
Abstract
BACKGROUND:
The present study aimed to determine the effect of perceived stress during pregnancy on neonatal outcomes and cortisol and leptin levels in mothers and their newborns.
METHODS:
This longitudinal study was carried out on 110 pregnant women in Miandoab city, Iran. Mothers, who had singleton pregnancies and gestational age of 24 to 28 weeks, were included in the study. The participants were asked to fill out Cohen’s Perceived Stress Scale (PSS). The mothers were then tracked in gestational ages of 28–32 weeks, 32–36 weeks, and the time of delivery. The maternal and umbilical cord blood samples were obtained during labor in order to measure leptin and cortisol levels.
RESULTS:
Umbilical cortisol level was significantly higher in newborns who had meconium stained amniotic fluid than those who did not. Maternal blood leptin levels at delivery were significantly higher in the mothers whose neonates had respiratory distress, low birth weight, low head circumference, low Apgar score, and were premature than those whose neonates did not have such problems. The level of leptin in umbilical cord blood was significantly higher in neonates who had respiratory distress than those who did not. The results also showed a significant correlation between maternal cortisol levels and PSS during weeks 24–28 and the entire pregnancy. A significant relationship was observed between umbilical leptin and maternal leptin levels.
CONCLUSIONS:
It can be concluded that stress during pregnancy is accompanied by fetal distress. The probable reason for newborns distress may be related to increased maternal leptin levels.
Introduction
Stress is a condition which is experienced by everyone and includes not only major life events but also the hassles of daily life [1]. Pregnancy and childbirth are among the most sensitive periods of women’s lives, which results in major changes in their lives, including physiological and psychological changes as well as changes in social-family roles. These changes can reinforce the emotional instability and give rise to Psycho-pathological disorders such as stress and tension in mothers [2, 3]. Pregnancy is an inherently stressful period; however, poor health outcomes are generally seen in association with extreme levels of stress. Stress during pregnancy can be accompanied by undesirable pregnancy outcomes such as miscarriage, nausea and vomiting, preeclampsia, weight loss, preterm delivery, and low birth weight [4, 5]. In addition, stress can increase the dangers of unhealthy behaviors, such as smoking and excessive drinking. Such behaviors may, in turn, lead to undesirable pregnancy outcomes [6]. Since stress is not commonly measured during pregnancy and its effects on the mother and infants’ health are not estimated, the stress level during pregnancy is unknown [7]. Stress activates the hypothalamic–pituitary–adrenal (HPA) axis and increased levels of stress in long-term can affect its function and lead to increased levels of cortisol in blood [8]. Although the cortisol secretion mechanism varies in different ages and there is no precise information on the secretion of cortisol especially in infants younger than 6 months, it is known that physical stressors and painful processes result in more secretion of cortisol [9]. It is reported that prenatal stress leads to a long-lasting increase in cortisol levels and potentiates febrile seizure in children under 2 years old; thus, neurological complaints can be intensified in a child that is exposed to stress prenatally [10]. In animal studies, it is reported that stress during pregnancy increases corticosterone hormone levels before and after childbirth in comparison to the group without stress. The stress during pregnancy also keeps the corticosterone hormone levels in infants high for a long time [11]. In a study, Edwards et al., investigated the effects of stress during pregnancy on changes in hormonal and behavioral responses that are effective in the body weight regulation system, such as increased appetite and a combination of metabolic syndromes such as insulin resistance and increased serum levels of cortisol and leptin [12]. It was found that adipose tissue responds to stress by secreting leptin [13]. Glucocorticoids, and probably adrenocorticotropic hormone (ACTH), stimulates synthesis and secretion of leptin which in turn affects the activity of adrenal glands [14]. Meanwhile, both cortisol and leptin levels rise in pregnancy by up to 30 days and remain almost constant during gestation [15] except stressful conditions that lead to high levels of cortisol [14, 17].
There is not enough evidence on the effects of leptin on fetus growth. Besides, it is not clear if there is a relationship between stress during gestation and leptin blood level of mothers and/or offspring.
