
Abstract
AIM:
To evaluate outcomes of a cohort of infants born at 23 weeks’ gestational age after introducing a new selection score for resuscitation in the delivery room (DR).
METHODS:
This was a retrospective charts review study using data from the maternal and newborn registry funded by the Qatar National Research Fund. Parents were consulted prenatally and their wishes were honored. The plan of resuscitation was based on the new selection score. The seven components of the score were four antenatal and three immediate postnatal in the DR. Each component received a score of zero, one, or two according to its presence, uncertainty or absence, respectively. Only a score of≥7 would receive active resuscitation unless specified otherwise during prenatal consultation.
RESULTS:
The study reviewed 60 infants that were delivered over a two year period. The DR death rate was 23 of 60 (38%). Thirty-seven infants (61%) were admitted to the NICU. The score was applied only on 37 infants where all score criteria were reported in their files. Twenty infants had score <7; of them 13 (65%) died in the DR and 7 were admitted to NICU of whom two (29%) survived to discharge. Seventeen babies with scores≥7 admitted to NICU of whom nine (51%) survived to discharge. The survival rate to discharge was 13 of 37(35%). A satisfaction survey included 33 neonatal physicians; 32 neonatologists stated the score was easy to comprehend, 26 voted for easy to implement, and 30 voted for ethical relief and moral comfort.
CONCLUSIONS:
Using a resuscitation score of seven was associated with improved survival until the discharge of those infants resuscitated. NICU physicians described the score as functional and convenient.
Keywords
Abbreviations
Delivery room Extreme low birth weight Neonatal intensive care unit Pulmonary interstitial emphysema Qatar National Research Fund Vaginal delivery/Cesarean section Women’s Wellness and Research Center
Introduction
Neonatologists operating in the tertiary neonatal intensive units (NICUs) have mixed feelings about resuscitation, admission, and managing infants born at 23 weeks’ gestational age, which is judged to be the limit of viability. NICU services are judged by their level of sophistication in managing infants born at the limit of viability in terms of their survival until discharge. NICUs are keen to achieve favorable two-year neurodevelopmental outcomes among these infants [1]. In Japan, Nazomi et al. reported survival of 65% and cerebral palsy as low as 18% in the NICU [2]. These and other encouraging published reports regarding the survival and outcomes of infants born at 23 weeks, ethical and cultural obligations to provide care for all infants, and social and political expectations to be good stewards of healthcare spending have led advanced healthcare policymakers to demand similar outcomes from their NICUs [2]. To care for these infants with evidence-based medical practice, it is crucial to comprehend the embryology and physiology of this gestational age and the immaturity of their organs, and how these factors impact their survival [2]. The American Academy of Pediatrics published guidelines in 2009, updated in 2015 that noted the wide variation in approaches, outcomes, and decision-making processes in managing infants born at the limit of viability [3]. Over the past several decades, advances in perinatal and neonatal care have improved the survival of even the most immature infants, increasing and diversifying our knowledge of the causes of death in preterm infants [3, 4]. The Epicure study reported that 64% of infants born at 23 weeks were resuscitated and admitted alive to the NICU, and 40% survived until 28 days; 30% survived to discharge [5]. In a 2014 review of the Epicure study, there were 284 live births at 23 weeks’ gestation with intended care, of which 217 (76%) were admitted to the NICU and 151 infants (69%) died before discharge. A few publications have addressed or focused on this particular gestational age [6, 7]. Our hospital, Women’s Wellness and Research Center (WWRC), is a state-of-the-art tertiary women’s hospital with 40 to 50 deliveries daily. WWRC accommodates 214 maternity beds and 11 NICU cots, and it is a referral hospital for three governmental and five private maternity services. In 2004 and 2005, 12 infants at 23 weeks’ gestation were admitted to our NICU, and only one survived to discharge (9%). Since 2009, we have been encouraged to admit infants of this gestational age to our NICU, but not more than 18% of these have survived to 1 years, and the average length of stay for those who survived was 140 days. In this study, we measured the probability of death before and after introducing the resuscitation score (the score of seven) targeting 23 weeks’ gestational age.
