
Abstract
INTRODUCTION:
High frequency jet (HFJV) and oscillatory (HFOV) ventilation were used to rescue newborns with congenital diaphragmatic hernia (CDH), who failed conventional mechanical ventilation (CV). Changes in ventilator settings and pulmonary gas exchange were evaluated following transition to high frequency ventilation (HFV).
METHODS:
Records of patients with CDH rescued with HFV prior to surgical intervention between 2006 and 2015 were reviewed. Mean airway pressure (Pāw) and arterial blood gases during CV and those obtained within the first hour of HFV were compared. A composite repeated measure analysis was performed to evaluate longitudinal and intergroup variances.
RESULTS:
Twenty-seven patients were rescued from CV, 16 by HFJV and 11 by HFOV. The two groups had similar gestational ages and birth weights. Prior to HFV, both groups had similar Pāw, PaCO2, FiO2 and PaO2. HFV was associated with a significant improvement in ventilation, and the rate of decrease of PaCO2 was no different between groups. There was a significantly higher increase in Pāw increase with HFOV compared to HFJV.
CONCLUSIONS:
In newborns with CDH rescued with HFV, ventilation improved but Pāw was significantly lower in patients supported with HFJV compared to HFOV.
Introduction
High frequency jet (HFJV) and oscillatory (HFOV) ventilation deliver lower than pulmonary dead-space volumes at rapid rates and have unique flow dynamics [1, 2]. A conventional mechanical ventilator is used in tandem with HFJV to provide positive end expiratory pressure and sigh breaths. Exhalation is passive in HFJV and exhalation is active in HFOV. Other differences in the basic characteristics of these two devices are described by Keszler et al [3]. Both modalities of HFV have been used to support newborns with congenital diaphragmatic hernia (CDH), who fail conventional mechanical ventilation (CV) [4]. Some centers utilize HFOV as the initial form of ventilation to support infants with CDH [5, 6] and as part of a management plan that aims to provide “gentler ventilation” and to deliver inhaled pulmonary vasodilators [7]. Other centers choose to use HFOV to rescue infants with CDH who fail CV [8], a practice that is accepted by many international experts [9]. In some centers, more than half of patients with CDH are treated with HFOV [10]. In a recent large randomized controlled trial (RCT) comparing CV and HFOV as the initial ventilation strategy for CDH, HFOV did not provide improvement in the primary outcome (death or bronchopulmonary dysplasia), and the HFOV group had a longer duration of mechanical ventilation and treatment with vasopressors. On the other hand, there are fewer clinical reports of successful support of infants with severe CDH with HFJV [11-13].
In a study done in normal adult cats, Boros et al., reported that at equivalent proximal Pāw, HFJV produced better ventilation and oxygenation with higher cardiac output (CO) compared to HFOV [14]. Traverse et al evaluated Pāw and cardiac output using HFJV and HFOV on adult cats. Some of the animals underwent surfactant washout by bronchial lavage to reduce lung compliance. They reported lower Pāw using HFJV [15]. These investigators also found that increased Pāw adversely affected CO with both modalities and concluded that cardiovascular effects of mechanical ventilation depend mainly on the Pāw rather than the type of ventilation. These potential cardiovascular benefits encouraged some clinicians to use HFJV during open heart and Blalock-Taussig surgical procedures [16, 17].
Many infants with CDH have significant hemodynamic problems stemming from severe pulmonary hypertension and systemic hypotension [18]. Altit et al found that in infants with CDH and pulmonary hypertension, the need for extracorporeal membrane oxygenation (ECMO) was associated with decreased left and right ventricular function, suggesting that interventions to improve cardiac output may reduce the need for ECMO [19].
In this retrospective review, we evaluated ventilator pressure changes and markers of gas exchange following transition from CV to HFV. We hypothesized that these changes would be unique to the specific modality of HFV.
