
Abstract
BACKGROUND:
The objective of this study was to determine factors associated with long-term intermittent positive pressure ventilation (IPPV) in extremely preterm infants.
METHODS:
Study setting was a ten bed pod (SBP) part of the Level IV all referral NICU, dedicated to the care of infants born at <27 weeks and which utilizes a protocol-driven approach to care. All admissions to the SBP from 2005 to 2011 were included if admitted in the first week of life and alive at 56 days of age.
RESULTS:
There were 210 patients and 35% were on IPPV for ≥56 days (for the purposes of this study defined as long-term IPPV). Long-term IPPV patients were born earlier, had lower birth weight, were admitted later, and more likely to come from a level III NICU. LTV patients were more likely to have a PDA ligation, receive dopamine, receive TPN longer, and receive supplemental oxygen at 36 weeks PMA. In logistic regression modeling transfer from another Level III NICU (OR 3.7, 95% CI 1.5–9.2, p = 0.006) and recieveing dopamine (OR 3.1, 95% CI 1.5–6.3, p = 0.002) were associated with long-term IPPV.
CONCLUSIONS:
In this cohort of infants born at <27 weeks gestation 35% were on long term IPPV. There are identifiable factors known on admission and occurring during the NICU stay that are associated with long-term IPPV.
Keywords
Introduction
Preterm infants often have respiratory distress at, or soon after, birth requiring intermittent positive pressure ventilation (IPPV). Although IPPV saves lives, it is also associated with the development of lung injury leading to bronchopulmonary dysplasia (BPD) [1, 2]. BPD is the most common chronic lung disease affecting preterm infants, and was first described in 1967 by Northway et al. [3] as a fibroproliferative disease with 4 classic stages. Improved neonatal intensive care practices including surfactant and antenatal steroids have led to the emergence of a “new” BPD characterized by fewer and larger alveoli, as well as decreased pulmonary microvasculature development [2, 5]. It remains difficult to define BPD, and currently utilized definitions are based on need for supplemental oxygen. The consensus definition of BPD [6] is widely utilized and defines BPD in patients born at <32 weeks as a need for supplemental oxygen at 28 days of life and then stratifies severity into mild, moderate, or severe based on the need for supplemental oxygen at 36 weeks post menstrual age (PMA). Regardless of the definition used [7], the incidence of BPD has not changed dramatically over time, perhaps due to improved survival of the smallest preterm infants [2, 5].
Extremely preterm infants usually need respiratory support for lung disease and/or refractory apnea of prematurity. There is data to suggest that extubation and placement on nasal continuous positive airway pressure (nCPAP) will decrease the incidence of BPD without increasing mortality [8–12]. However, the decision to extubate the extremely preterm infant is difficult, particularly in the quaternary care setting where co-morbidities often influence this decision. This may contribute to the finding that the incidence of BPD is inversely related to gestational age at birth [2, 13]. Furthermore, the extremely preterm infant is more likely to require prolonged courses of IPPV [14, 15]. We hypothesized that there would be factors identifiable at admission or during the hospitalization that would be associated with prolonged mechanical ventilation in preterm infants born at <27 completed weeks of gestation. To study this hypothesis we utilized the small baby database, which contains information for all babies born at <27 weeks admitted to the small baby pod (SBP) at Nationwide Children’s Hospital.
Subjects and methods
All neonates admitted to the SBP between 12/26/2004 and 12/30/2011 were evaluated. The study was approved by the Institutional Review Board of Nationwide Children’s Hospital. Nationwide Children’s Hospital does not have a labor and delivery service, thus the NICU and SBP consists entirely of outborn patients. Nationwide Children’s Hospital has the only Level IV neonatal intensive care unit (NICU) in the region and therefore patients are referred from level III NICUs in Franklin County when a higher level of care is required, for example a pediatric sub-specialty consult (neurology, infectious diseases, cardiology, etc.) or a pediatric surgery consult (general surgery, neurosurgery, otolaryngology, urology, etc.). Patients are also referred for on-going NICU care from delivery hospitals without neonatology coverage outside of Franklin County. Thus, birth in Franklin County is used as a surrogate for transfer from another Level III NICU, since all delivery hospitals in Franklin County have a Level III NICU, while none of the delivery hospitals outside of Franklin County have Level III NICUs. Furthermore, it should be noted that the SBP uses an interdisciplinary, family-centered, and guideline-driven approach to care [16–18].
