research personnel at each center. Variants of preeclampsia, including hemolysis elevated liver enzymes low platelets (HELLP) syndrome, eclampsia and chronic hypertension with superimposed preeclampsia, were included in the analysis. Our exposure of interest was the anesthetic procedure used for cesarean delivery, determined from the clinical record. We included in our analysis women who received spinal anesthesia, epidural anesthesia or combined spinal-epidural (CSE) anesthesia as the first anesthetic administered (Fig. 1).
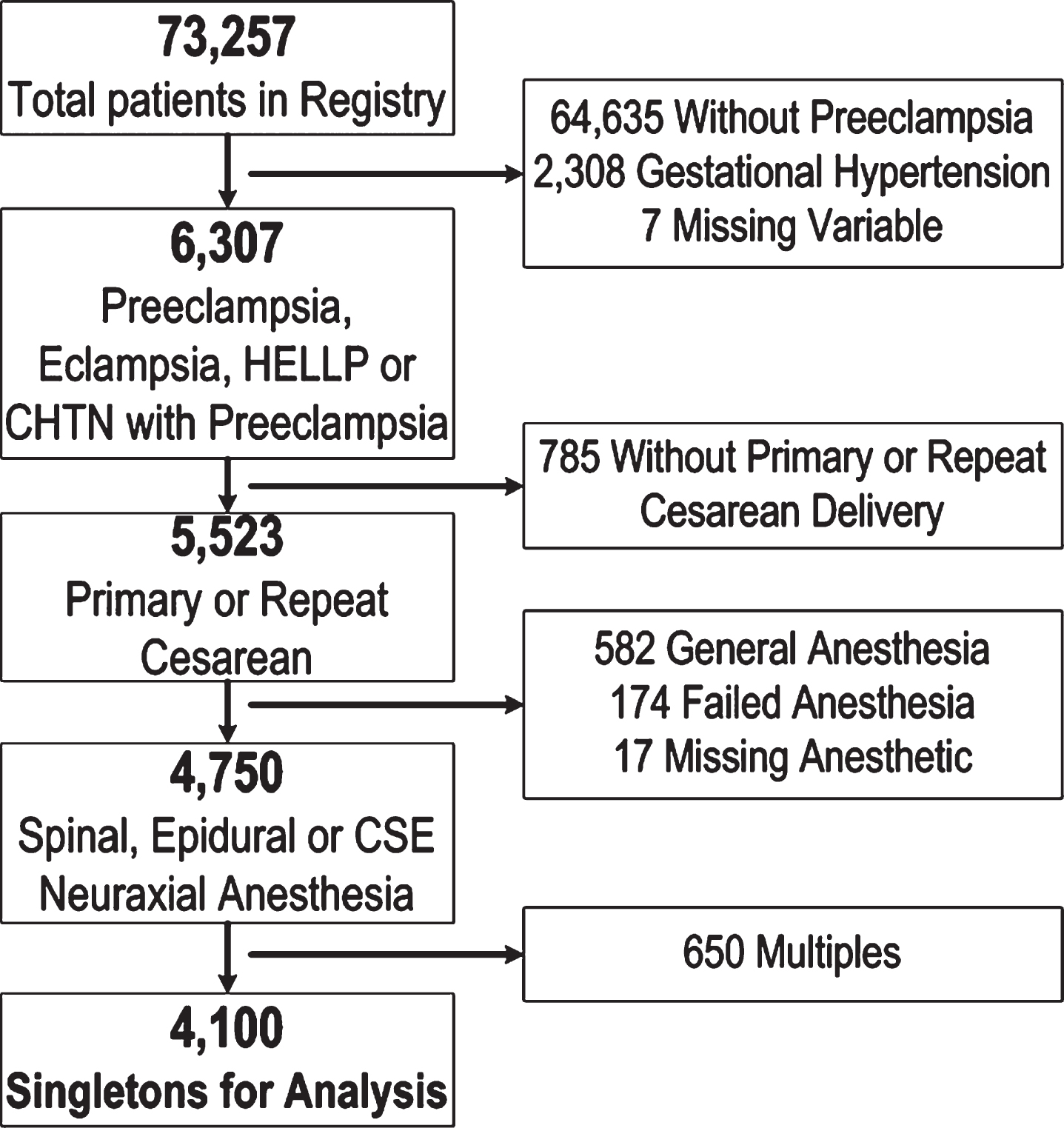
Patient flow.
