
Abstract
BACKGROUND:
Necrotizing Enterocolitis (NEC) is a multifactorial condition where PRBC transfusion is associated with necrotizing enterocolitis (TANEC) in about a third of all cases of NEC. We have investigated the role of feeding practices in incidence of TANEC. We sought to compare infants diagnosed with TANEC versus infants diagnosed with classic NEC and investigated the effects of a standardized slow enteral feeding (SSEF) protocol on TANEC incidence as well as the effects of SSEF on growth of infants with NEC.
METHODS:
We conducted a retrospective cohort study, where medical records of infants born in a tertiary care neonatal intensive care unit (level IIIb) from January 1997 to May 2014 with birth weight < 1500 grams and gestational age≤34 weeks with NEC stage IIa or greater according to the modified Bell’s staging were reviewed.
RESULTS:
During the study period, 111 infants developed NEC, and 41/111 (37%) were diagnosed with TANEC. Infants with TANEC were smaller, more premature, had higher SNAPPE scores and were more anemic prior to transfusion compared with infants with ‘classic NEC’. The severity of NEC did not differ between the two groups, however, infants with TANEC had worse outcomes and longer NICU stays. Introduction of SSEF protocol, led to a significant decrease in TANEC. There was no difference in weight and head circumference of infants in the two groups at 2 years corrected age.
CONCLUSION:
SSEF led to a significant reduction in the incidence of TANEC without impairing growth at 2 years corrected age.
Abbreviations
appropriate for gestational age;
Necrotizing enterocolitis;
patent ductus arteriosus;
pregnancy induced hypertension;
packed red blood cells;
prolonged rupture of membranes;
periventricular leukomalacia;
retinopathy of prematurity;
transfusion associated necrotizing enterocolitis;
transfusion-related acute gut injury;
transfusion associated lung injury;
score for neonatal acute physiology perinatal extension;
slow standardized enteral feeding
Introduction
Necrotizing enterocolitis (NEC) is an acute, devastating illness commonly seen in 5–10% of the preterm neonates, where transmural necrosis of gastrointestinal tract leads to feed intolerance, abdominal distension, bloody stools, perforation, and peritonitis in some cases with increased long-term morbidity and mortality [1]. NEC leads to need for surgical intervention in many cases and is responsible for increased length of stay, cost of care and later developmental delays in survivors. Transfusion associated NEC (TANEC) has been recognized as a distinct entity over the past two decades and the reported incidence of TANEC ranges from 5–17 per 1000 transfusion events, accounting for almost a third of all NEC cases [2–5]. TANEC has also been described as transfusion-related acute gut injury (TRAGI) and is analogous to PRBC transfusion associated lung injury (TRALI) [6]. TANEC has been hypothesized to be related to degree of anemia in these infants [6–8], feeding practices like duration of withholding feeds before transfusion [9–11] and activation of T-cryptantigen in stored red blood cells due to growth of micro-organisms, which produce neuraminidase like enzymes [12, 13]. However, to date no cause and effect relationship has been established between any of these risk factors and TANEC.
The incidence of NEC at our institution over the past 2 decades prior to the year 2009 had mirrored the rate of this disease in the country. Since NEC is such a severe and devastating disease, we adopted changes in our feeding practices and as a result, were able to achieve a significant decrease in our NEC rate. Our slow standardized feeding regimen and that of others have been associated with a decrease in incidence of NEC [2, 14–16]. However, so far it is unclear how these feeding practices affects TANEC rates. We hypothesized that along with NEC, TANEC rates are also decreased significantly with adoption of a very slow enteral feeding protocol. Our study aims to describe the effects of SSEF on TANEC rates in comparison to classic NEC and study whether adoption of SSEF leads to impaired postnatal somatic growth.
Methods
After approval by the institutional review board of the MetroHealth Medical Center, we conducted a retrospective chart review of all infants with birth weight less than 2500 grams and less than or equal to 34 weeks gestational age, born between January 1997 and May 2014, who were diagnosed with NEC. Our inclusion criteria were: stage IIa or greater NEC according to the modified Bell’s staging. We excluded all infants with known congenital malformations of the GI tract, chromosomal anomalies, major congenital heart disease or infants with hypoxic ischemic encephalopathy. We further analyzed data on infants who developed NEC and had birth weight≤1500 g.
