
Abstract
OBJECTIVE:
To determine the association between hemodynamic instability requiring inotropes and brain injury or death in neonates with hypoxic ischemic encephalopathy (HIE).
METHODS:
Retrospective cohort study of 221 neonates with HIE. Brain injury was defined using four HIE patterns based on MRI diffusion or T1 changes. The primary outcome was death or brain injury. Secondary outcomes were abnormal MRI, death, and abnormal EEG. Logistic regression was used to examine the risk of death or brain injury with the use of inotropes while adjusting for confounding factors.
RESULTS:
Brain injury or death occurred more often in neonates who received inotropes (71.1%, 69/97) compared to those who did not (44.3%, 55/124). The use of inotropes was associated with increased risk of death or brain injury (OR 3.11; 95% CI 1.39–7.004) and abnormal MRI (OR 2.78; 95% CI 1.22–6.34) after adjusting for confounding factors. Mortality was significantly higher in neonates exposed to inotropes (21.6%, 21/97) compared with those who did not receive inotropes (4%, 5/124), P < 0.001.
CONCLUSION:
In infants with HIE, hemodynamic instability requiring inotropes in the first 72 hours of life was associated with increased risk of death or brain injury detected by MRI.
Keywords
Abbreviations
Hypoxic Ischemic Encephalopathy
Magnetic Resonance Imaging
Electroencephalogram
Therapeutic Hypothermia
Diffusion Weighted Images
Apparent Diffusion Coefficient
Introduction
Despite widespread improvements in neonatal care and the introduction of therapeutic hypothermia (TH), the incidence of neonatal encephalopathy and long term neurological morbidity due to Hypoxic-Ischemic Encephalopathy (HIE) remains high [1–7]. One of the proposed mechanisms for brain injury in HIE is based on a two phase theory of hypoperfusion and reperfusion [8–11]. The timing and duration of hypoperfusion and transition to adequate reperfusion depends on several factors including preconditioning, severity of insult, and timing of obstetrical and neonatal interventions. These factors vary between patients, making identification of the stage of injury and prediction of outcome, difficult. Furthermore, there is conflicting data in the literature about the definitions and prevalence of hemodynamic instability in patients with HIE. However, studies do demonstrate decreased cardiac output, significant changes in the peak systolic, diastolic and mean blood flow velocities in the middle and anterior cerebral arteries, along with changes in the resistive indices (RI) in infants with HIE. In prior studies these changes were shown to vary based on the severity and the stage of injury [12, 13]. Little is known about the effects of TH on cardiac output and neonatal brain perfusion [14, 15], which poses challenges in the selection, dosage and timing of inotrope use. The safety of inotrope usage in HIE and especially while undergoing TH is yet to be eestablished [16].
The aim of our study was to investigate the association between brain injury and mortality, and the early use of inotropes in neonates with HIE.
Methods
We performed a retrospective cohort study of patients admitted between July 2008 and February 2016 to the level III neonatal intensive care units (NICUs) at Foothills Medical Centre and Alberta Children Hospital in Calgary, Alberta. The primary outcome was death or brain injury on Magnetic Resonance Imaging (MRI). The secondary outcomes were: abnormal MRI, death, and abnormal electroencephalogram (EEG) background and or electrographic seizures.
The study was approved by Conjoint Health Research Ethics Board, ID REB13-1247 and consent was waived.
The diagnosis of HIE was made at the time of admission to the NICU by the attending physician using the diagnostic criteria in Table 1 following the local therapeutic hypothermia guideline.