Today, in developing countries such as Iran, prenatal health care is limited to physical care while mothers’ mental health is ignored. Whereas, physical health depends on mental health and mothers’ mental health improves family health and the health of the child that is going to be born [18]. In general, stress during pregnancy is of utmost importance, since it can have a significant influence on mothers and babies’ health as well as babies’ later-life stages. Any kind of change in mothers’ hormones can result in some changes in the fetus through the placenta. The present study aimed to investigate the effect of perceived stress during pregnancy on neonatal outcomes and cortisol and leptin levels in mothers and their newborns. We hypothesized that a high-stress score during pregnancy is accompanied by high leptin and cortisol levels both in mothers and babies.
Method
This study was approved by the Medical Ethics Committee, Urmia University of Medical Sciences, Urmia, Iran. All the experimental protocols and procedures complied with the guidelines of 1975 Declaration of Helsinki as reflected in Guidelines of Medical Ethics Committee, Ministry of Health, IR Iran. The present study was a longitudinal study which investigated the pregnant women who had referred to the hospital and the health care centers in Miandoab city, Iran for routine prenatal care. This study started in November 2015 and lasted for 6 months, until the end of April 2016. The population under study was comprised of pregnant women within the gestational age range of 24 to 28 weeks who were pregnant for a singleton. The sampling was based on availability. The sample size, based on the study conducted by Salari et al. [19] and considering the correlation coefficient between stress and cortisol level (0.312), the confidence level of 5%, and statistical power of 80%, was calculated as 100 participants using the correlation coefficient formula. Taking a 10% drop-out rate into account, 110 pregnant women were included in the study. There were no dropouts in the study; therefore, the number of the participants remained 110 all through the study. The criteria for inclusion in the study was not having any underlying disease such as diabetes or cardiovascular, kidney, lung, and autoimmune disease during and before pregnancy, as well as not having any psychological disorders and not using any psychotropic drugs. In order to obtain the required information, the researcher went to the reference laboratory where all pregnant women of the city referred to for routine check-ups of week 24–28 of pregnancy. The reference laboratory was selected so that the samples would have the same conditions. Since this laboratory was a public one, it had lower costs and all pregnant women from all over the city (including villages) were referred to this center. After an interview and explaining the methods of conducting and goals of the research, a written consent was obtained from the pregnant women who volunteered to take part in the study. Cohen’s perceived stress questionnaire, as well as a questionnaire developed by the researcher about the demographics of the participants, were filled out by the participants. The mothers’ then were contacted three times, every four weeks. In other words, they were first contacted in the weeks 28–32 of pregnancy, the second contact was in the weeks 32–34 of pregnancy, and the third one was during delivery. The researcher contacted the participants by calling them in the first and second times. In the first and second contact Cohen’s perceived stress scale was filled out by the participants, and for the third time, they were asked to call the researcher, via the number they were provided with, in case of going to the delivery room and onset of labor. In addition, based on the first day of last menstrual period, the exact time of the delivery was estimated and the researcher was present in the delivery room at the time that was determined for the delivery of the participants, even if the participants didn’t call the researcher. Thus, the third contact was made by the presence in the delivery room. At the time of labor, the same perceived stress questionnaire, as well as a questionnaire related to neonatal outcome (weight, length, and head circumference after birth, the Apgar score, having respiratory distress, meconium stained amniotic fluid, and being full term), was filled out. In this stage mothers’ blood samples that were drawn as a routine at the time of reception was used to measure the leptin and cortisol levels of mothers’ blood. The blood samples were obtained prior to any intervention on participants in order to avoid any possible effects of those interventions on blood levels of the hormones. In order to test the leptin and cortisol levels of the neonates, cord blood samples, which are drawn at the time of birth as a routine for determining Rh, were used. Although cortisol concentrations follow a circadian rhythm and sampling time should be the same for all of the participants, due to the unpredictability of the delivery time, this was not applicable and the time of sampling depended on the time of delivery. Blood samples were centrifuged for 10 minutes at 3000 g and their serum samples were separated. Serum samples were put in closed and coded Eppendorf tubes and were kept in – 20°C until they were tested. The frozen serums were melted in the laboratory temperature and the hormone levels were measured. All of the samples were analyzed under the same conditions (time, place, and analyst). Leptin and cortisol were measured by ready-to-use ELISA kit (BioVendor, Karásek, Czech Republic) and (DiaMetra, Milan, Italy), respectively.
