
Abstract
BACKGROUND:
Legacy-making, actions or behaviors aimed at being remembered, may be one strategy to enhance coping and improve grief outcomes for bereaved parents and siblings. While legacy interventions have been developed and tested in pediatric and adult populations, legacy activities specific to bereaved parents in the neonatal intensive care unit remain unexplored. This study explored bereaved parents’ perceptions of a digital storytelling legacy-making intervention for parents after the death of an infant.
METHODS:
Six bereaved mothers and fathers participated in a focus group interview three to 12 months after the death of an infant in the NICU. A semi-structured interview guide with open-ended questions was used to obtain parent self-reports. Qualitative content analysis identified emerging themes.
RESULTS:
Four major themes emerged regarding participants’ perceptions of a legacy intervention: (a) parents’ willingness to participate in a legacy intervention, (b) parents’ suggestions for a feasible intervention, (c) parents’ suggestions for an acceptable intervention, and (d) parents’ perceived benefits of legacy-making.
CONCLUSIONS:
Participants reported that a legacy-making intervention via digital storytelling would be feasible, acceptable, and beneficial for NICU parents. Study results support the need and desire for legacy-making services to be developed and offered in the NICU.
Introduction
Expert care for seriously-ill or premature infants has been provided in neonatal intensive care units (NICUs) since the 1960s. Approximately 12% of the four million babies born in the U.S. each year are cared for in the NICU. Of these, 11% are born premature, and 1% have significant illnesses that require NICU care [1]. NICU care may be supportive, palliative, or surgical and is lifesaving for many infants. On the other hand, neonatal death is an unfortunate reality within the NICU. Neonatal death is classified as death within the first twenty-eight days of life, and is most commonly caused by premature birth, low birth weight, and birth defects. In 2015, the United States had a neonatal mortality rate of four per every 1000 live births. With an estimated four million births per year, approximately 16,000 babies died in the NICU during 2015 [2].
Although bereaved parents can experience positive growth, they are high risk for significant negative consequences such as marital disruptions [3], psychopathology [4], and mortality [5]. Having an infant in the NICU often requires large amounts of time spent at the hospital and many decisions involving the care of the infant as well as siblings [6]. The NICU environment is foreign and intimidating and can be tremendously frightening to parents. Grieving parents may experience physical and emotional symptoms including fatigue, insomnia, aches, chest pain, nausea, shortness of breath, anxiety, and panic attacks [3, 6]. Emotional symptoms (e.g., sadness, helplessness, guilt, anger) may occur as bereaved individuals move through the stages of grieving including denial, anger, bargaining, depression, and acceptance. Grief can also create a source of toxic stress that can have damaging effects on one’s immune system [7]. The death of a child is not only significant in the present, but it also symbolizes the loss of a future for families [8].
Growing research has examined bereavement programs in the NICU, needs of bereaved parents, perspectives and needs of siblings, and nurses’ understanding and perceptions of bereavement services in the NICU [9–13]. Studies have noted the importance of physical representations of deceased infants, supporting the need for bereavement programs that enable families to create and collect physical representations of their children. Parents have emphasized that it was important to “receive mementos such as photographs, handprints, footprints, casts, or clothes” [11].
Legacy-making, defined as memory making, or doing and saying things to be remembered [14], may be one strategy to enhance coping and improve grief outcomes for bereaved parents and siblings. Previous work suggests that legacy-making activities may be important and helpful for terminally-ill adults [15] and bereaved parents and siblings who experienced the death of a child from cancer [14]. However, studies exploring legacy-making with samples of bereaved parents who experienced the death of an infant cared for in the NICU have not been conducted. While legacy interventions have been developed and found feasible for adults and children living with cancer [14–19], such interventions have not been developed or tested in populations of bereaved NICU parents. The overall purpose of this study was to explore bereaved parents’ perceptions of a legacy-making intervention for parents after the death of an infant.
Methods
Participants
Of ten eligible and contacted bereaved families, three (30% ) participated in the focus group. Participants (N = 6) included three mothers and three fathers. Parents averaged 29.50 years of age (SD = 6.35), and 100% (n = 6) were White and non-Hispanic. Deceased infants were all female (100% , n = 3) and averaged 1.67 (SD = 2.08) days of age. Two (67% ) infants were considered non-viable, and one (33% ) was viable. Data were collected 10 to 11 months (M = 10.33, SD = 0.58) post-death.