Inclusion and exclusion criteria for moderate to severe neonatal HIE diagnosis
Inclusion and exclusion criteria for moderate to severe neonatal HIE diagnosis
Any inotrope use (dopamine, dobutamine, epinephrine, and or hydrocortisone) was defined as exposure during the first 72 hours of life. Use of inotropes was at the discretion of the attending physician, however at our institutions we use the TH guideline, which defines hypotension as a mean arterial blood pressure below 40 mmHg for more than 30 minutes in term infants, as an indication to initiate pressor support. Data on the type and duration of inotropes used were extracted. At our institutions the local guidelines recommend dopamine as first line therapy, followed by dobutamine and epinephrine as alternatives for refractory hypotension. Hydrocortisone is typically used in hypotension unresponsive to escalating doses of vasoactive drugs. In addition to hypotension as a prime indication, inotropes, were also used if there was poor cardiac contractility by echocardiography, irrespective of whether there was concomitant hypotension. In these cases, the first line inotrope is dobutamine followed by dopamine if hypotension was present.
Primary outcome measurement
Brain MRI
All MRI studies were carried out without pharmacological sedation on a Siemens 1.5 tesla Avanto scanner. Routine MR sequences obtained were: sagittal and axial T1W, axial and coronal FSE T2W, axial and coronal Diffusion Weighted Images (DWI) and Apparent Diffusion Coefficient (ADC) maps, axial T2* GRE, as well as axial 3D volumetric T1W with reformats. Single-voxel MR spectroscopy (2×2×2 cm) was performed using TE135 with voxel positioning over the left basal ganglia.
A neuroradiologist (JS) unaware of the severity of clinical categorisation of HIE read the MRI images performed in two windows: 1) a diffusion window at the 4-5th day of age (post cooling), and 2) a T1 weighted window at the 7–14th day of age. Brain injury was diagnosed based on the presence of abnormalities on DWI sequence and ADC maps, or T1 signal shortening. The MRIs were scored using a previously validated scoring system [17], and were categorised as follows (Fig. 1): (1) Injury mainly to the basal ganglia with sparing of the white matter, (2) Injury to the white matter with sparing of the basal ganglia, (3) Injury to both the basal ganglia and white matter (4) Multifocal signal abnormalities that do not fit the above three patterns of injury.
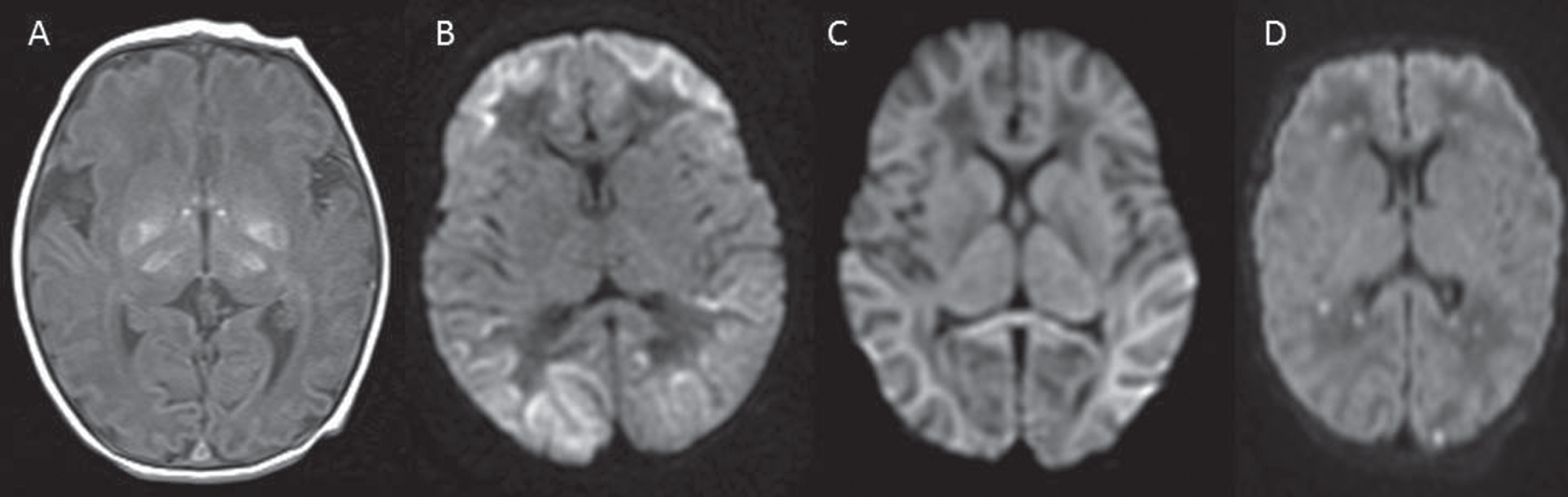
HIE patterns on MRI. A. Acute profound asphyxia: basal ganglia T1 shortening sparing the white matter. B. Partial prolong asphyxia: bilateral diffusion weighted image changes in the white matter sparing the basal ganglia. C. Total asphyxia: diffusion weighted image changes in basal ganglia and white matter involvement. D. Multifocal: multiple small restricted diffusion areas on the diffusion weighted image.