Patients were included if they were admitted in the first week of life and survived to 56 days of life. We used 56 days as our cut-off for long-term mechanical ventilation based on previous studies suggesting that approximately 25% of extremely preterm infants needed mechanical ventilation for ≥56 days (15,17,18). Data collected included county of birth, birth weight, gestational age, Apgar scores, age of admission, age at discharge, treatments received in the NICU, total days on IPPV, total days on nCPAP, and the development of morbidities such as necrotizing enterocolitis (NEC), intraventricular hemorrhage (IVH), and BPD. The diagnosis of NEC was based on the modified Bell’s criteria. The diagnosis of IVH was taken from the head ultrasound reports and the worst grade reported is used; we defined severe IVH as grade III or IV. We utilized the consensus definition of BPD [6]. Additional hospital outcome data included length of stay and discharge on oxygen.
Statistical analysis
Data are shown as median and intraquartile range [IQR], or as percentages. Groups were compared using a Mann-Whitney Rank Sum test for nonparametric data. Categorical data was compared between groups using Fisher’s Exact Test. Multiple logistic Regression modeling was done for those factors found to be significantly different between groups. All statistical tests were run using Sigmaplot 12.5 (Jandel Scientific, Carlsbad, CA). Differences were considered significant if p < 0.05.
\enlargethispage 12pt
Results
There were 277 patients admitted to the SBP in the first week of life and 210 who survived to 56 days of life. Of these 210 patients, 137 (65%) patients received IPPV for <56 days and 73 patients (35%) received IPPV for ≥56 days (Fig. 1). The distribution of total IPPV days is shown in Fig. 2 as the cumulative number of patients for given IPPV days. Twenty-five percent of patients had 13 or fewer total IPPV days, 50% of patients had 37 or fewer total IPPV days, and 90% of the patients had 92 total IPPV days or fewer. The IPPV days were not necessarily consecutive, indeed 72% of the patients in this cohort were re-intubated after an initial successful extubation, and there was no difference between groups (76% in the <56 days group and 65% in the ≥56 day group, p = 0.13) in the need for re-intubation.
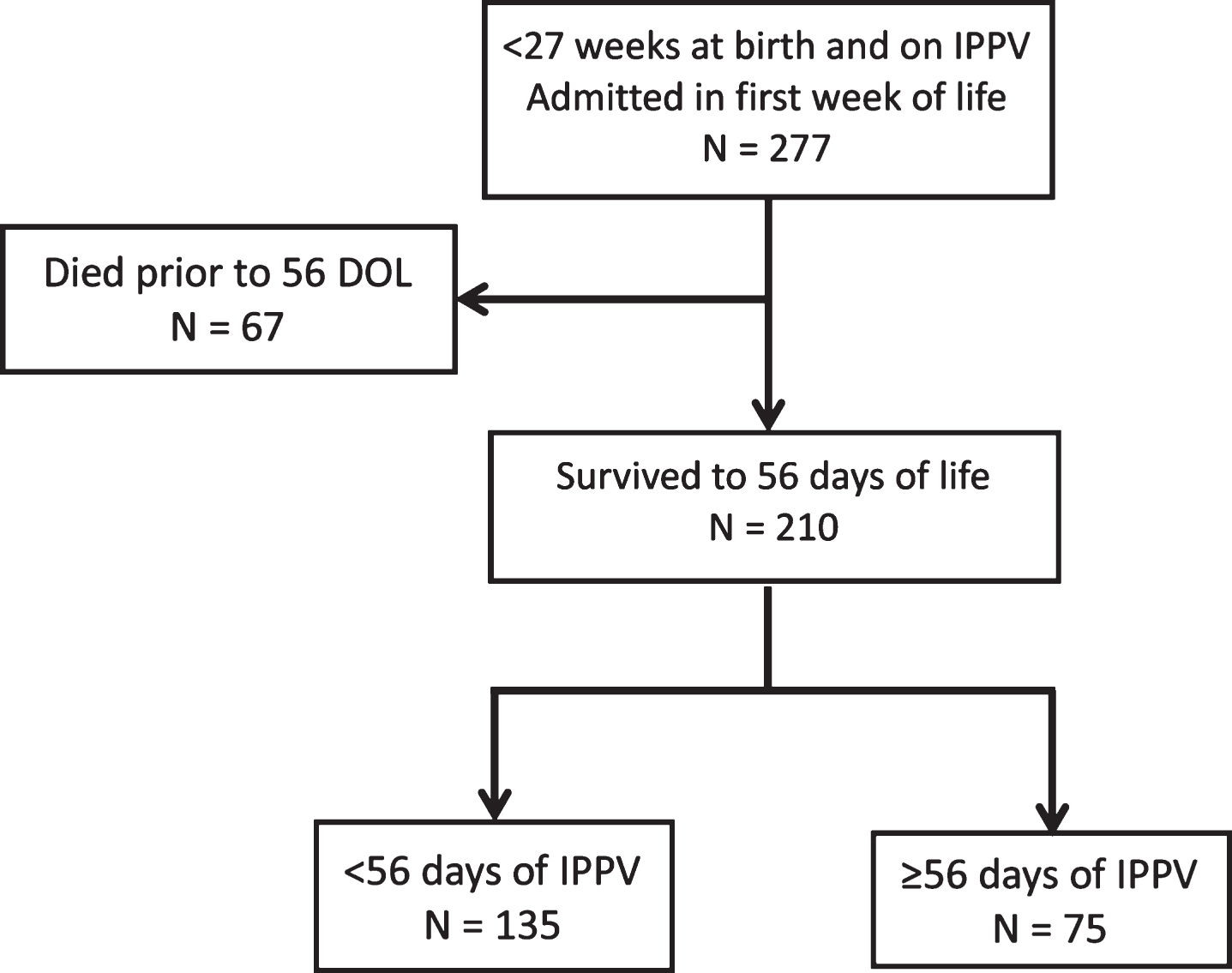
Eligible patients were born at <27 weeks, admitted in the first week of life, and survived to 56 days of life. 277 patients admitted in the first week of life and 210 (76%) survived to 56 days, of which 75 (36%) were on IPPV for ≥56 days.

Distribution of total IPPV days in the entire cohort of <27 week infants. There were 4 patients who never received IPPV and 4 patients who received IPPV for >200 days, max IPPV days was 292. The median of the total IPPV days was 37 with an IQR of 13–71.