Demographic and prenatal data was extracted from the medical records of all selected infants and their mothers. Infants were classified as TANEC if PRBC transfusion was given 48 hours prior to developing signs and symptoms of NEC. Demographic data including birth weight, gestational age, race, gender and mode of delivery were recorded. Maternal characteristics recorded were blood type, the presence of pregnancy induced hypertension (PIH), chorioamnionitis, prolonged rupture of membranes (PROM) and use of antenatal steroids. Infant characteristics recorded were pre-transfusion hematocrit (first transfusion), age in days at onset of NEC, relationship of NEC onset to a transfusion in the preceding 48 hours, and severity of NEC. Additional infant data elements recorded were Apgar scores at 1 and 5 minutes, SNAPPE scores on admission, the presence of a hemodynamically significant patent ductus arteriosus (PDA), type of feeds (breast milk, formula or mixed breast milk and formula feedings) and enteral feeding status during the time of transfusion. Data on outcome variables included diagnosis of bronchopulmonary dysplasia (BPD), intraventricular hemorrhage (IVH), periventricular leukomalacia (PVL), retinopathy of prematurity (ROP), length of stay, death, weight at discharge and weight and head circumference at 1 and 2 years of corrected age.
During the pre-study period (Epoch 1, 1997 to 2008) infants were started on enteral feeds within the first three days of life with no predefined NPO period and feeds were advanced at the rate of 10–15 ml/kg/day till full feeds were achieved by 14 to 18 days of life. A new SSEF protocol was introduced in our NICU in July 2009 and adopted for care of all VLBW infants in Epoch 2 (after July 2009), details of which are as published (16). This protocol mandated an NPO period of 14 days for infant’s≤750 g birth weight, 7 days for infants between 750–1000 g birth weight and lesser duration for older infants. This was followed by a period of trophic feeds for 7 days in each group where infants received human milk only feedings at 10 mls/Kg. The SSEF protocol differed from previous feeding guidelines by delaying the start of enteral feeding, providing more days of priming and then increasing very cautiously. In addition, human milk fortifier (HMF) was introduced during the SSEF protocol when the enteral feed reached around100 mL/kg/d compared with 150 mL/kg/d during the earlier epoch. In some cases, at the attending physician’s discretion, the initiation of feeds was allowed to be further delayed, if clinically indicated, but no infant was fed sooner than the stated guidelines. Thus, full feeds (150 ml/kg/day) were achieved by day 44 to 52 of life in second epoch compared to 14–18 days earlier in the first epoch.
The guidelines for PRBC transfusion in our NICU did not change significantly during the entire study period. We use prophylactic recombinant human erythropoietin to prevent severe anemia of prematurity from day of life 7–14 for 4–6 week period at standard dose of 250–400 units/kg three times each week. We supplement IV or enteral iron during Erythropoietin use at standard dosing. During the study period, no guidelines existed for withholding feeds during PRBC transfusions and the decision to hold feeds was determined by the treating neonatologist.
To assess the impact of SSEF on growth of infants with NEC, we compared the weights and head circumferences of all survivors of NEC born from January 2000 – May 2014 at discharge and at 1 year and 2 years corrected age. This cohort was chosen because follow up records for babies born prior to January 2000 were incomplete.
Data is expressed as mean±standard deviation, and as percentages. Chi square tests and Fisher exact tests were used for categorical data and T-tests was used for continuous variables with Bonferroni correction applied to multiple comparisons. A p value < 0.05 was considered statistically significant.