Methods
We conducted a retrospective review of the medical records of patients with severe CDH between 2006 and 2015 at Michigan Medicine’s Brandon Neonatal Intensive Care Unit. We included patients who were transitioned from CV to either HFJV or HFOV for more than 30 minutes prior to surgical repair or support with ECMO. We compared mean airway pressure (Pāw) and arterial blood gases on CV to those obtained within the first hour of HFV. Ventilators included the AVEA® ventilator (Vyaire Medical, Mettawa, IL, USA), the SensorMedics 3100A high frequency oscillator (Vyaire Medical, Mettawa, IL, USA) and the Life Pulse High Frequency Jet Ventilator (Bunnell Inc., Salt Lake City, UT, USA) in tandem with CV.
The neonatology service supervised the stabilization after birth of infants with CDH. The type of HFV chosen to rescue infants with hypercarbia or hypoxemia during CV was determined by the clinician. Since 2010, a protocol for pulmonary management of infants with a CDH, similar to that described by Tracy et al [20], was adopted.
Paired t-tests (Wilcoxon matched-pairs signed rank test) were used to compare changes within the HFJV and the HFOV groups following the transition from CV. Univariate comparisons of continuous variables were done using the Mann Whitney test. A composite repeated measure analysis evaluated variance longitudinally and between groups. We used IBM SPSS Statistics 19 (SPSS Inc., Chicago, Ill., USA) and GraphPad Prism version 7 (GraphPad Software, La Jolla, California USA).
This project was approved by the medical institutional review board.
Results
Of the 130 patients with CDH, 44 patients were rescued with HFV (HFJV 27, HFOV 17) at any time before ECMO or surgical repair and included patients supported with HFV immediately after birth. Of the 44 patients, 27 were switched from CV to HFV for more than 30 minutes and had arterial blood gases done before and within an hour of switching to HFV (HFJV 16, HFOV 11), met study criteria, and were available for analysis. The two groups (HFJV and HFOV) had similar gestational ages and birth weights. Patient characteristics, pulmonary support, and outcomes are summarized in Table 1. Infants in the HFJV group more frequently had liver in the thoracic cavity (75% vs. 36%) and less frequently had left-sided CDH (56% vs. 91%) compared to the HFOV group. Infants in the HFOV group were more frequently treated with inhaled nitric oxide (iNO) (36%) prior to surgical intervention compared to those in the HFJV (6%) group.
Descriptive characteristics
Descriptive characteristics
amean ± SD, OI = oxygenation index, out born = born outside then transferred to the study center.
Prior to switching to HFV, both groups had similar Pāw, PaO2, and FiO2 . The mean values for oxygenation index (OI) and PaCO2 were statistically different. There were no statistically significant differences in the rates of ECMO (69% vs 73%), death in the hospital (44% vs 45%), or the duration of support with mechanical ventilation, or hospital stay between the HFJV and HFOV groups. The rate of pneumothorax (19% vs 27%) between the two groups prior to repair or support with ECMO was not statistically significantly different. There were 2 patients in the HFJV group and 2 patients in the HFOV group who had either very severe pulmonary hypoplasia, extreme prematurity, or a combination of lethal anomalies, who were not offered support with ECMO and subsequently died after redirection of care within the first 1-4 days.
HFV in general was associated with a statistically significant improvement in ventilation (p = 0.001). The rate of decrease in PaCO2 was no different between HFJV or HFOV on composite repeated measure analysis (p = 0.991). However, using a paired t-test, there was a greater variation in the change in PaCO2 within the HFOV group, and the change in PaCO2 was only statistically significant within the HFJV group (Table 2 and Fig. 1).
Changes in Pāw and gas exchange following switch to HFV
aexpressed in (mean ± SD); P = paired t-test, Wilcoxon matched-pairs signed rank test, comparing changes within the HFJV or the HFOV groups; bComposite repeated measure analysis to evaluate variance longitudinally [P1 = Comparing changes from CV (n = 27) to HFV (n = 27)] and between groups [P2 = Comparing degree of changes between HFJV (n = 16) and HFOV (n = 11) following switching to HFV].