The characteristics on admission to NCH for the two groups are shown in Table 1. The gestational age at birth and the birth weight were significantly lower in the ≥56 days IPPV group than in the <56 days IPPV group. The Apgar scores at 1 and 5 minutes were not different between the two groups. The patients in the <56 day IPPV group were admitted earlier and less likely to be transferred from a Level III NICU.
Admission characteristics
DOL, day of life; NICU, neonatal intensive care unit.
Patients on IPPV for ≥56 days generally had greater acuity than patients on IPPV for <56 days during their NICU stay. Table 2 shows the NICU therapies and morbidities these patients received. The majority of these extremely preterm infants received prophylactic indomethacin although there was no difference between the two groups. There was no difference in the number of patients who received a treatment course of indomethacin, although there were significantly more patients in the IPPV for ≥56 days group that had a PDA ligated. There was no difference between groups regarding the age of the patients when PDA ligation occurred. Dopamine was used more frequently and for longer periods of time in the patients who received IPPV for ≥56 days than in those with IPPV for <56 days. IVH, severe IVH, and PHH were more common in patients requiring ≥56 days of IPPV than in those with <56 days of IPPV. There was no difference in the incidence of NEC between the two groups. The length of stay was substantially longer for patients requiring ≥56 days of IPPV than for those with <56 days of IPPV. The mortality in the NICU after DOL 56 for these patients was substantially greater in those patients requiring ≥56 days of IPPV than in those patients with <56 days of IPPV.
NICU therapies and morbidities
PDA, patent ductus arteriosus; DOL, day of life; IVH, intraventricular hemorrhage; PHH, post-hemorrhagic hydrocephalus; VP, ventriculoperitoneal; NEC, necrotizing enterocolitis.
Logistic regression modeling was carried out to determine if there were factors that would be predictive of need for IPPV for ≥56 days. We first looked at those admission characteristics (Table 1) that were different between the two groups. Of the 6 factors used in the model only being transferred from a Level III NICU was significant (OR 4.17 (95% CI 1.45–12.01); p = 0.008) in predicting need for IPPV ≥56 days. We then looked at all of the NICU therapies and characteristics (Table 2) that were different between the two groups except length of stay and mortality. Of the 5 factors used in the model (dopamine days did not have enough entries for the model to converge) only dopamine use was significantly (OR 2.82 (95% CI 1.38–5.75); p = 0.004) associated with need for IPPV for ≥56 days. We then utilized the 5 factors in Tables 1 and 2 that were different between groups with a p-value<0.001, which included transfer from a Level III NICU and dopamine use, in a logistic regression model. The results of the model are shown in Table 3 and being born at a facility with a level III NICU and dopamine use during the NICU increased the risk for needing IPPV for ≥56 days by ∼3-fold.