Results
During the study period (January 1st 1997 till May 30th 2014), 111 infants with NEC with birth weight≤1500 g met our inclusion criteria and their demographic characteristics and NEC risk factors are as shown. Of these infants, 41 (37%) had received PRBC transfusion 48 h before the onset of clinical signs and symptoms and later acquired the diagnosis of stage IIa NEC, and 70 infants did not receive PRBC transfusion. A flow chart of the study population is illustrated in Fig. 1 and the infants’ demographics and risk factors for NEC are shown in Table 1. Infants with TANEC were smaller, more premature with lower Apgar scores at 1 and 5 minutes of life, had higher SNAPPE scores at birth and were more likely to be born by Caesarian section. PDA was more common in infants with TANEC compared with infants diagnosed with classic NEC. Infants with TANEC had lower hematocrits prior to receiving transfusion compared with hematocrits of infants with classic NEC at the time of diagnosis. Maternal characteristics like mother’s blood type, pregnancy induced hypertension, prolonged rupture of membranes, chorioamnionitis and use of antenatal steroids did not differ between the two groups (p = NS).

Flow chart of study population.
Infants demographics and risk factors for NEC
Data are expressed as mean±standard deviation unless otherwise specified. Hct: hematocrit; NEC: necrotizing Enterocolitis; SNAPPE: score for neonatal acute physiology, perinatal extension; TANEC: transfusion associated necrotizing enterocolitis.
Use of mother’s breast milk was similar between the two groups (p = NS) (Table 2), though more infants with classic NEC received either formula or mixed (breast milk+formula) feeds (p = 0.03). The practice of withholding feeds around the time of transfusion was not protective against TANEC, where in our cohort of patients more infants were kept NPO in the TANEC group (p = 0.01). There were no differences between the two groups in terms of severity of NEC, but infants in the TANEC group had worse outcomes. They had more ROP (38% versus 77% p < 0.001), more PVL (6% versus 24% p < 0.001), and longer lengths of stay (77±53 days versus 105±67 days; p = 0.01). Infants with TANEC had higher mortality, however this did not reach statistical significance (20% versus 29% ; p = 0.28) (Table 2).
Feeding Characteristics, severity and outcomes of NEC
BM: breast milk; NEC: necrotizing enterocolitis; TANEC: transfusion associated necrotizing enterocolitis; NPO: Nil-per-mouth; ROP: retinopathy of prematurity; PVL: periventricular leukomalacia.
Figure 2 depicts the incidence of NEC and TANEC each year from 1997 to 2014. The incidence of NEC remained steady between 0.7% to 2.5% in epoch 1 of the study before the introduction of SSEF. With introduction of SSEF protocol in 2009 the incidence of NEC decreased to 0.3% to 0.75% and there was only one case of TANEC recorded during the 6-year Epoch 2 observation period. Table 3 outlines the demographic and outcome differences in infants with NEC before and after introduction of SSEF protocol. There were no differences in gestational age, birth weight, and number of small for gestation infants, PDA, hematocrit at birth and pre-transfusion hematocrit between the two groups and similar number of infants were receiving breast milk feeds. Besides the decrease in TANEC cases after introduction of SSEF, the onset of NEC in SSEF group was delayed till mean of 52 days (p = 0.003). The length of stay was slightly prolonged but it did not reach statistical significance. The number of days infants required a central line were significantly higher (15.5±3.64 versus 31.4±6.9; p = 0.0004) in the SSEF group, but this was not associated with an increase in central line associated blood stream infection (CLBSI) (p = 0.28) and there was decrease in incidence of late onset sepsis in the SSEF group (p < 0.001). Likewise, the incidence of TPN induced cholestasis defined as direct bilirubin > 2 mg/dL was similar between the two groups (p = 0.91).