The MRI imaging with the most severe injury pattern was used to define the final diagnosis of brain injury.
Neonatal EEG
A 60-minute EEG was performed usually within the first 12 hours of age, subsequent EEGs were requested at the discretion of the provider using standard 10–20 electrode placement method with 19 electrodes plus the physiologic electrodes to evaluate sleep state, detect artifact, and detect autonomic function for all patients. EEG was done even if the baby did not qualify for TH. EEGs were evaluated for: background activity, epileptiform transients and electrographic seizures. A board certified pediatric epileptologist interpreted the EEG studies using Standardized EEG report template. In August 2013, continuous video EEG was introduced for routine care of patients with moderate to severe HIE. We used the worse background activity or the presence of seizure at any point in the first 72 hours as the final diagnosis.
The diagnosis of abnormal EEG (Fig. 2) was defined as the presence of: (1) isoelectric signal, (2) burst/suppression pattern, (3) discontinuous background and (4) electrographic seizures with or without clinical correlate.
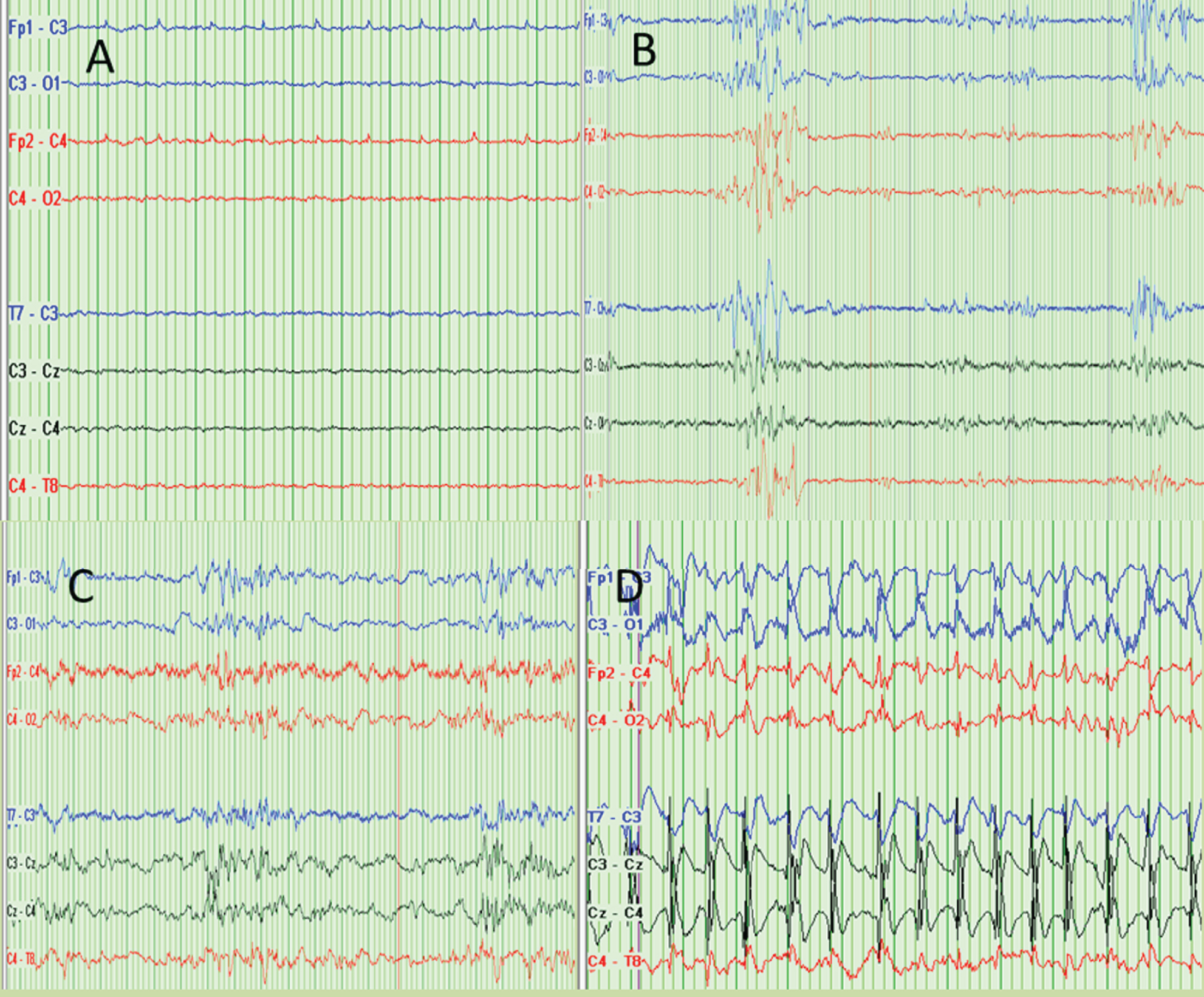
Abnormal EEG patterns. A. Isoelectric. B. Burst suppression. C. Discontinuous. D. Electrographic seizure.
Clinical seizures and the use of anti-seizure medications (including initial and maintenance) and/or sedation were documented. Routine EEG was repeated after rewarming or if clinically indicated.