Multiple logistic regression modeling
Respiratory outcomes
As expected the respiratory outcomes between groups were different as shown in Table 4. As expected, the median IPPV days were substantially greater, nearly 4 times greater, in the IPPV ≥56 days group than in the <56 days group. The incidence of tracheostomy placement was more than 6-fold greater in the ≥56 days IPPV group than in the <56 days IPPV group. The incidence of any BPD was high in both groups and there was no difference between groups. The incidence of moderate/severe BPD was greater in the ≥56 days of IPPV group than in the <56 days group. The need for positive pressure (either IPPV or nCPAP) at 36 weeks PMA was substantially higher in the ≥56 days IPPV group than in the <56 days IPPV group. Nearly all patients in the ≥56 days IPPV group were discharged to home on supplemental oxygen, while ∼two-thirds of the <56 days IPPV group were discharged to home on supplemental oxygen (p < 0.001).
Our data demonstrate that in infants born at the edge of viability admitted to an all referral Children’s Hospital in the first 7 days of life relatively long durations of IPPV are not uncommon. Indeed, we found that 50% of infants born at <27 weeks had >37 total IPPV days during their hospitalizations. The median IPPV days for the entire 210 patients surviving to 56 days was 37 with an IQR of 13–71. This is comparable to a recent report from the Children’s Hospital’s Neonatal Consortium which found that babies born at ≤27 weeks admitted to NICUs in Children’s Hospitals had median ventilator days of 39 with an IQR of 16–69 [15]. It should also be pointed out that 50% of patients had fewer than 37 total IPPV days and that 25% of the cohort had fewer than 13 days of total IPPV. Given that the average length of stay for the entire cohort was 134 days, this suggests that the infant born at <27 weeks referred to a Children’s Hospital early in the NICU course spends a considerable portion of their initial NICU stay on IPPV. Although, for most infants the total IPPV days are not consecutive and need for multiple courses of IPPV did not increase the likelihood of needing 56 days or more of total IPPV.
Our patients are a sub-set of all extremely preterm infants, in that the patients included in this cohort had to survive the delivery room and transfer to an all referral NICU. Thus, this cohort of patients is not a cross section of all extremely preterm infants born in our region, and does not include patients who died in the delivery room, in the referral NICU, or who never developed conditions or co-morbidities that required tertiary/quaternary care. We have previously shown that for this all referral population the rate of moderate/severe BPD is relatively high [14]. This relatively high rate of moderate/severe BPD is consistent with other studies in extremely preterm infants. For example, Stoll [19] using Neonatal Research Network data found in a birth cohort of 8,515 patients born at <29 weeks gestational age in 2003 to 2007 that the incidence of moderate/severe BPD was 41% . The Express Study [2] found that in a birth cohort of infants born at <27 weeks in Sweden the incidence of any BPD was 73% and severe BPD was 25% . Natarajan et al. [20] using data from the Neonatal Research Network found that the incidence of severe BPD was 46% in infants born at <27 weeks.
Our data support our hypothesis that there are factors identifiable at admission associated with prolonged IPPV in preterm infants born at <27 completed weeks gestational age. Factors that would be known on admission to a Children’s Hospital that were more likely to occur in patients needing longer term IPPV included lower gestational age and birth weight, referral from another level III NICU, and greater age on admission. However, when used in a multiple logistic regression the only factor that remained significant was being transferred from another Level III NICU, which increased the odds of needing ≥56 days of IPPV by ∼4 times. We have previously found in our SBP that infants transferred from other Level III NICUs have a greater severity of illness than those admitted from Level I or II nurseries [17]. We also found that, although “sicker” than small babies transferred from Level I or II units, small babies transferred from other Level III NICUs had a better survival rate [17, 18]. It is also of interest that although the patients that received ≥56 days of IPPV were born earlier and weighed less at birth, that in this particular cohort of patients born at the limits of viability neither gestational age nor birth weight were predictors of requiring longer IPPV durations in the multiple logistic regression modeling. This may be due to the relatively limited gestational age range studied in this cohort (i.e. 22 to 26 weeks).