Of the 7 families who declined participation, four (57% ) infants were considered viable and three (43% ) non-viable. Reasons for refusal included schedule conflicts with the scheduled date and time (n = 3), too busy in general/not interested (n = 2), concern with sensitive topic related to currently expecting another baby (n = 1), and not interested in a group interview although willing to do an individual interview (n = 1).
Procedures and measures
The principal investigator (PI) collaborated with the physician division director of the NICU to develop study procedures. Institutional Review Board approval was obtained prior to beginning study recruitment. The PI obtained a list of the names of deceased infants by contacting the palliative care nurse who manages the NICU database. Eligible participants were (a) bereaved parents (legal guardians 18 years of age and up) of infants who received care or died in the NICU, (b) between 3 to 12 months after the death of their infant, and (c) able to speak and understand English.
The PI determined families who likely met the inclusion criteria based on dates of infant deaths, discussions with the medical team, and review of medical records. The PI prepared participant introductory letters to be reviewed and signed by the attending physician or NICU department head; this served as a screening process for physicians who worked with the families to screen out any families they felt would not be good candidates for the study. Physicians screened out two eligible families in this study. The PI mailed letters to families that were signed by physicians. The letters included an opt-out number/email for families who wish not to be contacted further, although no families opted out. The PI called families two weeks after letters were mailed to describe the study in further detail, answer any questions, and determine parents’ interest to participate. New participants were invited until six parents agreed to attend, with the goal to have six to eight participants based on Krueger’s focus group techniques [20]. To increase participation, participants received a reminder phone call, text, or email one to two days prior to the focus group. (Fig. 1. Recruitment process).
After all focus group participants arrived, the PI (experienced in conducting and consenting bereaved parents for research) explained the study and consent materials and answered questions. After verbal and written consent, participants individually completed a demographic questionnaire that included the parent caregiver’s gender, age, race, marital status, educational level, and deceased child’s date of birth (month and year only) and date of death (month and year only). The PI began the group interview by asking an ice-breaker question to decrease potential participant anxiety. Next, the PI presented the intervention idea to participants by describing and showing video examples of digital stories created from previous work in pediatric oncology [19]. The PI then used a semi-structured interview guide with open-ended questions to obtain self-reports from the bereaved parents regarding their suggestions for developing the intervention content, their acceptability of the intervention, and their willingness to participate in such an intervention. The focus group lasted approximately 60 minutes and was conducted using Krueger’s focus group techniques [20]. The focus group interview was conducted in a private living room style conference room at a school of nursing. The interview was audiotaped and later transcribed.