Patients were excluded from the analysis if they had a multiple gestation, gestational hypertension, successful vaginal birth after cesarean, general anesthetic, failed neuraxial anesthesia or if the type of anesthetic was missing (Fig. 1). Maternal and obstetric conditions that may have affected our outcomes of interest were assessed, including maternal age, gestational age at delivery, body mass index at delivery at delivery (BMI, kg/m2), self-identified race, and American Society of Anesthesiologist (ASA) physical status as assigned by the obstetric anesthesia provider during preoperative assessment. Intrapartum characteristics collected included treatment with magnesium, presence of abruption, and chorioamnionitis. Operative characteristics included the type of cesarean delivery (primary or repeat), trial of labor prior to delivery, emergent delivery (defined as those operations with skin incision timed within 15 minutes of the first decision recorded to operate) [13], the time interval between skin incision and infant delivery, and the indication for the cesarean delivery. The data forms allowed each patient to have one major and one or two secondary indications for the cesarean delivery from an inclusive list of 20 pre-specified options that included “other” [15]. For the purposes of our analysis, only the major indication for cesarean was included and this variable was collapsed for the analysis into 6 clinically-related subcategories, including abnormal labor, fetal distress (including nonreassuring fetal testing and cord prolapse), abruption or previa, preeclampsia, elective (including prior cesarean), and other (including malpresentation, prior classical, vertical T or J incision, prior myomectomy, herpes, suspected macrosomia).
Our primary outcome was neonatal intensive care unit (NICU) admission. Secondary outcomes included clinically meaningful short-term neonatal morbidities of arterial cord pH ≤7.2, and 5-minute Apgar score <7. Assuming a 50% NICU admission rate, we calculated that 3210 total patients would be needed to detect a 5% difference between the groups, with 80% power and an alpha of 0.05.
Categorical variables were compared using χ2 for dichotomous variables and ANOVA for continuous variables. Odds ratios (OR) and 95% confidence intervals (CI) were determined for primary and secondary outcomes using multivariable logistic regression to control for the potential confounders of maternal age, birth weight, gestational age at delivery, number of prior cesareans, time between incision and delivery, type of delivery, magnesium treatment, race, abruption, chorioamnionitis, attempted labor, emergency delivery and indication for cesarean. As gestational age at delivery may independently affect NICU admission, stratified analyses for preterm (<37 weeks) and term (≥37 weeks) were completed. All P values reflect 2-tailed statistical analyses with statistical significance defined as P < 0.05. Data were analyzed using SAS software, version 12.0 (SAS Institute, Inc, Cary, NC).
Of the 73,257 patients in the registry, 4,100 patients met inclusion criteria and were included in the analysis (Fig. 1). Of these 4,100 patients, 1696 (41.4%) received a spinal, 1848 (45.1%) received an epidural and 556 (13.6%) received a CSE. Table 1 shows these three groups differed in baseline characteristics, including maternal age, BMI at delivery, race/ethnicity, ASA, number of prior cesarean deliveries, and gestational age at delivery(p < 0.01). The groups also differed in intrapartum characteristics, including treatment with magnesium, indication for cesarean, presence of chorioamnionitis, type of cesarean, attempted labor and emergent delivery (p≤0.02). Table 2 shows the neonatal outcomes of the study population, including birth weight, NICU admission, cord pH ≤7.2 and 5-minute Apgar ≤7.