Our data also support that there are factors identifiable during the NICU stay that are associated with prolonged mechanical ventilation in preterm infants born at <27 weeks gestational age. As perhaps expected in the light of data suggesting that PDA ligation increases the risk for BPD [21], we found that patients requiring ≥56 days of IPPV were more likely to have a PDA ligation than were those with <56 days of IPPV. The median time of PDA ligation was ∼2 weeks of age and did not differ between groups. Dopamine use was also greater in the patients with ≥56 days of IPPV, as was the median number of days that dopamine was used, than in patients with <56 days of IPPV. We also found that IVH was more common in patients requiring longer IPPV. When used in a multiple logistic regression model the only NICU factor that was significant was the use of dopamine, which increased the risk of needing ≥56 days of IPPV by 3-fold. This is consistent with a previous report from our group that demonstrates that dopamine use is a predictor of mortality in patients admitted to the SBP [18]. It is likely that dopamine treatment is a marker of disease severity in these patients. Larger trials will be necessary to determine if low blood pressure per se is a risk factor for subsequent development of severe BPD.
We also found that in these patients born at the edge of viability that the mortality rate after 56 days of life and prior to discharge from the NICU was substantially greater in the patients who received ≥56 days IPPV than in those who received <56 days IPPV. Although the NICU mortality rates after 56 days for both groups were relatively low. This is consistent with a previous study examining factors associated with in-hospital mortality in patients born at <27 weeks wherein we found that 50% of mortality occurred by day 21 of life [18], and a report by the EXPRESS Group [22] where 81% of NICU death occurred in the first week of life in patients born at <27 weeks. We recently reported in a cohort of patients weighing <1500 grams and requiring at least 30 days of IPPV that mortality after 30 days of life was 11% [23]. In a recent report on BPD and neurodevelopmental follow-up in patients born at <27 weeks who survived to 28 days, we reported a mortality rate of 9% between 29 days and 18 months of age, with 61% of all mortality occurring between 29 days and 36 weeks PMA [14]. Interestingly in that study [14], we found that only patients on supplemental oxygen died, and those that were weaned to room air had no mortality. In this study, we found that the mortality rate for patients not on IPPV at 56 days was <1% . These findings suggest that the need for prolonged IPPV and supplemental oxygen increases the risk of later death in extremely preterm infants.
Receiving ≥56 days of IPPV was also associated with worse outcomes. The patients with prolonged IPPV had more IVH, more severe IVH, and were more likely to have PHH than patients who received <56 days of IPPV. The length of stay was greater in those patients with ≥56 days of IPPV than in those patients with <56 days of IPPV. As expected the group of patients who received ≥56 days of IPPV all had BPD, and had a significantly higher rate of moderate/severe BPD than did those patients with <56 days of IPPV, indeed only one patient in the ≥56 days of IPPV group had mild BPD. In fact, 80% of the patients who received ≥56 days of IPPV were on positive pressure at 36 weeks PMA compared to only 20% of patients with <56 days of IPPV.
In conclusion, we found that long-term IPPV is not uncommon in our cohort of infants born at <27 weeks gestational age. Factors known on admission associated with long-term IPPV include lower gestational age and birth weight, referral from another level III NICU, and greater age on admission. Factors known during the early NICU stay were also associated with long-term IPPV including PDA ligation, dopamine treatment, duration of dopamine treatment, and IVH. In multiple logistic regression modeling only dopamine treatment and transfer from another Level III NICU were significantly associated with need for IPPV for ≥56 days. These findings suggest that larger trials to develop predictive models are feasible and that such predictive models could likely identify extremely preterm infants at the highest risk for developing severe BPD to accelerate the development of preventative therapies.
Disclosure statements
Financial disclosure statement
The authors have no conflicts of interest to disclose.
Human research statement
The authors affirm that the research involving human subjects described in this manuscript was conducted in accordance with the ethical standards of all applicable national and institutional committees and the World Medical Association’s Helsinki Declaration.
Footnotes
Acknowledgments
The authors would like to thank Nick Foor and Margaret Holston for their help with the data collection for this study. We would also like to thank the staff of the Small Baby Pod at Nationwide Children’s Hospital for their continued dedication to improving long-term outcomes for our smallest patients.