Instruments
Cohen’s Perceived Stress Scale (PSS): Cohen’s PSS was first prepared by Cohen et al. in 1983. This questionnaire is used to measure general perceived stress during the last month of pregnancy. This questionnaire measures the individual’s perceptions, thoughts, and feelings about stressful events, as well as controlling, overcoming, and coping with stress and mental pressure. This scale also investigates risk factors and shows the stressful relations’ processes. It is widely used in different countries for measuring perceived stress and thus is standardized and translated into many different languages. The PSS includes 14 items that investigate the participants’ feelings and thoughts and their general perceived stress during the last month. In this research, a 14-item version of the questionnaire was used. This 14-item questionnaire includes seven negative items and seven positive items indicating a good adaptation of the person with stress factors. The items are rated on a 5-point Likert scale ranging from “Almost Never” to “Almost Always”. Items number 4, 5, 6, 7, 9, 10, and 13 were reverse coded. The lowest obtained score was zero and the highest score was 56. The cutoff point of 21.8 and higher indicated higher perceived stress [20]. In studies conducted by Ghorbani et al., Cronbach’s alpha for the American and Iranian population was calculated as 0.86 and 0.81 respectively [21]. Construct validity of the questionnaire was determined as 0.63 that is significant in the alpha level of p < 0.05 [22].
Demographic questionnaire: this questionnaire was developed by the researcher and has three parts: demographic information (age, language, address, and pregnant women and their husbands’ level of education and job), information about fertility (pregnancy age, number of deliveries, type of delivery, abortion, stillbirth, problems in previous pregnancies, problems in the current pregnancy, the pregnancy being intended or unintended, neonate’s gender, desirability of the neonate’s gender, mother’s interest in pregnancy, weight before pregnancy, weight gain during pregnancy), and neonatal outcome (weight, length, head circumference, Apgar score, having respiratory distress, meconium-stained amniotic fluid, and prematurity).
Statistical analysis
The data was analyzed by SPSS software version 16. Student’s t-test, ANOVA, and K2 tests were run to analyze the data. In addition, the Pearson Correlation test was run to test whether there is a relationship between PSS and leptin and cortisol levels in the mothers and babies. The normality for continuous variables was assessed using the Kolmogorov-Smirnov test and P < 0.05 was considered significant. The results were presented as mean±SD.
Results
In the present study, the mean age of mothers was 27.48 years and their age ranged from 15 to 40 years. Of the mothers and their husband’s, 40% and 37.3% respectively had elementary education; 96.4% of the participants were housewives and 8.2% of participants’ husbands were unemployed. 35.5% of the mothers were experiencing their first delivery and 68.2% of the pregnant women in this study had had natural vaginal delivery. Some of the psychological issues and problems were also investigated in this study: the pregnancy was intended in approximately 88.2% of the mothers, 6.4% had medical problems in their previous pregnancies, 85.5% were happy with their child’s sex, and 91.8% of them were interested in their pregnancy (Table 1).
Demographic and reproductive information in research units
Demographic and reproductive information in research units
Perceived maternal stress scores at different time point of pregnancy, as well as cortisol and leptin levels (pg/ml) in mothers and babies, are shown in (Table 2).
Maternal perceived stress score and cortisol and leptin levels (pg/ml) in Research Units (Mean±SD)
PSS at different time points of pregnancy, cortisol and leptin levels in mothers and umbilical cord, and neonatal outcomes were compared based on demographic and reproductive information in research units (Table 1) by means of Student’s t-test, ANOVA, and K2; and no significant difference was found among them. Therefore, logistic regression was not used in the data analysis since there was no need to adjust these data according to demographic information.
According to Table 3, 96.4% of neonates were born full term, and 90% of them had no respiratory distress. In addition, 9.1% of the neonates had meconium stained amniotic fluid during delivery, 8.1% had low birth weight (<2500 g), 7.2% had low birth height (<45 cm), 13.2% had a small head circumference (<32 cm), and 9.9% had a low Apgar score (<7).
Information on outcomes of neonates in research units
There was no significant difference between PSS during pregnancy and delivery under the two conditions (yes or no) related to prematurity, respiratory distress, meconium-stained amniotic fluid, low birth weight, low height weight, low head circumference and low Apgar score (Table 4).
Comparison of perceived stress score (PSS) based on neonatal outcomes in research units
The bivariate was compared by student t-test. Although there was no significant difference between yes or no conditions, the PSS was higher in yes state almost in all cases.