All statistical analyses were performed with IBM SPSS version23. The tests used were two-sided and significance was defined as p-value <0.05 and alpha was set at 5%. Univariate and bivariate statistics were used to describe the sample. Baseline characteristics were expressed as count and percentages for categorical variables and mean and SD for continuous variables. Categorical variables were compared by Fisher’s exact test or chi-square test and continuous variables by Student’s t test (two-sided) if normally distributed and Mann Whitney U test if not normally distributed. For our analyses, the outcome of interest was death or abnormal MRI.
Logistic regression was performed to examine the association between use of inotropes and death or abnormal MRI. Confounding factors like gestational age (GA), birth weight, birth outside the referral tertiary centre, cord blood gas pH, Apgar score at 10 minutes of age, HIE clinical stage, use of anti-seizure medication, use of sedation, and TH, were controlled for in the analysis. The association between patient characteristics and death or abnormal MRI was also examined. As this study was exploratory in nature we did not correct for multiple comparisons. We repeated the regression analysis after; first excluding the mild HIE cases then excluding severe HIE cases. Finally, we included only moderate HIE cases to address the concern that hemodynamic instability requiring inotrope use was a marker of disease severity rather than risk for brain injury.
Power calculation
221 subjects with the diagnosis of HIE were identified from the NICU database. Preliminary analyses found an absolute difference of 26% in any MRI abnormality or death between patients treated with inotropes and those not treated with inotropes. Given a total sample size of 221 subjects this study had 97% power with a two-sided alpha of 0.05 to detect a 26% absolute difference in MRI abnormality or death between subjects with inotrope use and those without inotrope use.