Methodology
This population-based retrospective study was designed to assess the mortality and survival rate of all extremely low birth weight (ELBW) infants born at 23 weeks’ gestation in WWRC to residents of Qatar from 2016 to mid-2018. We evaluated outcomes for these infants both before and after introducing resuscitation guidelines concerning the limit of viability at 23 weeks’ gestation. We retrieved the medical records of each infant from the Pearl-Peristat Maternal and Newborn registry and the Vermont Oxford database related to our hospital. We selected liveborn cases at between 23 weeks + zero days and 23 weeks + 6 days who were born in, died in, or admitted to the NICU. Gestational age estimates were verified using maternal ultrasound, dates of in vitro fertilization, first-trimester ultrasound, or menstrual dating confirmed by second-trimester ultrasound. The study excluded confirmed intrauterine fetal deaths and infants with significant anomalies. It included infants for whom resuscitation was attempted in the DR. The rates of the NICU admission, death before 2 weeks of age, and death before discharge were assessed. We also evaluated complications during the first 2 weeks associated with death to measure the probability of death where such complications occurred. We evaluated the best evidence available from the literature [8–16] reflecting antenatal risk factors associated with death at this age of gestation and level of intrauterine maturation. We selected seven parameters supported by the evidence as being the most crucial for potential survivability or death at this gestational age (Fig. 1). The designed score accommodated evaluative subjectivity, ambiguity of clinical features, and unknown clinical information. The score took into consideration parental wishes not to proceed with resuscitation based on information conveyed to them before delivery. However, parents were advised not to ask for