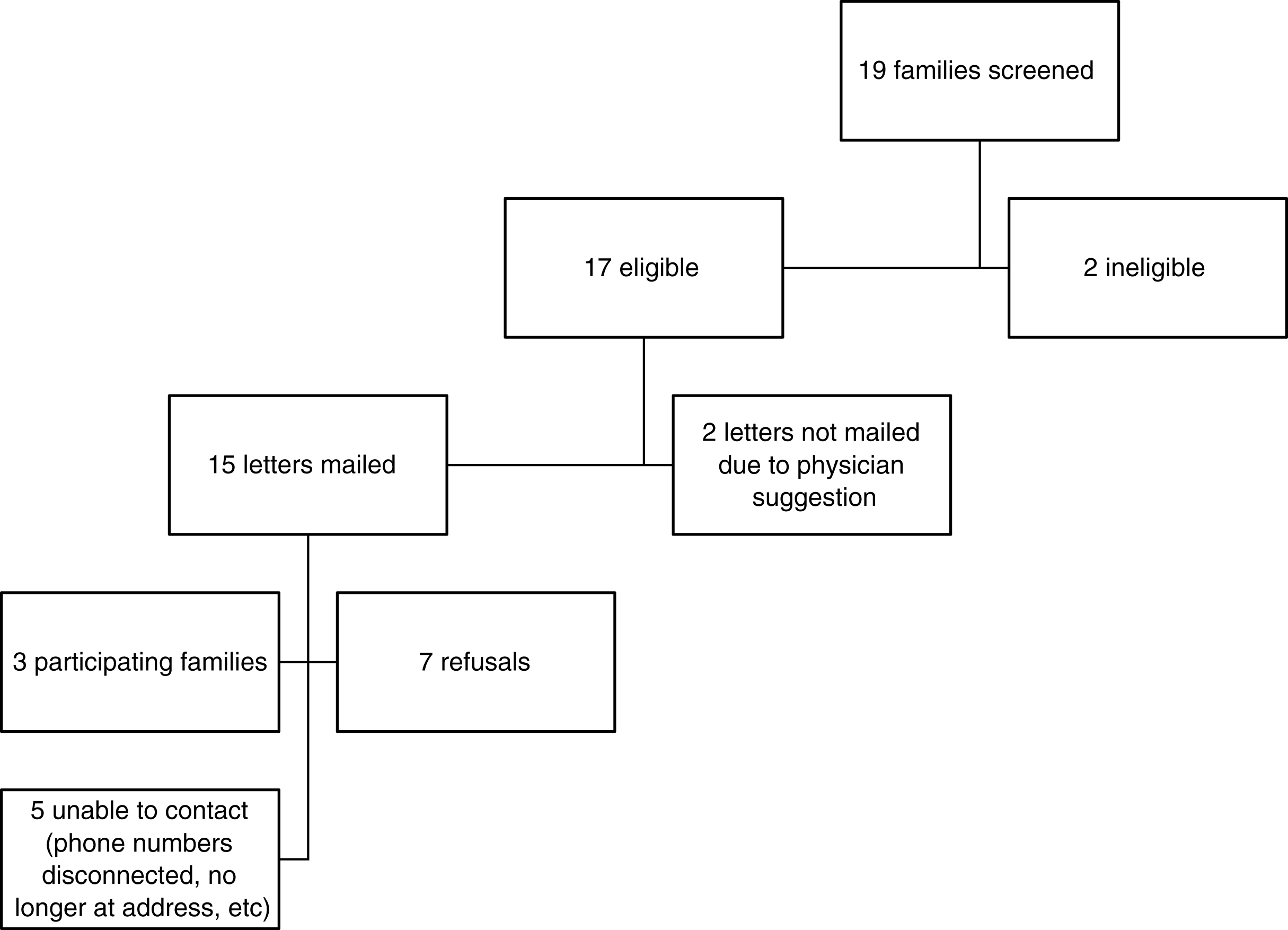
Recruitment process.
Trained and guided by the PI, three graduate research assistants (RAs) analyzed data from the open-ended questions through qualitative content analysis, the coding method used by the PI in previous research [e.g., 15,16,18,19]. The researchers manually coded the data rather than using coding software because of the small amount of data. The RAs repeatedly read the transcripts to gain a holistic sense of the data. They made notes in the margins and underlined key thoughts as they read. Next, similar ideas were clustered from the first five pages (double-spaced document) of transcript, and preliminary categories emerged. The researchers reviewed the initial coding scheme, extracted quotes, and regularly discussed the rationale for emerging categories during regular meetings (e.g., every other week) led by the PI. Data were re-examined by recoding original transcripts and making mutually agreed upon category changes. Fifteen new pages of transcript were added to the coding scheme, and new codes were adopted when data did not fit into an existing category. The RAs repeated this process until they reached consensus and no new categories emerged (data saturation).
Results
Four major themes emerged regarding participants’ perceptions of a legacy intervention: (a) parents’ willingness to participate in a legacy intervention, (b) parents’ suggestions for a feasible intervention, (c) parents’ suggestions for an acceptable intervention, and (d) parents’ perceived benefits of legacy-making. Descriptions and exemplar quotes will be presented for each theme.
Parents’ willingness to participate in a legacy intervention
All six parents said they would have been willing to participate in a legacy intervention and perceived that future bereaved parents would want to participate. Sub-categories emerged within this theme including parents’ desire to share stories about their deceased infants, unpreparedness to create legacies on their own, and desire for help to create legacies of their infants.
Parents’ desire to share stories about their deceased infants
The parents were quick and eager to talk about and share storied about their deceased infants, which although not probed, occurred during the focus group discussion. One parent told a story of when and where her water broke. Another spoke about the cross that her sister gave to her daughter after she was born. Sharing stories was a way that families seemed to connect with and support each other. For example, one parent said, “ … I just remember seeing her story [referring to another participant] … and I just remember praying for her and for you guys before I even met them. And it’s just amazing how God puts people in your path in your life.” During the focus group, parents’ stories focused on their infants’ lives and included sharing photographs on their mobile devices with other participants.