Umbilical cords’ cortisol levels were significantly higher in the babies who had meconium stained amniotic fluid than those who did not (p = 0.001) (Fig. 1). In addition, maternal leptin levels were significantly higher in the newborns who had prematurity (P = 0.007), respiratory distress (P = 0.009), low birth weight (P = 0.002), small head circumference (P = 0.014) and low Apgar score (P = 0.006) than those who did not have such problems (Fig. 2A). The umbilical cord leptin level was higher in the neonates who had respiratory distress and those who did not (P = 0.005, Fig. 2B).

The maternal blood cortisol levels at birth time (A) and the cortisol levels in umbilical cord blood (B) based on neonatal outcomes in research units; *indicates significant difference between yes and no condition, P = 0.001.
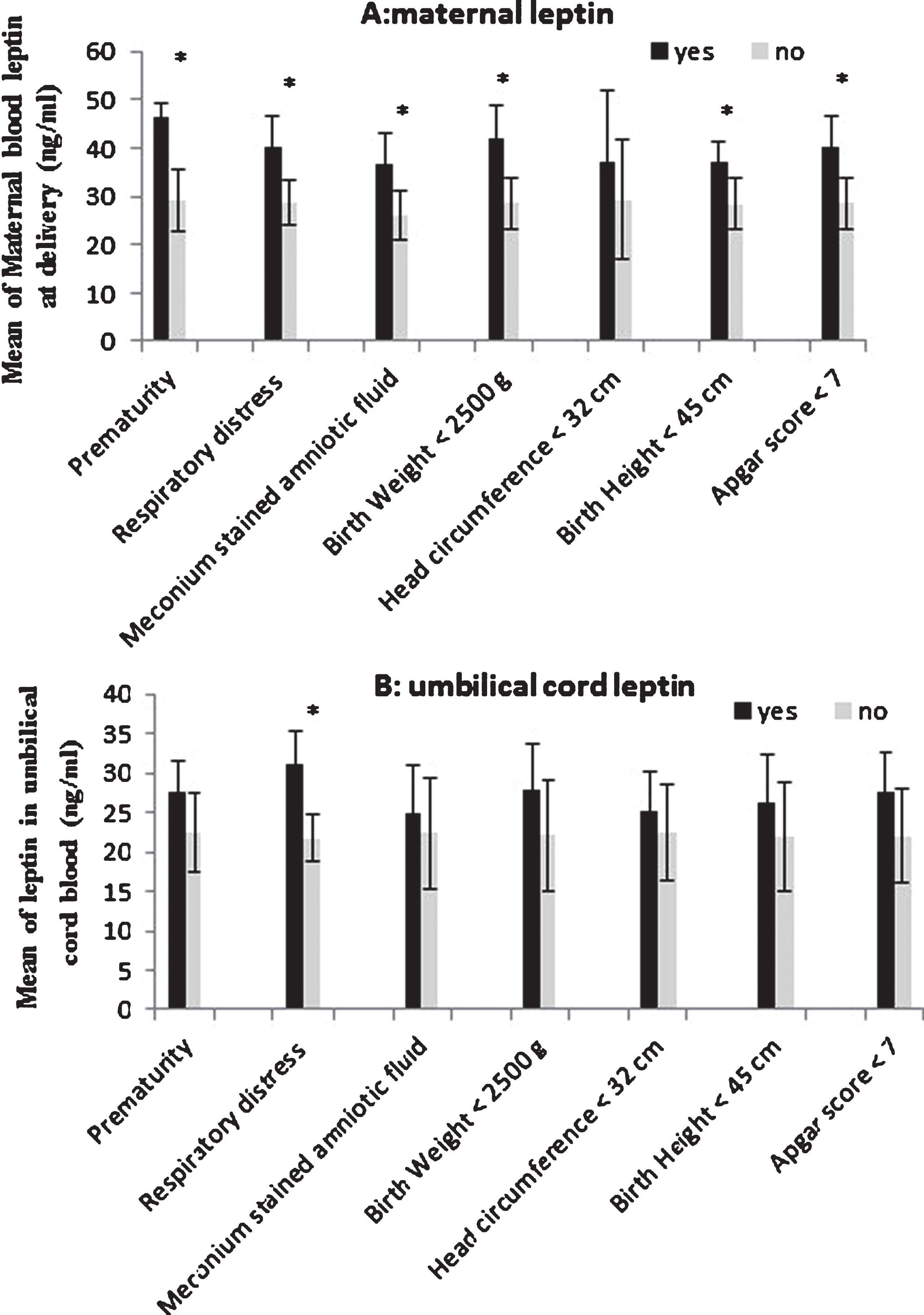
The maternal blood leptin levels at birth time (A) and the leptin in umbilical cord blood (B) based on neonatal outcomes in research units; *indicates significant difference between yes and no condition (panel A P < 0.01, panel B P = 0.005).
