
Abstract
BACKGROUND:
The objective of this study is to evaluate the obstetric outcomes of pregnancies with congenital diaphragmatic hernia (CDH).
METHODS:
Fifty one pregnancies prenatally diagnosed with CDH at our institution between January 1, 2002 and August 31, 2018 were retrospectively evaluated. The pregnancies were divided into two groups according to neonatal survival. Demographic features, clinical characteristics and prognostic factors were compared between the neonatal survival (n = 16) and non-survival (n = 28) groups. Cut-off values of fetal lung area to head circumference ratio (LHR), observed/expected LHR (o/e LHR) and observed/expected total fetal lung volume (o/e TFLV) for neonatal survival were calculated.
RESULTS:
Thirty six (70.6%) and fifteen (29.4%) fetuses had left and right sided CDH respectively. Seven patients chose termination of their pregnancies (13.7%). Statistically significant differences were found between survival and non-survival groups in terms of parity, median gestational week at diagnosis, polyhydroamniosis rate, CDH type, stomach position, liver position, median LHR, o/e LHR, o/e TFLV, median 5th minute Apgar score and neonatal operation rate values (p values were 0.03,<0.001, 0.02, 0.006,<0.001, 0.006,<0.001,<0.001,<0.001, 0.04 and <0.001 respectively). According to ROC curve analysis, 1.05 (82% sensitivity, 74% specificity) for LHR, 22.5 (78.6% sensitivity, 73.9% specifity) for o/e LHR and 23.5 (85.7% sensitivity,74.2% specificity) for o/e TFLV were determined to be cut-offs for neonatal survival, respectively, with highest sensitivity and specificity.
CONCLUSION:
Earlier gestational week at diagnosis, right sided CDH, presence of liver herniation, supradiaphragmatic stomach position, lower LHR, o/e LHR and o/e TFLV were associated with decreased rates of neonatal survival.
Keywords
Introduction
Congenital diaphragmatic hernia (CDH) is a developmental disorder of the diaphragm which results in abdominal viscera herniation into the fetal chest [1]. The prevalence of CDH is approximately 1 to 4 per 10,000 live births [2]. Although the diaphragmatic defect may be repaired surgically in the postpartum period, CDH related pulmonary hypoplasia together with pulmonary hypertension can lead to increased neonatal morbidity and mortality [3–6]. The vast majority of CDH occurs sporadically, while familial cases involving autosomal recessive, autosomal dominant, and X-linked inheritance patterns have been reported [7]. Approximately 70% of CDH cases are isolated [1]. On the other hand, CDH can be associated with major structural malformations, chromosomal abnormalities and single gene disorders. Invasive prenatal diagnostic tests (IPDT)s may be performed in case of suspected genetic syndromes [8, 9]. Mortality rates still range between 30–50%, despite advances in the field of neonatal intensive care and pediatric surgery [10]. The prognosis for survival of neonates with CDH depends on various antenatal factors [3–6]. Cases with chromosomal abnormalities, severe congenital malformations, hydrops fetalis, right-sided CDH, liver herniation and lower fetal lung volume generally have worse prognosis [3–6]. Appropriate prenatal prognostic assessment is crucial in order to give families proper antenatal counselling. Determining the candidates for termination of pregnancy (TOP), intrauterine fetal therapy and postnatal extracorporeal membrane oxygenation (ECMO) is a pivotal step in providing optimal perinatal management protocols [1, 11]. However, management of pregnancies complicated with CDH may be challenging for physicians [3–6]. Hereby, various ultrasonographic parameters are used for the estimation of neonatal prognosis. Fetal lung area to head circumference ratio (LHR), observed/expected LHR (o/e LHR) and observed/expected total fetal lung volume (o/e TFLV) are the most commonly used parameters used for the assessment of neonatal prognosis [3–6]. It has also been reported that fetal magnetic resonance imaging (MRI) has come into practice for further evaluation of fetuses complicated by CDH [12]. Fetal endoluminal tracheal occlusion (FETO) is an investigational procedure that may prevent or reverse pulmonary hypoplasia and may provide adequate lung growth for neonatal survival [13]. It seems to be the only intrauterine intervention with favorable neonatal outcomes for the time being [13]. On the other hand, this procedure requires a fetoscopic approach and it may lead to preterm delivery in approximately 17% of the cases [14]. Thus, choosing the suitable cases for FETO is critical for physicians. Primary or patch repair of the diaphragmatic defect may be performed depending on the clinical characteristics [15, 16]. Although early intervention was preferred in the past, at present surgery is delayed until stabilization of the neonate [17]. However, neonates with severe pulmonary hypertension and pulmonary hypoplasia mostly die without an opportunity for an intervention [17]. For this reason, TOP may be a reasonable option for fetuses with poor prognostic factors.
The objective of this study was to evaluate the obstetric outcomes of pregnancies with CDH at our clinic and to compare the pregnancies with survival and non-survival neonates in terms of demographic features, clinical characteristics and obstetric outcomes. Additionally, we aimed to determine cut-off values for LHR, o/e LHR and o/e TFLV in order to predict neonatal survival.