Parents’ unpreparedness to create legacies on their own
Parents reported that the nature of the experience leading to the NICU left them mentally and practically unprepared to create legacies of their infants on their own. This was often due to the unexpected or unpredictable nature of the NICU. One parent said, “Especially in the NICU that [legacy intervention services] would be good, because you don’t know the outcome when you’re in the NICU. Some children will pass away and those people, you could make that story for them like this. I don’t know about you guys, but when we got here we didn’t know the outcome would be that [death], and so that would have been great to have.” Parents discussed physically not having items necessary to document memories and time with their child. One parent said, “In our position, it was a very stressful time. Like my sister is the one who got all the videos and pictures. Like we didn’t even have our cameras and stuff because we didn’t even know that we were going to be having our daughter that day.” Parents also reported on being mentally unprepared: “I didn’t think about taking videos. I just wasn’t in my … neither one of us … I wish I would have....”
Parents’ desire for help to create legacies of their infants
Participants reported that without the help of their family and the hospital staff, they may not have any videos or pictures of their children. One participant said, “I mean, if it wasn’t for my sister, we would not have had the videos and pictures, and I cherish those.” Another parent said, “We have lots of pictures, and like I said, we’ve got albums and pictures hanging up at the house, and they are all taken by the NICU nurse. There was nobody else back there with us.” Another parent similarly said, “It was just so nice that somebody, you know, cared to do that, you know?” Parents also noted that nurses especially helped them in other ways to facilitate legacy-making, such as providing “little gowns,” facilitating finger/ hand/foot prints and molds, staying after their shift, and praying with family. One parent said, “Her [bereaved infant] nurse actually stayed two hours over her shift to help take care of our daughter. That’s awesome.” Another parent added, “It was awesome. It was crazy how much they cared, you know.”
Parents’ suggestions for an acceptable intervention
Parents made suggestions for how to develop a future legacy intervention via digital storytelling that would be acceptable to parents with an infant in the NICU. Sub-categories that emerged within this theme included (a) maintaining focus on the infant and (b) sensitivity to the presentation of legacy-making services.
Focus on the infant
In discussing logistics of offering a legacy intervention for parents in the NICU, participants’ main suggestion was to develop an intervention and offer it in a way that would allow parents’ focus to remain on their infant. One parent said, “I didn’t think about taking videos … Your focus is on that child … You’re just not thinking. It felt like a dream.” Another added, “I knew there were people in there, but they were like blurred. Yeah, I know. Like the only thing I was focused on was her … I didn’t think about anything else. So I don’t think I even would have really noticed them [legacy intervention staff, e.g., videographer, photographer] to be honest.” Another parent said, “As long as they’re [study staff] not bothering me and I’m getting my time, I don’t care. I mean, I just wouldn’t want anyone imposing on me.”
Sensitivity to the presentation of legacy-making services
Parents discussed the need for sensitivity to legacy interventions that could potentially imply that death is imminent. Participants suggested that researchers be thoughtful in how the study is presented to avoid the perception that only children who are going to die will be included. One specific recommendation was to provide the intervention as “a standard service that doesn’t imply any outcome [by saying], you can have this if your baby is healthy, you can have this if your baby doesn’t … we’ll give it to you either way and it’s a service that everyone gets in the NICU.” Participants also suggested that digital stories could help future families that might undergo similar situations, regardless if baby ultimately died or survived. Thus, participants suggested offering digital stories to as many families in the NICU as possible, including those with infants not expected to die. A parent said, “If the hospital filmed some hope stories, it would help out for other people, because not everyone will have a baby pass away.”
Parents’ suggestions for a feasible intervention
Finally, parents offered suggestions for how a legacy intervention could be developed as feasible for NICU families. Sub-categories that emerged within this theme included (a) when (b) where, and (c) how to offer a legacy intervention.
When to offer a legacy intervention
Parents discussed timing for when to offer a legacy intervention in the NICU. Participants agreed that although difficult to ask legacy-related questions during their time in the NICU, they perceived that bereaved NICU parents would want to include photographs and videos of the infant, while still alive when possible, and that such activities would have to be offered during the NICU stay. Parents suggested that sooner versus later would be better for parents who may be able to anticipate a NICU stay. For example, parents reported that mothers notified of an infant’s potentially life-threatening condition during pregnancy may want to hear about legacy-making services during pregnancy, prior to potential time in the NICU.