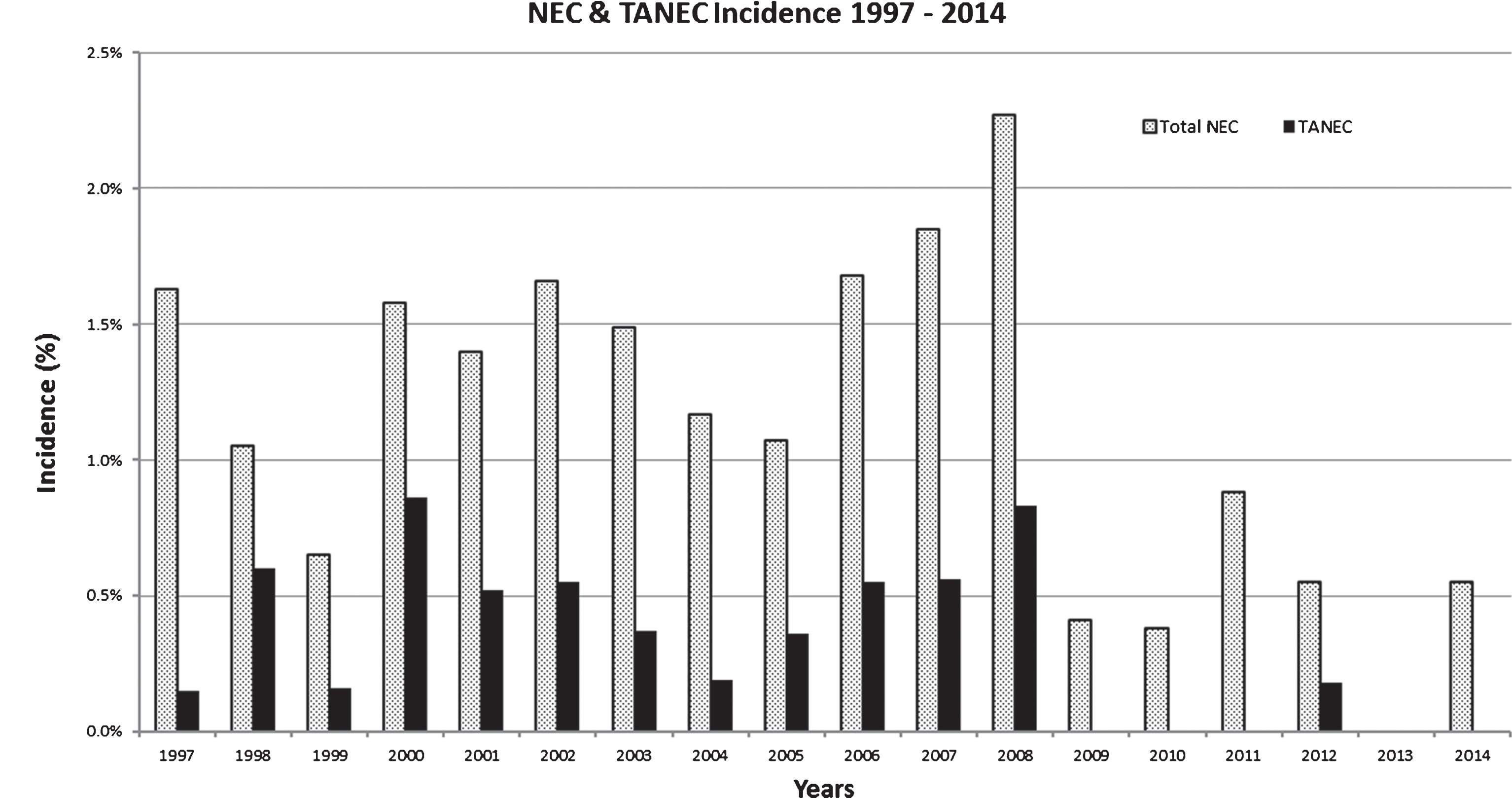
Incidence of necrotizing enterocolitis and transfusion associated necrotizing enterocolitis 1997 to 2014 in infants≤34 weeks and≤1500 g birth weight.
A comparison of NEC cases prior to and after introduction of SSEF
Data are expressed as mean±SD; NEC: necrotizing enterocolitis; TANEC: transfusion associated necrotizing enterocolitis; CLBSI: central line associated blood stream infection. aData includes survivors only, bn = 73, cn = 9; dData for years 2002 to 2008 in Prior to SSEF group and 2009–2014 in Post SSEF group; eCases/year.
A comparison of survivors of NEC before and after introduction of SSEF showed no significant difference in weight at discharge (Table 4) and both groups grew around the 40th percentile. Likewise, weights and Z scores at 1 and 2 years corrected age, respectively, were similar (p = NS). Head circumference at 1 year corrected age was also not significantly different; however, a p-value for head circumference at 2 years corrected age could not be computed due to insufficient data.