Materials and methods
This retrospective cohort study was conducted at Hacettepe University Hospital, Division of Perinatology. Pregnancies prenatally diagnosed as CDH at our institution between January 1, 2002 and August 31, 2018 were included in the study (n = 51). The required data were obtained from the perinatal medicine electronic database. The cases were evaluated in terms of demographic features, clinical characteristics, obstetric outcomes, prognostic ultrasound findings and neonatal interventions. Rates for TOP, IPDT, chromosomal abnormality, coexisting congenital anomalies and mean gestational week for TOP were recorded. Thereafter, the remaining cases were divided into two groups depending on neonatal survival. Median maternal age, rates of nulliparity/multiparity, median gestational week at diagnosis, polyhydramniosis rate, CDH type, fetal stomach and liver position, LHR, o/e LHR, o/e TFLV, median gestational week at birth, birthweight, 5th minute Apgar score, mode of delivery, neonatal operation rate and necessity for ECMO were compared between the neonatal survival (n = 16) and non-survival (n = 28) groups. Additionally, cut-off values of LHR, o/e LHR and o/e TFLV for neonatal survival were calculated. The pregnant women were registered in a special antenatal care program provided by a multidisciplinary team (perinatologist, pediatric surgeon and neonatologist) after the diagnosis of CDH. Pregnancy follow-up consisted of serial ultrasonography to evaluate fetal growth, genetic consultation (fetal karyotype analysis was performed in appropriate cases), fetal anatomy scanning, oral glucose challenge test (between 24th–28th gestational weeks), and non-stress test weekly (after the 28th gestational week). Measurements of LHR, o/e LHR and o/e TFLV were performed using antenatal ultrasonography [18–20]. Total fetal lung volume was calculated by two-dimensional ultrasonography in all cases [21]. Magnetic resonance imaging was not used in any of the cases due to cost-effective issues. Fetal stomach position was recorded according to the method used by Basta et al. [22]. Polyhydramniosis was defined as an amniotic fluid index of >24 cm [23]. Fetal tracheal occlusion could not be performed in any of the cases due to the lack of technical devices. The mode of delivery was determined according to the clinical characteristics of the cases and obstetrical indications. Neonates were immediately intubated in the delivery room and transferred to the neonatal intensive care unitafter delivery.
Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS.22, IBM SPSS Statistics for Windows, Version 22.0 Armonk, NY: IBM Corp.). Variables were investigated using visual (histograms, probability plots) and analytical methods (Shapiro-Wilk’s test) to determine whether they were normally distributed. Descriptive analyses are presented as medians and interquartile range for non-normally distributed variables. As continuous variables were not normally distributed, Mann-Whitney U test was conducted to compare the median values among the groups. An overall 5% type-I error level was used to infer statistical significance. Categorical variables were defined based on numbers and percentages. Categorical variables were compared with Fisher’s exact or chi-square test as appropriate. Receiver operating characteristic (ROC) curves were used to assess the performance of LHR, o/e LHR and o/e TFLV values in predicting neonatal survival. ROC curves plot the true positive rate (sensitivity) against the false positive rate (1-specificity) for possible cut-off values. The area under the curve corresponds to the probability that the criterion will correctly classify a random observation; an area under the curve >0.5 indicates that the criterion is superior to chance. A two-tailed p value <0.05 was regarded as statistically significant. The study protocol was approved by the Hacettepe University Ethics Committee (GO 16/189). Written informed consent was obtained from all patients.
Results
Mean maternal age was 28.55±5.35 (range, 18–40) and 50.9% of the pregnant women were nulliparous (26/51). Mean gestational week at diagnosis was 22.39±3.53 (range, 18–30). Fetal karyotype analysis by amniocentesis was performed in 8 cases (15.7%) and all were reported to have a normal karyotype. Thirty-six (70.6%) fetuses had left sided CDH and 15 (29.4%) fetuses had right sided CDH. There were no bilateral hernias. There were two (3.9%) prenatally detected coexisting congenital structural abnormalities: one single umbilical artery and one limb-body wall complex.
After appropriate counselling, seven families chose TOP (six left sided, one right sided CDH) (13.7%). Mean gestational week for the TOP was 20.10±3.65 (range, 19–24). Three of the seven patients with TOP underwent amniocentesis (all had a normal karyotype). Limb-body wall complex was detected in one of the terminated fetuses. There were no detected structural abnormalities in the remaining terminated fetuses. The remaining 44 cases ended with live fetuses. Survival (n = 16) and non-survival (n = 28) groups were comparable for median maternal age, gestational week at birth and birth weight (p values were 0.49, 0.58 and 0.11, respectively). Flow diagram describing the patient inclusion, exclusion and selection was shown in Fig. 1. Furthermore, there were not significant differences between the groups for the mode of delivery and neonatal ECMO therapy (p values were 0.57 and 0.07, respectively). However, significant differences were found between the groups for parity, median gestational week at diagnosis, polyhydroamniosis rate, CDH type, stomach position, liver position, median LHR, o/e LHR, o/e TFLV, median 5thminute APGAR score and neonatal operation rate values (p values were 0.03,<0.001, 0.02, 0.006,<0.001, 0.006,<0.001,<0.001,<0.001, 0.04 and <0.001, respectively) (Table 1).