Parents also reported on the individual nature of grief and how that may impact timing of when parents could participate in a legacy intervention. One parent described grief as a “chapter in a book.” Another parent said, “It’s been ten months [since the death], and I mean we can talk about it now, but I mean like it depends on who I talk to if it upsets me. Like I can talk to my family all day long, and at first I couldn’t talk to my family about it. Now I can talk to my family about it, but I can’t talk to strangers about it without crying. So like it’s just a different process.”
Where to offer a legacy intervention
Parents discussed the location of where to offer legacy-making services if any follow-up occurred post-discharge. One parent preferred not going back to the NICU: “They rolled me into the NICU twice. And that was just really … that was very traumatic for us. Like I had - that [death of infant] had just happened and then it was just, it was very traumatizing. It’s like going by the scene of a car wreck you were in just twenty-four hours after you were in it.” Another parent added “I feel the same way. I love the hospital, but I hate coming up here. I’ve had a lot of loss up here.”
How to offer a legacy intervention
Parents suggested to share with future study participants that the study was developed based on reports from other bereaved NICU parents: “I think it would help if you told the parents, too, that you’ve talked to people who have been through this.” Parents also recognized that while they wished legacy services could be offered to all families in the NICU, that inclusion criteria would have to be developed to create a feasible study due to the time and effort required by videotaping. One parent said, “This could be a lot of work the more I’m thinking about this. I mean, I’m thinking through and a lot of video work. Right. And a lot of video editing and … Is the hospital prepared to take on that much work? That’s a big effort … ‘Cause you’re going to have four or five people trying to videotape and four or five people you know, in the NICU with cameras and things and there’s twenty … Are there twenty of thirty people up there in the NICU at one time?” Another parent perceived “ … It’s a big project. Yeah. And not a lot of space.” The parents felt that stories could not feasibly be offered to everyone: “Because you’ve got so many babies in the NICU, and how could you do everybody’s story and everybody’s … you know what I mean?” One parent suggested that such a project could benefit from including students. One parent wondered if “ … [name of University] has a school of video and film” and if perhaps there would be “graduate type students” whose “project” would be to take and create video.
Perceived benefits of legacy-making
Parents reported that a legacy intervention via digital storytelling would result in beneficial visual representations and reminders of their baby. One parent expressed, “You’re able to keep your memories. You can go back and look at it.” Parents noted how the legacy intervention could enhance comforting continuing bonds with their deceased infants. A parent said, “I think just having [a video] helps. It helps comfort you … Just kind of like, you know … I feel close. It’s weird, but I feel close to her through that.” Another parent similarly stated, “It helps me to hold I mean, that connection is … is still there.” Parents also discussed the benefit of having a tangible digital story of their baby: “You just have videos and memories, because you don’t have anything else.”
Parents suggested that a digital story would not only benefit parents but also other family members. Participants liked the sharable nature of having a digital story. One parent suggested a digital story could “ … help your family … I mean, family that wasn’t able to be here … So they can still have a connection to that child.” Another participant said, “I think it helps with the grieving process. And, to show their siblings. … We have a six-year-old and four-year-old. So you know, they never got to meet her or see her so … That [a digital story] would have helped out further down the road when they would have understood what was going on.” Parents reported that the continuing legacy that a digital story could help facilitate could help alleviate bereaved parents’ fears of the deceased child being forgotten.
Discussion
This qualitative study is the first to explore bereaved parents’ perspectives of legacy-making intervention in the neonatal intensive care unit. Through our qualitative analysis, we effectively explored the feasibility and acceptability of a legacy-making intervention for parents of infants in the NICU. All participants agreed that a legacy-making intervention via digital storytelling would be feasible, acceptable, and beneficial for NICU parents. Participant reports supported the need and desire for legacy-making services to be offered in the NICU.
Parents suggested that one potential outcome of legacy-making included continuing bonds with their deceased infants. The continuing bonds theory suggests that maintaining connections with the deceased can help facilitate coping and provide comfort to bereaved individuals [21]. Continuing bonds has been shown to be expressed in various ways, such as keeping physical representations (e.g., photographs, videos) of the deceased and thinking about the deceased, and can result in comforting and discomforting effects [22]. While legacy-making has been studied in pediatric and adult patients with advanced illnesses and their family members [14–19], the impact of legacy-making in bereaved parents of infants who died in the NICU remains unexplored. Continuing bonds is an important outcome to consider for legacy-making in bereaved populations.