Anthropometric measurements of surviving infants with necrotizing enterocolitis (NEC) before and after introduction of standardized slow enteral feeding (SSEF) at one and two years corrected age
Data are expressed as mean±standard deviation unless otherwise specified. NEC: Necrotizing enterocolitis; CA: Corrected age; HC: Head circumference. Number of infants studied: an = 38, bn = 32, cn = 7, dn = 37, en = 27, fn = 2.
Our results show a significant decrease in NEC and almost complete prevention of TANEC after the introduction of a SSEF protocol in our institution, suggesting that NEC and TANEC are both related to feeding practices. The premature GI tract, when fed early and aggressively with calorie dense nutrition, may be at increased risk of NEC as well as TANEC. This is plausible for several reasons: the preterm GI tract has poor expression of tight-junction proteins which help to maintain epithelial barrier [17–19], gut motility is poor leading to stasis, [20] and bacterial overgrowth on top of poor host defenses allow colonization by pathogenic microorganisms [21]. The digestive capacity of the preterm gut is also limited as shown by poor expression and secretion of several enzymes, and gut hormones which help degrade nutrients in the milk [22, 23]. Standardized feeding regimens have been shown to reduce the incidence of NEC [24, 25] and slow start and slow advancement of feeding have been shown to reduce NEC, which led us to adopt our current feeding protocol [26]. Our data has clearly demonstrated that standardized feeding reduces not only the incidence of NEC, but also TANEC. Since TANEC accounts for nearly a third of cases of NEC, the cause-and-effect relationship between NEC and PRBC transfusions have been debated by over 2 decades with no clear insight so far. Our data on TANEC in Epoch 1 before introduction of SSEF in comparison to Epoch 2 make us conclude that “early aggressive feeding of the preterm gut” in association with other prematurity related factors may be at the heart of this perplexing problem.
Extremely premature infants are at risk for severe anemia and are highly likely to receive blood transfusions in the first few weeks of life [7, 27]. Similar to other investigations, our study has shown that TANEC infants had lower mean pre-transfusion hematocrits compared to infants with ‘classic NEC’ [27, 28]. Severe anemia with early enteral feeding may lead to relative tissue hypoxia of the gut, which has been postulated to predispose these infants to develop NEC [8, 29]. Thus, low hematocrit before transfusion in infants who are fed aggressively are more likely to develop gut ischemia and NEC, resulting in higher incidence of TANEC. Likewise, PDA requiring intervention (medical/surgical) was more common in infants with TANEC in our study where there is preferential shunting of blood from mesenteric circulation to the lungs leading to relative gut hypoxia. Our infants with TANEC had higher SNAPPE scores and worse APGAR scores then non TANEC controls, likely related to their lower gestational age and birth weights.
We found no difference in the amount of breast milk feedings between the TANEC and non TANEC infants, but our non TANEC infants were more likely to be exclusively formula fed or to receive a combination of breast milk and formula. NPO status during any blood transfusion did not prevent TANEC. Holding feeds around the time of transfusion is also not supported by most other investigators [28–30]. In contrast, El-Dib et al., have reported a decrease in NEC after holding feeds prior to blood transfusions [11] and Lawrence et al found no benefit to holding feeds during blood transfusions, although more infants with TANEC had achieved full feeds at the time of transfusion [30]. Christensen et al reported a larger volume of enteral intake twenty four hours prior to and during blood transfusions in TANEC cases [10]. Krimmel et al., reported that infants fed immediately after a blood transfusion failed to demonstrate the expected increase in blood flow velocity in the gut [9]. We postulate that the preterm gut that has not been fed large volumes of enteral feeds by the time of PRBC transfusion is less likely to become hypoxic and less likely to be colonized with pathogenic bacteria since the gut is not challenged to digest foodstuff which it is not capable of handling. Thus, keeping infants NPO before and after PRBC transfusion may have an additive effect to slow feeding where the volume of feed is much lower. Perhaps the delay in onset of NEC from a median of 21 days to 52 days (p = 0.003) is also reflective of this same phenomenon. Delayed initiation and slow advancement of feeds likely delays the onset of NEC beyond the critical periods of the extremely premature baby’s life allowing for growth and maturity of the gut and protecting against NEC.