Results
Patient characteristics
Over the seven and half year period 221 cases with HIE were identified in our cohort, median GA was 40 weeks (IQ 38–40), mean birth weight was 3250 grams (IQ 2877–3600), and 53% of the babies were male. Further, mean cord pH was 6.99 (IQ 6.86–7.15). One hundred and twenty eight infants were classified as Sarnat Stage II, 57 as Stage I, and 36 as Stage III. One hundred and forty-six infants (146/221; 66.1%) received TH. More than half of the infants (146/221; 66.1%) were out born. Clinical chorioamnionitis was reported in only 14 cases (14/221; 6.3%). One hundred and fifty-one infants (151/221; 68.3%) received a narcotic infusion (morphine or fentanyl) for sedation.
Use of inotropes and HIE (Table 2)
Ninety-seven infants (97/221; 43.9%) received at least one inotrope within the first 72 hours of life. The most common inotropic agent was dobutamine (88/221; 39.8%) followed by dopamine (61/221; 27.6%), while epinephrine and hydrocortisone were used infrequently (4% and 5.4% respectively). Median duration of inotrope use was 60.5 hours; IQ 31–83.8. Neonates who received inotrope support were of significantly lower gestational age (p = 0.038) and had a significantly lower cord pH (p = 0.003). Infants treated with inotropes were also more likely to be HIE Stage III, treated with TH, receive more sedation, and be diagnosed with persistent pulmonary hypertension of the newborn (PPHN).
Antenatal and postnatal risk factors and outcomes compared between 2 groups: Inotropes versus non inotrope treated group
Antenatal and postnatal risk factors and outcomes compared between 2 groups: Inotropes versus non inotrope treated group
*= p < 0.05.
Neonates receiving inotropes had a significantly higher incidence of death (21 cases) compared to those not receiving inotropes (5 cases) (p < 0.001).
Use of inotropes and death and/or brain injury as determined by death, abnormal MRI or abnormal EEG
Use of inotropes and death and/or brain injury as determined by death, abnormal MRI or abnormal EEG
*= p < 0.05.
The likelihood of an abnormal brain MRI was significantly higher in the inotrope group (62/90; 69.6%), compared to the non-inotrope group (55/113; 48.6%), p = 0.004. Further, those in the inotrope group were significantly more likely to have an abnormal EEG (32/45; 71.1%) compared to the non-inotrope group (22/51; 43.1%) (p = 0.006).
With regression analysis, hemodynamic instability requiring inotropes use was associated with a significant increase in the risk of death or brain injury (OR 3.11; 95% CI 1.39–7.004) and brain injury alone (OR 2.78; 95% CI 1.22–6.34), after adjusting for gestational age, birth weight, being out-born, cord blood gas pH, APGAR score at 10 minutes, HIE clinical stage, use of anti-seizure medication, use of sedation, and TH. Hemodynamic instability requiring inotropes was also associated with increased risk of abnormal EEG (OR 1.36, 95% CI: 0.69–7.84), but this was not statistically significant.
Adjusting for confounding factors, longer duration of inotrope use was not associated with higher risk of death or brain injury (OR 1.00, 95% CI: 0.99–1.01), abnormal MRI (OR 1.00, 95% CI: 0.99–1.02), or abnormal EEG (OR 1.01, 95% CI: 0.99–1.03).
However, hemodynamic instability requiring more than one inotrope was associated with an increased risk of death or brain injury (OR 1.94, 95% CI: 1.25–2.99), abnormal MRI (OR 1.76, 95% CI: 1.13–2.75), and abnormal EEG (OR 2.43, 95% CI: 1.13–5.21).
Discussion
In this retrospective cohort study we explored the association between hemodynamic instability requiring inotropes and the incidence of death or brain injury in patients with HIE prior to and following the introduction of TH in our institutions. Our study showed a significant increase in the risk of death or brain injury, after adjusting for confounding factors, in babies exposed early to inotropes during TH.