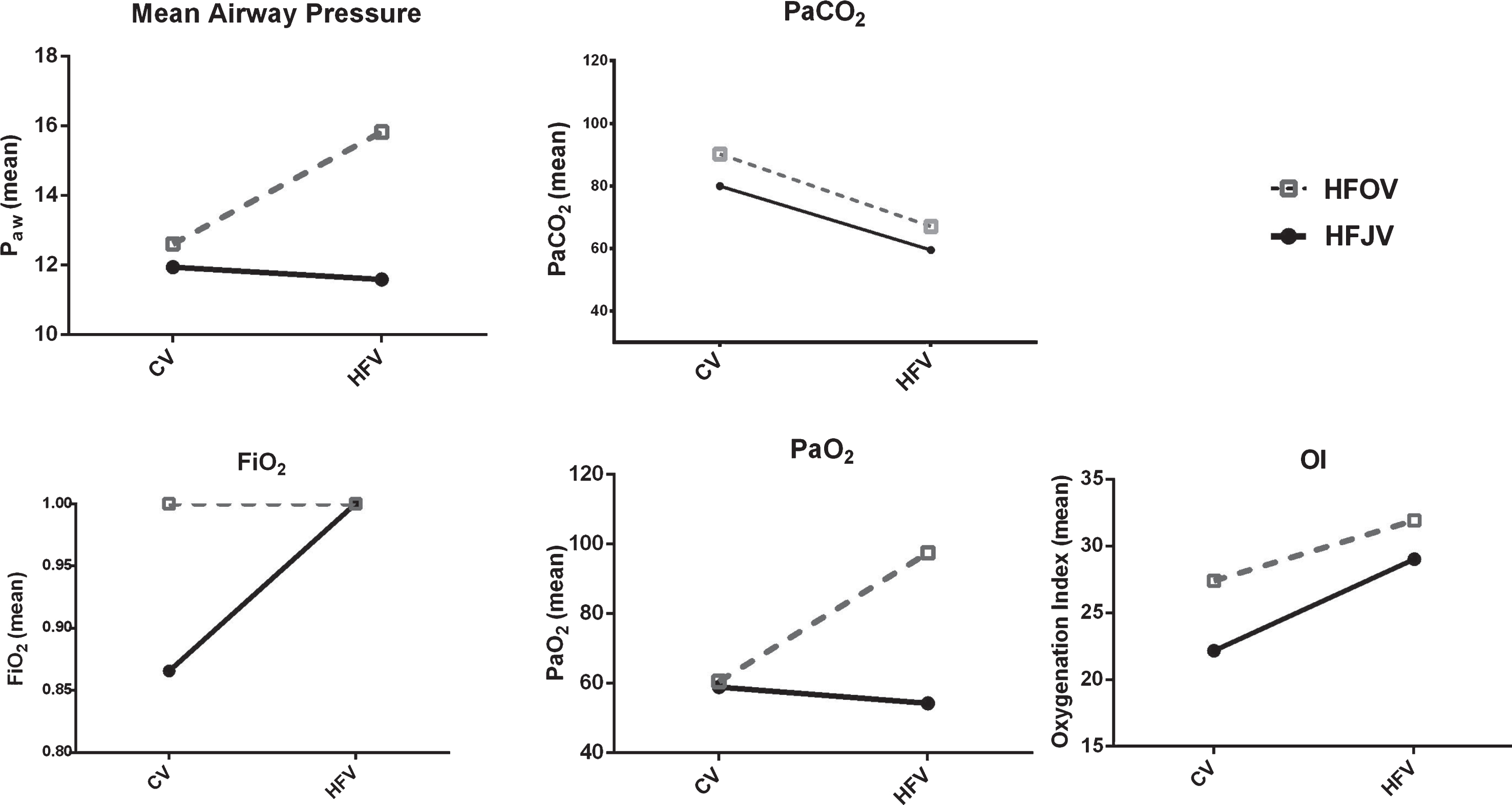
Mean airway pressure, PaCO2, FiO2, PaO2, and OI during conventional mechanical ventilation (CV), just before transition to high frequency ventilation (HFV), and within one hour of HFV (expressed in means). HFOV shown with open box and HFJV shown in filled circles.