Cohort characteristics
Cohort characteristics
Data expressed as n(%), mean(SD), or median(IQR). ASA, American Society of Anesthesiologists; NRFHT (non-reassuring fetal heart tracing). aData missing: BMI at delivery(248), ASA(84), number of prior cesarean(29), incision to delivery(727), gestational age(9). bOther includes: Malpresentation, prior classical, vertical T or J incision, prior myomectomy, herpes, suspected macrosomia.
Neonatal outcomes
Data expressed as n(%), mean(SD), or median(IQR). aMissing data: 5 Minute APGAR(3), cord pH (1941). bDeath within 28 days.
When comparing the three types of neuraxial anesthesia (Table 3), infants were more likely to be admitted to the NICU if the patient received spinal anesthesia compared to CSE anesthesia (unadjusted OR 1.35; 95% CI, 1.11–1.63) or epidural anesthesia compared to CSE anesthesia (unadjusted OR 1.23; 95% CI, 1.014–1.52), but no significant differences were noted when spinal compared to epidural anesthesia in the unadjusted model (unadjusted OR 1.07; 95% CI, 0.94–1.22). However, after adjustment for confounding variables, these associations changed as infants were significantly less likely to be admitted to the NICU if the patient received spinal anesthesia compared to CSE (aOR 0.71; 95% CI, 0.53–0.94) or spinal anesthesia compared to epidural anesthesia (aOR 0.79; 95% CI, 0.6–0.98). Rates of NICU admission were similar among patients receiving epidural anesthesia compared with CSE anesthesia (aOR 0.9; 95% CI, 0.8–1.2) (Table 3).
Odds ratios for neonatal outcomes comparing types of neuraxial anesthesia
OR, odds ratio; CI, confidence interval. aAdjusted for number of previous cesarean, birth weight, gestational age at delivery, incision to delivery time, maternal age, type of delivery, magnesium treatment, race, abruption, chorioamnionitis, attempted labor, emergency delivery and indication for cesarean. bAdjusted for number of previous cesarean, birth weight, time interval between incision to delivery, maternal age, indication for delivery, magnesium, abruption, chorioamnionitis, attempted labor, emergent delivery.
Infants of patients having epidural anesthesia were significantly more likely to have 5-minute Apgar scores <7 than those with spinal (aOR 0.59; 95% CI 0.4–0.83) (Table 3). This association with 5-minute Apgar was not noted when the other groups were compared. No significant associations in arterial cord gases pH ≤7.2 were noted among the groups (Table 3).
After stratifying by gestational age at delivery, the association between NICU admission persisted only for infants delivered preterm when spinal anesthesia was compared with CSE anesthesia (aOR 0.54; 95% CI 0.34–0.87). When spinal anesthesia was compared with epidural anesthesia, the association with decreased odds of 5-minute Apgar <7 persisted (aOR 0.66; 95% CI 0.6–0.96) (Table 4). However, no association between the type of neuraxial anesthesia and neonatal outcomes was noted among the subgroup of term infants (Table 4).
Odds ratios for neonatal outcomes comparing types of neuraxial anesthesia stratified by gestational age
OR, odds ratio; CI, confidence interval aAdjusted for type of cesarean, magnesium, race, abruption, chorioamnionitis, attempted labor, emergent delivery, indication for cesarean delivery, number of prior cesarean, birth weight, maternal age, time interval between incision to delivery and gestational age. bAdjusted for number of previous cesarean, birth weight, time interval between incision to delivery, maternal age, indication for delivery, magnesium, abruption, chorioamnionitis, attempted labor, emergent delivery.
In this large multicenter sample of patients with preeclampsia delivering via cesarean, spinal anesthesia, when compared with epidural anesthesia or CSE, was associated with reduced short-term neonatal morbidities including NICU admission and 5-minute Apgar <7. This association appeared to persist in preterm infants after stratification by gestational age. These findings were contrary to our initial hypothesis.