Besides, there was a significant correlation between maternal cortisol and PSS during weeks 24–28 and the entire pregnancy (r = 0.246, r = 0.211, respectively; Table 5). A significant negative relationship was observed between PSS during gestation and each of the birth weight and birth length (r = –0.187 and r = –0.214, respectively).
The Relationship between perceived stress score (PSS) with levels of cortisol and leptin at delivery time and umbilical cord as well as with birth weight, birth length, head circumference and Apgar score in research unit
Pearson test, *P < 0.05, **P < 0.01.
A significant positive relationship was observed between umbilical leptin and maternal leptin at delivery (P < 0.001, r = 0.474). Besides, there was a non-significant negative correlation between maternal cortisol and maternal leptin at delivery (r = – 0.168, P = 0.113); the same non-significant negative correlation was also observed in umbilical cortisol and umbilical leptin levels (r = – 0.120, P = 0.259).
The major findings of the present study were as follow: There was a significant correlation between PSS during pregnancy and maternal cortisol level. A significant relationship was also observed between umbilical leptin and maternal leptin levels. Umbilical cortisol levels were significantly higher in the newborns who had meconium stained amniotic fluid as compared with those who did not; moreover, maternal leptin levels were significantly higher in newborns who had prematurity, respiratory distress, low birth weight, small head circumference, and low Apgar score and those who did not have such problems. The umbilical cord leptin levels were also higher in neonates who had respiratory distress than those who did not. The results also revealed a significant negative relationship between PSS and birth weight which is in line with existing literature; It was reported that a significant negative relationship existed between birth weight and mothers’ stress level [23]. In addition, it was reported that women who had higher amounts of stress were more likely to give birth to premature infants [24]. This can be justified with respect to the fact that high levels of stress reduce the blood flow to the womb which may, in turn, lead to low birth weight [25].
The results also indicated that there was not a significant relationship between head circumference, Apgar scores, and stress scores. However, the stress score was higher in neonates with lower Apgar scores and smaller head circumferences. The results of our study are in line with the previous research studies, in which no significant relationship was observed between the Apgar scores and stress scores in the second and third trimester of pregnancy [26, 27]. Similarly, in another study [28] no significant relationship was reported between the neonates’ Apgar score and mothers’ state and trait anxiety from week 32 to week 34 of pregnancy. Besides, it was reported that the overall anxiety can be a predictor of the neonates’ head circumference [27]. The results of the present study revealed that there was a significant negative relationship between neonates’ birth length and mothers’ stress scores, which is in line with the findings of Molavi et al. (2004) who found a significant negative relationship between mothers’ stress and neonates’ length, as well as Apgar score and head circumference. The positive correlation between meconium-stained amniotic fluid (meconium expulsion) and high PSS can be justified with respect to the fact that high PSS can cause irregular and shallow breathing in the pregnant mother which results in oxygen deficiency in the fetus which in turn leads to more distress in the fetus and thus meconium-stained amniotic fluid. On the other hand, inadequate removal of meconium from the airway prior to the first breath and use of positive pressure ventilation prior to clearing the airway of meconium increase the likelihood of a neonate developing meconium aspiration syndrome [29]. In general, meconium-stained amniotic fluid is related to prenatal mortality and pathogenicity [30]. Therefore, stress causes meconium-stained amniotic fluid and respiratory distress during labor and hence low Apgar score in the neonates.
It has been reported that stress during gestation leads to an increase in offspring glucocorticoids’ levels [1, 31–33]. This can be due to the fact that severe stress affects HPA axis and Sympathetic Nervous System (SNS) and leads to neurological changes of endocrine glands and affects Adrenocorticotropic (ACTH) hormone secretion and increases plasma levels of glucocorticoids [34, 35]. Meanwhile, as the pregnancy progresses, the maternal HPA axis becomes gradually less responsive to stress and only a weak association between maternal emotional state and the woman’s cortisol level are seen in the pregnancy [34, 36]. Furthermore, the placenta inactivates a significant percentage of maternal glucocorticoids via 11β-hydroxysteroid dehydrogenase type 2 (11-βHSD2) during transfer to the fetus [37]. Our data is in line with the existing literature since, as presented in the result section, there was a significant positive relationship between PSS and maternal cortisol levels.