The core concept in cerebral autoregulation is that the intracranial arteries and arterioles constrict or dilate relative to changes in systemic blood pressure to maintain stable brain perfusion. Under normal circumstances this is largely an inverse relationship. However, beyond the normal ranges of blood pressure, cerebral circulation becomes pressure passive, meaning that the higher the systemic blood pressure the greater the blood flow to the brain and vice versa [18–20].
In intact healthy term newborns, the physiological principles of cerebral autoregulation are thought to follow similar principles to those of adults with the exception of two very important caveats. The first of these is that the cerebral autoregulation curve is shifted to the left as the “point” where the system becomes more pressure-passive is lower compared to adults [21–23]. Secondly, cerebral auto regulation in neonates is labile and more prone to changes in the clinical response curve [24, 25]. For example, hypoxic-ischemic insult impairs cerebral autoregulation capacity even after initial recovery [26], through mechanisms that are incompletely understood.
With these concepts in mind, prediction of the effect of inotropes on compromised cerebral autoregulation with hypoxic-ischemic injury is difficult, especially with the inability to identify the phase of brain injury and acceptable cerebral perfusion parameters to minimise secondary injury and optimise recovery [16, 27]. Studies have shown that inotropes, especially dopamine, through its alpha adrenergic effect, may cause intracranial vasoconstriction and blunt cerebral autoregulation thereby making these drugs potentially harmful when used in the reperfusion stage of HIE [28, 29]. In our study, the use of dopamine was associated with increased odds ratio (OR 3.98; P = 0.002) of brain injury. Dobutamine, on the other hand, may increase stroke volume and cardiac output, which can increase brain perfusion in the absence of cerebral autoregulation. Our study showed an increase in brain injury when dobutamine was used (OR 3.12, p = 0.005). An earlier study showed a significant increase in brain injury seen on MRI in preterm infants treated with inotropes [30].
Abnormalities in cerebral function, determined on neurological examination or on ancillary tests such as EEG, can be indicative of brain injury. More recent research has supported the use of continuous video EEG monitoring to increase the likelihood of identifying clinical and subclinical seizures [31]. In our institution, a 60 minute long EEG was performed soon after admission and repeated after rewarming or at the discretion of the clinician. The relatively short and variable EEG recording time may explain why our study did not identify a statistical difference in electrical seizure activity between the inotrope treated and the untreated group. The sensitivity of brief EEG recordings in reliably identifying electrographic seizure activity is dependent on timing of the EEG, use of therapeutic hypothermia, and stage of HIE [32–34].
Based on results from our study, the early use of inotropes may be a marker of hemodynamic instability and disease severity. Alternatively, it is possible that the use of inotropes may exacerbate brain injury by exceeding the natural capacitance of cerebral autoregulation mechanisms. Our results demonstrated a consistent association between use and number of inotrope use and brain injury on MRI, after adjusting for illness severity by excluding severe and mild cases of HIE.
Limitations
This was a retrospective study with inherent selection biases, therefore causation between the use of inotropes in the first 72 hours and death or brain injury cannot be conclusively established. Further prospective studies are required to establish the safety of inotropes in neonates with HIE especially while undergoing TH. In addition, our definition of hemodynamic instability and the choice of inotropes, was based on institutional guidelines and clinician preferences, which vary between institutions. Finally, the clinical staging of HIE is subject to inter-observer variability and may vary between institutions.
Conclusion
Our study identifies an association between hemodynamic instability requiring use of inotropes and the risk of death or brain injury in neonates suffering from hypoxic ischemic encephalopathy.
Disclosure statement
The authors declare that they have no conflict of interest to disclose.
Funding source
No external funding provided for work on this study.
Financial disclosure
None.
Conflicts of interest
The authors have no conflicts of interest to disclose.