resuscitation if the score were to be less than 7 as per institution’s guidelines. We allowed some exceptions such as when conception occurred via in vitro fertilization and with history of infertility. We assessed each newborn independently from gender, multiple births, and birth order or ethnicity. Before applying the score, we obtained the approval of the NICU and then the Women’s Hospital Board of Ethics. Seven elements were chosen in all: four antenatal (gestational age, chorioamnionitis, estimated birth weight, and antenatal steroids) and three immediately postnatal (confirmation of birth weight, bruises, skin friability, and fusion of the eyelids). Each component received a score of 0, 1, or 2 according to its presence, uncertainty, or absence, respectively. Newborns were not resuscitated if the total score was below 7 and were actively resuscitated and admitted to the NICU if the score was equal to or greater than 7. The protocol was implemented in February 2018. A satisfaction survey was administered 6 months after the application of the system to evaluate the medical staff’s comprehension of the system, judgment of its practicality, and ethical comfort with its guidelines.
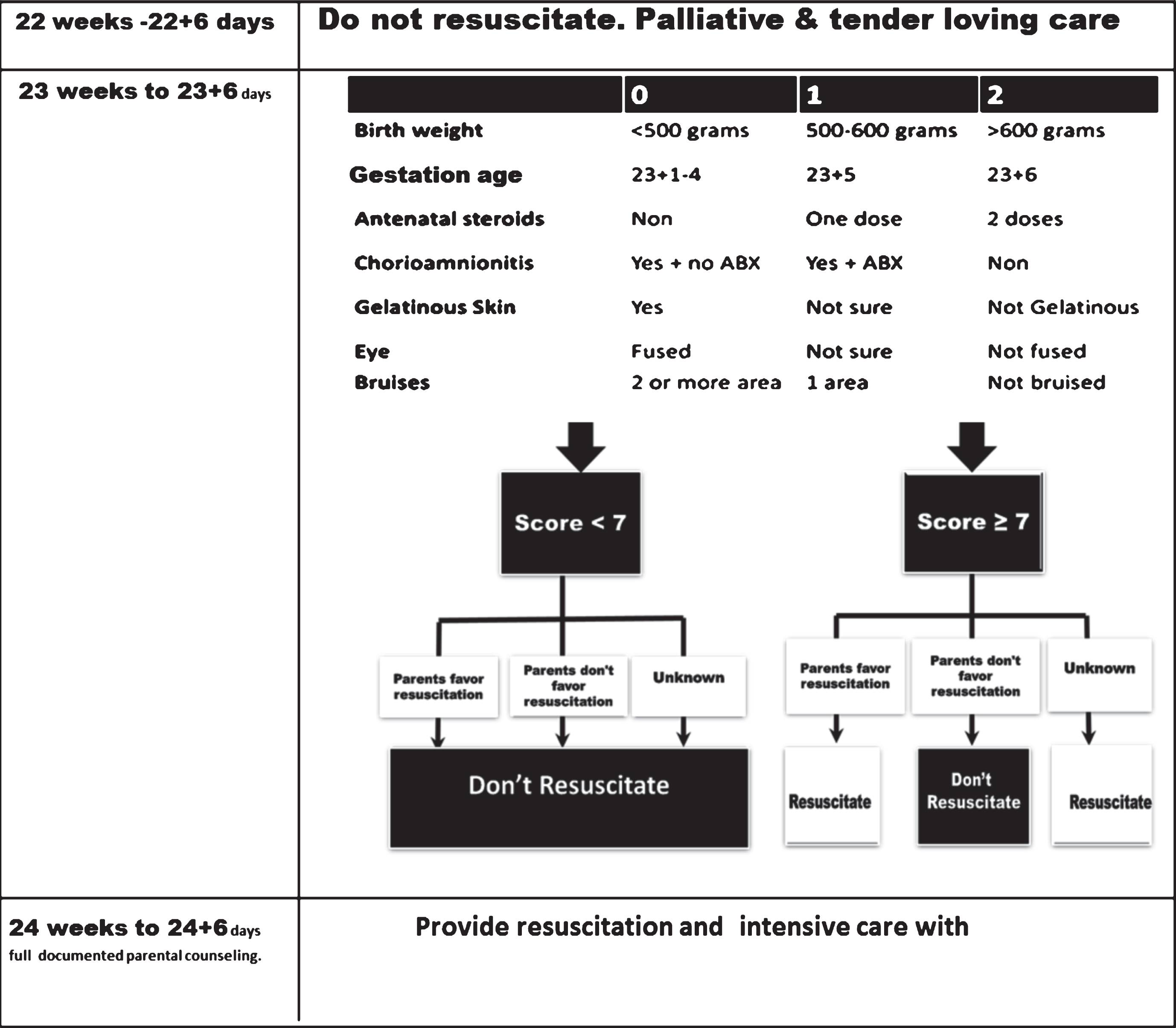
Limit of viability, 22–24 weeks’ gestation resuscitation decision-making guidelines. Unknown: Rapid delivery without meeting parents, no antenatal consultation, and mother cannot be approached (in active labor) or inapproachable husband/partner; multiple pregnancies: Each is evaluated as an individual case. Chorioamnionitis: clinically active symptoms within 1 week of labor. Assisted pregnancy due to long infertility (IVF) needs special consideration. Significant bruises: bruises involve two or more of (head & scalp), trunk & limbs.
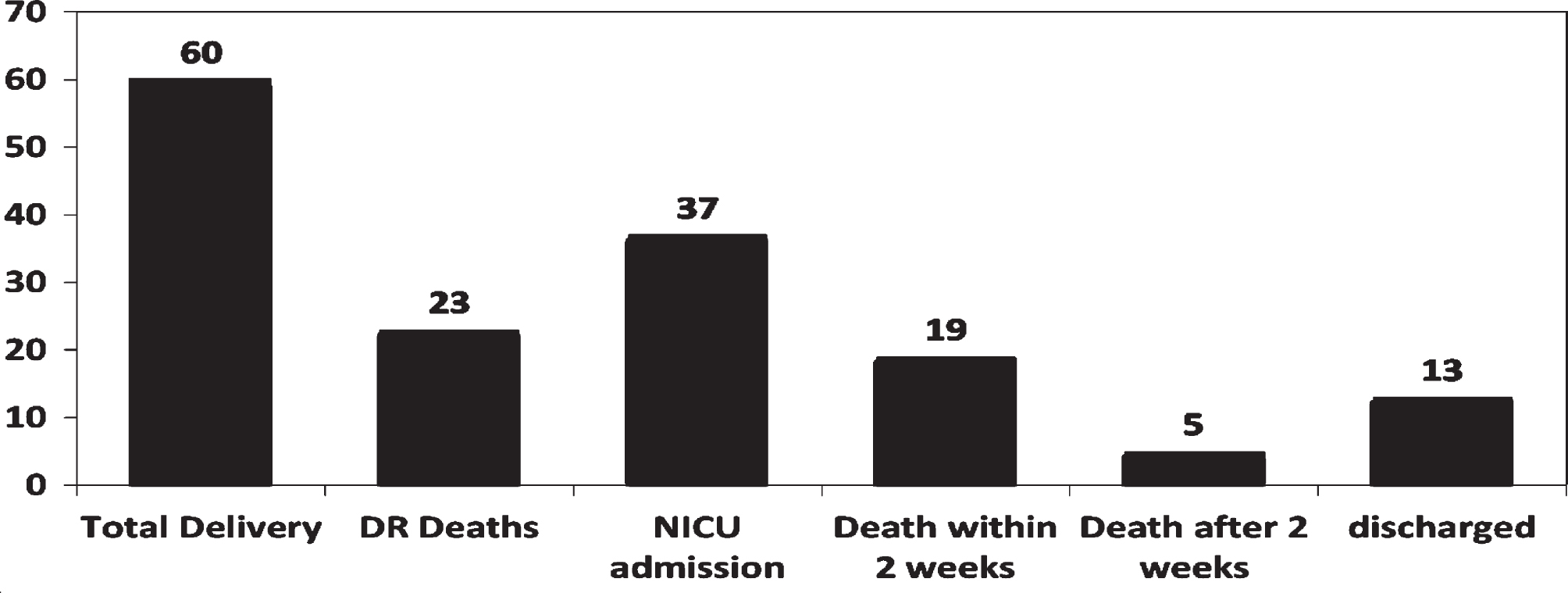
Total number of infants dying within the first two weeks versus those dying after two weeks versus survival to discharge.