Our NEC study population as reported is slightly different from most other studies since we have also studied incidence of NEC in infants≤34 weeks and≤2500 g whereas others usually report data on infants≤1500 g birth weight. We studied 38 infants with TANEC who had birth weight between 1500 g to 2500 g and in this birth weight range there were only 3 infants who developed TANEC, of which 2 were from epoch 1 and one from epoch2. Thus, we excluded these 38 infants in our final data analysis to remain in line with other published studies. We have also excluded infants who were > 2500 g in birth weight and > 34 weeks gestational age, since in these infants NEC is rarely seen and when it does occur, is related to congenital malformations or hypoxic-ischemic encephalopathy. The incidence of NEC in our VLBW infants was between 4–8.8% in epoch 1, which is in line with the national average. After introduction of SSEF our NEC rate dropped to 1.2–3.2% .
There was no difference in the median age of onset of NEC in Epoch 1 between TANEC and non TANEC groups (median of 16 days versus 19 days, p = 0.6)17 and our findings are similar to other reports where no difference was noted [28, 30]. Lawrence et al reported a higher percentage of surgical NEC in infants with TANEC; however, in our study, the severity of NEC was similar in the two groups [30]. Compared to infants with classic NEC our infants with TANEC had worse ROP, larger percentage of infants had PVL and longer lengths of hospital stay. These findings are most likely related to the lower gestational age and birth weight of infants with TANEC in our study.
We observed a decrease in total incidence of TANEC after introducing the SSEF, a drop from 41% to 8% (p = 0.03). Some other investigators have reported a similar trend. Berseth et al reported increased risk of NEC in very low birth weight infants (VLBW) with early advancing feeding volumes [31]. Early enteral nutrition has been proposed to avoid gut atrophy and promote gastrointestinal maturation [32, 33], and Leaf et al in a randomized trial of small for gestational age infants (mean gestational age of 31 weeks) showed that early enteral feeds on day 2 versus delaying enteral feeds up to 6 days did not increase the risk of NEC (15% in late feeders versus 18% in early feeders) [34]. Infants in our study were more premature (mean gestational age of 27 weeks) and the majority were the appropriate size for gestational age (AGA). Also, advancement of feeds according to the SSEF protocol in our institution is very slow, with infants achieving full enteral feeds in approximately 44 – 52 days compared to a median of 21 days for infants with delayed enteral feeds in Leaf’s study. The risk of extra-uterine growth restriction and poor neurodevelopmental outcomes have been described with a slow enteral feeding regimen [35, 36]. La pointe et al advocate for early optimization of nutrition. Their study reported a lower incidence of post-natal growth restriction and unchanged incidence of NEC in infants < 1300 grams (10% versus 12%) with more aggressive nutritional optimization (36). We found no difference in weight at discharge and head circumference and weight at 1 year corrected age and weight at 2 years corrected age. There was a trend of lower weight gain in the first 4–6 weeks of life while our study infants were in the NICU, but these infants were able to catch up with their peers by the age of 1 year.
The limitation of our study is its retrospective design, conducted in a single center and a small sample size. We feel the protective effect of slow feeding should be studied in a much larger, multi-center, randomized controlled trial to be able to confidently generalize our findings to the general population. Availability of data on neurodevelopmental outcomes of infants on SSEF will further help clinicians decide whether delaying initiation and slow advancement of enteral feeds is an acceptable tool to prevent TANEC. However, our study adds to the growing body of evidence that questions TANEC as a separate disease entity and points towards the multifactorial nature of NEC with perhaps greater emphasis on enteral feeding practices. We have conclusively shown that SSEF can significantly reduce the incidence of TANEC without impairing growth, thus adoption of our protocol is a simple and easy approach to primary prevention of NEC as well as TANEC.
Contributors’ Statement
All authors do not have potential or actual conflict of interest to report. Drs. Shekhawat, Pandey and Sharon Groh-Wargo conceptualized and designed the study, analyzed data, reviewed and revised the manuscript and approved the final manuscript as submitted. Dr. Dako designed the data collection instruments, collected the data, carried out the initial analyses, drafted the initial manuscript, and approved the final manuscript as submitted. Joshua Buzzard and Dr Jain collected the data, did initial data analysis, reviewed and revised the manuscript and approved the final manuscript as submitted.