Participants reported that the inclusion of pictures and videos of their child would be desired because it allows for a keepsake that can facilitate continued bonding with their child after death. A recent study found that “being a parent” and “being there for my child” is very important for NICU parents, even if their child’s life is very brief [23]. The current study not only supports this finding but extends it beyond the immediate bereavement period, suggesting that continued attention and feelings of closeness with the deceased child are important in maintain the feeling of being a parent, which may help with feelings of grief.
Participant reports also suggested that digital storytelling could enhance coping strategies for family members of deceased infants. Similarly, studies have shown that storytelling is an effective intervention to promote coping in surrogate decision makers for patients who have died in the intensive care unit [24, 25]. Narrative theory suggests that storytelling and other narrative-based interventions reduce distress from traumatic events and through emotional disclosure, cognitive processing, and social connection [26]. Future work is needed to further examine how legacy-making via storytelling could impact coping for bereaved parents and family members following the death of an infant.
In addition to some of the benefits digital storytelling could have for bereaved parents in the NICU, participants identified some potential barriers to its implementation, including timing of approaching parents in the NICU, sensitivity to the potential uncertainty of prognosis for infants in the NICU, and logistics of collecting photos and videos. Participants suggested making inclusion criteria as inclusive as possible, approaching parents as early as possible, and presenting the intervention to parents as a positive and productive activity that has been shown to help previous NICU parents in similar situations. Participants identified nurses as being in ideal roles to help facilitate the intervention process (e.g., taking photographs, etc.).
Participants stressed that an acceptable intervention would need to allow parents to remain focused on their child. Similarly, Hinds et al., [27] found that parents of children with cancer have defined being a good parent as including being at their child’s side and showing the child that he or she is cherished. Regardless if the intervention format developed and offered to parents is web-based or face-to-face, the important element for a feasible and acceptable intervention is that it must allow parents to remain in their “good parent” role. Pilot studies are now needed to develop and test feasibility of digital storytelling methods that may be best suited for bereaved NICU populations.
It is interesting to note that parents reported they would be willing to share their infants’ digital stories with others, including other parents and families in the NICU. Parents seemed willing to participate not only for their own benefit but also for others. This altruistic nature of bereaved parents is similar to the altruism previously described as a form of coping in clinical trial participation [28], perhaps by promoting meaning-making related to traumatic events [29, 30]. Moreover, digital storytelling could offer a way for parents to share their infant’s story with other family members who may not be allowed in the NICU or have opportunity to come to the NICU, such as siblings, grandparents, or friends and loved ones that live far away.
We acknowledge that the sample size is extremely modest, and thus, generalizability of results are quite limited. Generalizability of results are limited to parents who experienced the death of an infant who was treated or died in the NICU. Thus, the idea of a legacy intervention may not be feasible or acceptable to bereaved individuals who have experienced other types of loss. Despite these limitations, this study demonstrated feasibility and acceptability of legacy-making for bereaved parents who experienced the death of an infant.
Implications for practice include the potential for legacy-making in the NICU to improve relationships and communication between parents and the medical team. Nurses and physicians are often involved in the making of memorabilia hand and footprints for parents to take home [18]. A digital legacy-making tool that is created over the course of a baby’s hospital stay has the ability to improve parent-nurse and parent-physician dynamics and overall improve parent communication and satisfaction. Future studies should include the design of a conceptual framework that would include the relational impact of the parent, additional family members, and medical team through this novel legacy-making intervention. Primary outcomes for future studies could include parent coping, continuing bonds, satisfaction, anxiety, decisional conflict, and additional markers of quality. Research is now needed to develop a NICU-specific legacy intervention and examine preliminary efficacy of parent outcomes.
In summary, legacy-making is a unique tool that could benefit parents of infants in the NICU. Narratives are key to looking beyond the superficial facts or clinical context and critical to opening a ‘space’ to discuss deeper values and moral concerns [31]. Legacy-making interventions, including narratives, may allow opportunities to explore moral dynamics (the individual and collective processes by which moral behavior and moral attitudes emerge, evolve, spread, and disappear) in the context of the NICU, and potentially improve communication, decision-making, and family-centered care and healing.
Funding
The authors have no funding support or conflicts of interest to disclose.
Footnotes
Acknowledgments
The authors would like to thank the generous families who contributed to this project.