Impact of applying resuscitation score on 23 weeks’ gestation infants*. *Only 37 of 60 newborns had full score characteristics in their health records.
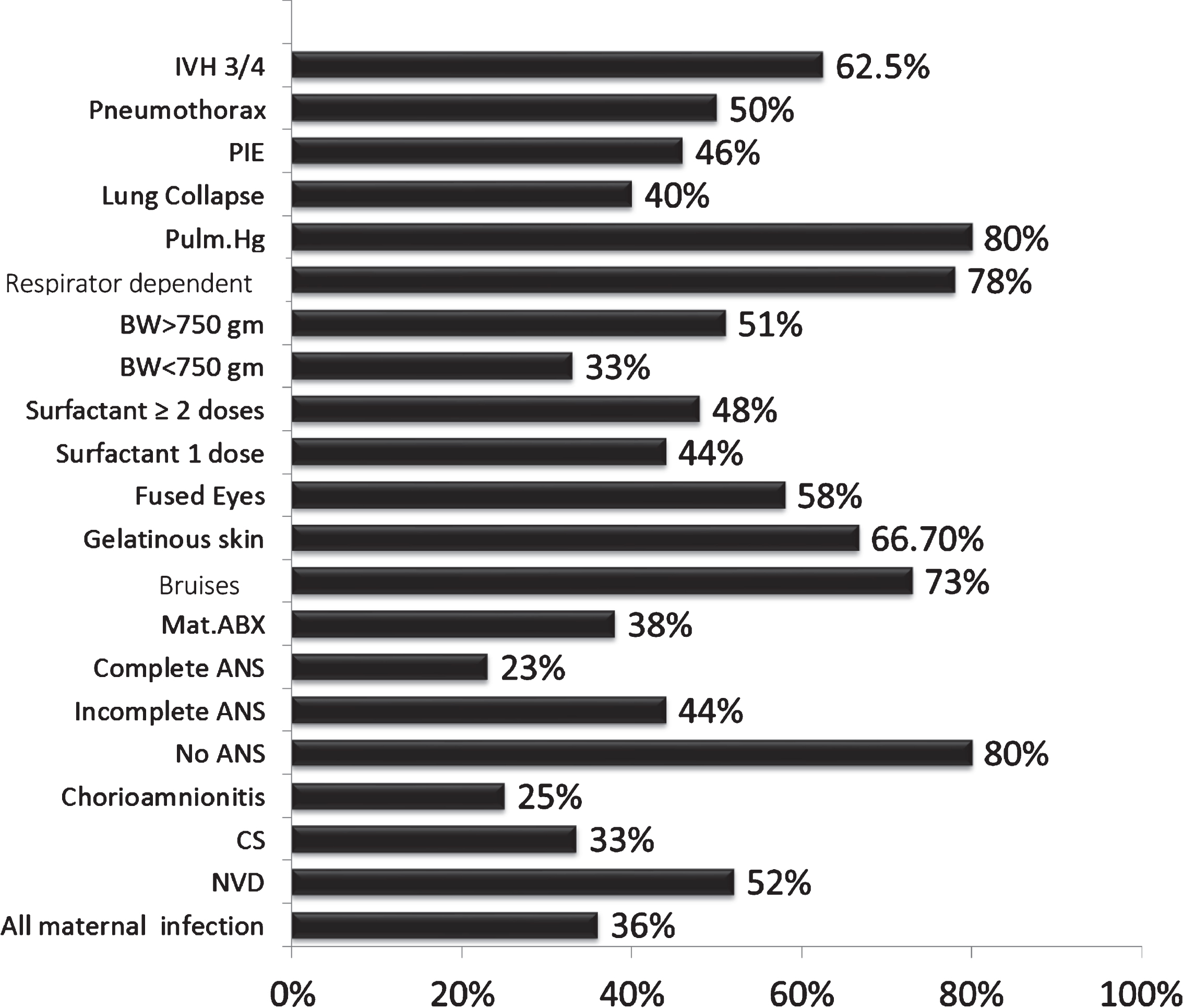
Death-related risk factors in 60 preterm, 23 weeks’ gestational age infants.