Our findings confirm and extend earlier work regarding neuraxial anesthesia among women with preeclampsia. We hypothesized that spinal anesthesia would induce greater hypotension in patients with preeclampsia, but this may not be the case. Aya et al demonstrated that the incidence of significant hypotension leading to ephedrine treatment was less in patients with severe preeclampsia undergoing spinal anesthesia for cesarean delivery compared to normotensive patients [6]. Specifically the sympathetic hyperactivity and decreased endothelial-dependent relaxation of small resistance vessels, which contribute to the hypertension seen in preeclampsia, could create widespread vasoconstriction that may not be altered by spinal anesthesia [6]. Thus, these patients might maintain a high vascular tone, limiting the decrease in blood pressure during spinal blockade. Thus, contrary to our hypothesis, placental perfusion may be preserved in those receiving spinal anesthesia and hence account for the observed associations with neonatal outcomes in preterm infants.
Although we cannot conclusively state which method of neuraxial anesthesia confers any neonatal benefit, we feel that these data do support the neonatal safety of spinal anesthesia among patients with preeclampsia undergoing cesarean delivery. Our observations are similar to findings by Wallace et. al., who concluded in a small randomized trial that general or regional anesthesia are equally acceptable for cesarean delivery in patients with severe preeclampsia [10]. These authors did not demonstrate serious fetal effects from maternal circulatory changes induced by sympathetic blockade, but the study was not powered to detect fetal acidosis, which they defined as ph <7.19 [10]. Similarly, Visalyaputra et al, in a randomized control trial of 120 severe preeclamptics, found no clinically significant difference in hypotension with spinal versus epidural [12]. In addition, no difference in neonatal outcome was apparent, as the duration of hypotension was short [12]. Both of these trials were underpowered to detect any differences in neonatal outcome. Although not a randominized control trial, our study contributes to the literature by having a sample size large enough to analyze any differences in neonatal outcomes by type of neuraxial anesthesia.
Our results should be interpreted within the context of the study design. This is a secondary analysis of a data set designed to measure complications of cesarean birth, and potentially important clinical variables were not collected, such as maternal blood pressures prior to delivery, the dose of anesthetic agent and block levels, the use of blood pressure support (e.g. phenylephrine, ephedrine) during neuraxial anesthesia placement and the amount of intravenous prehydration prior to neuraxial anesthesia. It is plausible spinal anesthesia was not administered in women thought to be at high risk of reduced placental perfusion, and the apparent protective effect of spinal anesthesia might reflect confounding by indication. In addition, the intent, indication, and dosing of the CSE technique were not collected. It is increasingly common to use low-dose or sequential CSE for patients with severe preeclampsia. While this is a limitation, the results were favorable for CSE in this study, considering that the cases were full dose CSE anesthetics used at the time of cesarean. Strengths of our study include the large size of the cohort and the validity of the database, as well as the inclusion of data from multiple US centers, which increase the generalizability of our results.
As preeclampsia and cesarean delivery remain very common obstetric occurrences, it is important to understand if the choice of neuraxial anesthesia affects neonatal outcomes. The choice of anesthesia in patients with preeclampsia is likely to be driven by other uncontrollable clinical factors, such as maternal obesity, anesthesia provider skills and preferences, number of prior cesareans and emergent delivery. However, acknowledging the limitations of this study, in term infants, there was no apparent difference in neonatal outcomes and short-term neonatal morbidities did not appear to be increased. In preterm infants, short-term neonatal morbidites, such as NICU admission and 5 minutes Apgar <7, may potentially be decreased by the use of spinal anesthesia rather than epidural anesthesia among patients with preeclampsia who undergo cesarean delivery.
Disclosure statement
a. Financial Disclosure Statement: There are no potential or actual interests relevant to the topic discussed in this manuscript to disclose.
b. Human Research Statement: We affirm that this research was conducted in acordance with the ethical standards of all applicable national and institutional commitees and the World.
c. Animal Research Statement: NA
d. Other Disclosure or Disclaimer Statment(s): Funding source: NC TRACS Grant # 2KR451217.
Footnotes
Acknowledgments
None.