The findings of this study regarding the significant relationship between maternal leptin levels and birth weight, length, and head circumference were in line with Larijani and Ghodsi (2005) in which infants’ BMI has a direct relationship with leptin serum levels. It has also been reported that birth weight has a relationship with umbilical cord leptin levels [38]. In the current study, a significant positive relationship was observed between maternal leptin levels at delivery and umbilical leptin levels. Approximately 95% of leptin in placenta spreads in mother’s blood [39]. Thus, the correlation between leptin levels in mothers and umbilical cords is probably due to its spread between mother and her fetus, through the placenta. In a systematic review consisting of 44 relevant studies, Karakosta et al. (2011) reported a positive correlation between leptin levels and birth weight; results were similar in males (r = 0.55) and females (r = 0.60), and between Caucasians and eastern Asian populations [40]. Our finding was not consistent with the result of this study. Our study showed a higher leptin level in newborns with poor outcomes such as having respiratory distress. Evidence suggests that stress and leptin stimulate SNS activity [41]. It is likely that higher activation and increased sensitivity of SNS in the mothers can be the reason for poor neonatal outcomes in these subjects. Unfortunately, we did not measure SNS activity in the current study. Also, the PSS was non-significantly higher in mothers who had a premature delivery. The number of premature neonates was very small (3.6%) in this study; It can be estimated that if the number of premature babies was higher, the difference might have been significant. On the other hand, in the present study, a significant relationship was not observed between PSS and leptin levels in mothers and umbilical cord. It is reported that women with larger waists had greater stress-induced increases in plasma leptin. Similarly, women with higher basal leptin displayed greater stress-induced increases in heart rate and plasma interleukin-6, and larger decreases in heart rate variability and cardiac pre-ejection period [41]. Our finding was not consistent with these data; the mismatch might be from the subjects and the methods used in the studies. Unfortunately, we did not find a relevant study in pregnant women to compare the results.
Our findings indicated that there was a significant relationship between mothers’ stress score and cortisol levels during delivery. This can be justified with respect to the fact that during stressful conditions HPA axis is activated and increases cortisol secretion [32, 33]. Kammerer et al., (2002) also showed that there is a high correlation between mothers’ and infants’ blood plasma cortisol levels and maternal blood cortisol has a direct effect on fetal development. Increase in the levels of cortisol quickly affects the fetus and causes problems in the development process of the offspring [42–44]. The strengths of this study were that the participants’ stress levels were evaluated in four stages and it was a longitudinal study. In all stages of the research, the researcher monitored the filling out of the questionnaires. The participants’ not giving proper answers to the questions can be considered as one of the limitations of a study which was controlled to a large extent by the presence of the researcher while the questionnaires were filled out in order to answer any probable questions and also to state that the answers would be kept confidential. The participants’ personal, cultural, and emotional differences can be effective in their answers to the questions. The reason for some mismatch between the results of other studies with the present study can be the use of different instruments for evaluation of stress during pregnancy. Besides, a longitudinal study on this topic had not been conducted in Iranian context before and hence there is a need for more research to confirm the relationship between the variables.
Conclusion
The result of the current study confirmed that higher PSS during pregnancy leads to lower growth and development in the fetus which, in turn, results in higher fetal distress. The probable cause of some of these results can be attributed to increased maternal leptin and cortisol levels. Changes in maternal neuroendocrine can lead to increased fetal cortisol and leptin levels. It might be concluded that maternal leptin level can be a better predictor of fetal distress in high-stress pregnancies.
Disclosure statements
The authors have no conflicts of interest to declare regarding the study described in this article and the preparation of the article.
Footnotes
Acknowledgments
This study is derived out of a thesis (master degree) presented at Urmia University of Medical Sciences and was carried out by the financial support of Urmia University of Medical Sciences. Hereby, we sincerely thank the research department of Urmia University of Medical Sciences, the staff of health care centers and Fatemeh Zahra Hospital of Miandoab city, and all of the participants, without whose kind cooperation it would have been impossible to carry out this research.