Odds ratios for death at two weeks for 60 infants at 23 weeks’ gestation
†Statistically significant at p < 0.05.
Sixty infants delivered from January 2016 to June 2018 were investigated for a mortality-associated risk assessment. The DR death rate was 23 of 60 (38.3%), 37 infants were admitted to the NICU (61.7%), and half of those admitted died before 2 weeks of age. The survival rate to discharge was 35% (13 of 37). Only 37 of 60 infants had fully described selection components, and their survival rate was analyzed using this score. Of infants with a score <7, 13 of 20 (65%) died in the DR, compared with 0 of 17 with scores≥7 dying in the DR. Amongst infants admitted to the NICU, seven had a score <7, of whom two (29%) survived to discharge, while 17 had a score≥7, of whom nine (51%) survived to discharge. On a satisfaction survey administered to 33 neonatal physicians, 32 felt that the system was easy to comprehend, 26 concluded that it was easy to implement, and 30 reported that using the resuscitation protocol provided ethical relief and moral comfort to both parents and medical providers, leading to less moral distress and questions regarding the standard of evidence-based care for these extremely prematureinfants.
Discussion
Birth before 24 weeks’ gestation remains frightening and ethically challenging for both parents and medical professionals. Parents often lack knowledge of the outcomes and complications among these very premature infants, and it is common for there to be anxiety about the future and fear of having a disabled child. Medical professionals have a medico-legal and ethical responsibility to each infant and family, a mandate to conserve available resources, and face the high possibility of an unfavorable outcome. They must also pay vigilant attention to outcome measures over a very long time. “Optimal” perinatal care for infants born at the limit of viability remains unclear, varying significantly across several reports [2, 17–19]. While these complexities are well-established, increasing evidence from the NICUs in Japan and other regions suggests favorable outcomes are possible. However, in practice, Qatar and other countries around the world have no formal national consensus regarding the standard of care at this gestational age, leading to variation between tertiary institutions and their referring regional hospitals. Differences between local and international practice make comparisons between centers difficult. Outcomes at some centers might reflect deficiencies in expertise or technology. Many centers report widely different rates of antenatal corticosteroid use, operative birth, and other perinatal care strategies that could explain the variations in morbidity and mortality [18–20]. Furthermore, early trimester dating scans have a margin of error of at least one week, which undermines treatment-threshold decisions based on gestational age alone [21]. Similarly, other variables, including corticosteroid exposure, can significantly modify survival risk [22]. Medico-legal conflicts, the need for very long hospital stays, eventual death after long periods of struggle, and parents’ frustration, which can lead to separations and even divorce, are all crucial factors to consider when developing and implementing a meaningful scoring system. Evidence-based knowledge is complicated by human subjectivity and possibly sub-optimal decision-making skills. The score of seven presented here identifies infants with enough potential for resuscitation while providing guidance for infants who present with less potential. In every instance, parents’ wishes were addressed and discussed before the final decision and thoroughly explained to parents. The score was designed to accommodate uncertain physical signs, particularly signs of maturation. As the primary objective in this study, we report the survival rate rather than the two-year outcome. Applying the score did not increase labor room deaths; indeed, they fell marginally, by 7%. The score may have helped physicians decide when to attempt resuscitation before birth, as four of seven components of the score are calculated before delivery. Since is scoring system was supported by the hospital administration and approved by the Board of Ethics, clinicians were able to handle these resuscitations more comfortably without any overwhelming ethical decisions or responsibilities.
The current study reports a survival rate of 35% to discharge. This is lower than some centers have reported [23, 24], while meeting or exceeding survival rates at other centers [2, 26]. We therefore propose that the score of seven represents is a practical, convenient, and ethically sound approach to this particular gestational age, based on evidence, which can solve the significant confusion among healthcare professionals. Although this score should be applied consistently to achieve maximal benefit, an individualized approach to decision-making must be used where applicable.