There was a statistically significant increase in Pāw following the switch to HFOV but no significant change in Pāw following the switch to HFJV.
There was no significant increase in PaO2 following the switch to HFOV or HFJV; however, PaO2 was associated with a large variation within the HFOV group. There was no significant change in FiO2 following the switch from CV to HFV. Oxygenation index significantly increased following the switch to HFV (p = 0.017), but the degree of change was not different between the HFJV and the HFOV groups.
In this cohort of newborns with CDH supported with CV then rescued with HFV, ventilation improved significantly during HFV. Although, the rate of decrease in PaCO2 was not statistically different between HFJV and HFOV, the decrease in PaCO2 within the HFJV cohort was statistically significantly better and the change within the HFOV group did not reach statistical significance. Infants supported with HFJV did not have a significant reduction in Pāw, but those supported with HFOV had a significant increase in Pāw following the switch from CV. On the other hand, as PaO2 did not significantly change in the HFJV group following the switch from CV, infants in the HFOV group had an increase in the average PaO2, but this change was not statistically significant (nor was rate of change in PaO2) between the groups. Our data suggest that HFJV is a better choice of HFV to improve ventilation in patients with severe CDH and may carry the advantage of doing so at a lower Pāw. HFOV may have an advantage of improving oxygenation and ventilation in some patients but at the cost of utilizing a higher Pāw. We were unable to retrieve data that might be useful markers of hemodynamic function, in part because of our interest in describing short term changes (within one hour) during HFV and it would be challenging to interpret changes in blood pressure, use of vasoactive agents, and intravascular volume expanders utilized over this short period of time. Variables that better predict cardiac output might be derived from serial echocardiography, but those were not collected as part of routine care [18, 19]. These variables should be part of future prospective trials to evaluate high frequency ventilation for infants with CDH and respiratory failure.
Other investigators who compared changes in ventilation, oxygenation, and Pāw in patients or animal models with respiratory failure utilizing CV, HFJV, and HFOV also reported differences between these modalities of ventilation. Zhang et al. reported that infants with CDH switched from HFOV and CV to HFJV had a significant reduction in PaCO2 [13]. In a small (n = 24) RCT comparing CV to HFJV for infants with respiratory failure and persistent pulmonary hypertension, Engle et al., reported better oxygenation and ventilation in the HFJV group. The mean Pāw appeared lower in the HFJV group but the difference was not statistically significant [21]. Carlo et al., in a retrospective case control study of infants with severe respiratory failure and pulmonary hypertension, also reported lower Pāw and PaCO2 in the infants supported with HFJV compared to CV [22]. In a multicenter RCT comparing the use of CV and HFJV for infants with pulmonary interstitial emphysema, Keszler et al. also reported lower Pāw and lower PaCO2 in the HFJV group [23]. While a large RCT comparing initial support of infants with CDH with HFOV and CV did not specifically report on Pāw, PaCO2, or echocardiographic markers of cardiac output in the two groups, the HFOV group required vasoactive medications for a longer period of time [24].
The retrospective nature of our study report is also limited by a small number of patients and subsequently some differences in patient characteristics between the two groups might not have reached statistical significance from a type two error. In addition, some of the parameters that might be used as markers of cardiac output were not collected. Mechanical ventilation management, including the high frequency modalities, are to some extent operator dependent, which adds to the limitations of this observation. Standardized ventilator management guidelines for infants with CDH should be utilized in the design of future studies of HFV in CDH. While there is great interest in the role of vasoactive medications in the treatment of pulmonary hypertension [18], use of a ventilation modality with lower Pāw, like HFJV, might further improve cardiac output. In the meantime, our observations may be useful to clinicians stabilizing infants with CDH. HFJV might be the modality of choice when these infants exhibit hypercarbia and hemodynamic instability during CV.
Disclosure statement
The authors have no conflicts of interest to declare.