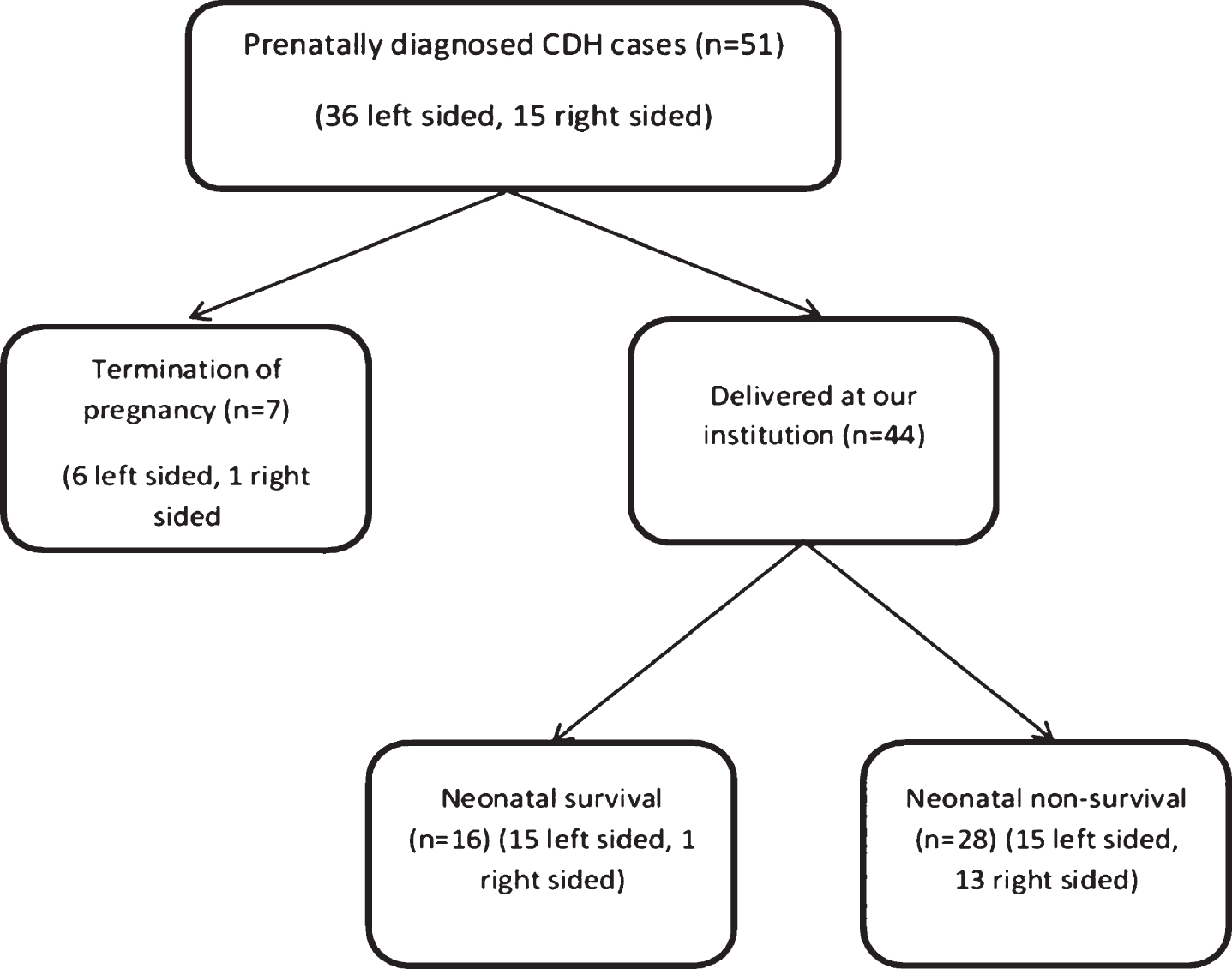
Flow diagram describing the patient inclusion, exclusion and selection (CDH: Congenital diaphragma hernia).
Comparision of survival and non-survival CDH groups in terms of demographic features, clinical characteristics and obstetric outcomes
CDH: Congenital diaphragmatic hernia, LHR: The lung area to head circumference ratio, o/e LHR: Observed/expected lung-to-head ratio, o/e TFLV: Observed/expected total fetal lung volume, ECMO: Extracorporeal membrane oxygenation. Data presented as % (n/total) or median (range), Mann-Whitney U, chi-square or Fisher’s exact test was performed for the statistical analysis as appropriate.
Results of the ROC analysis for assessing the performance of LHR, o/e LHR and o/e TFLV values in predicting neonatal survival are shown in Table 2, and ROC curves are shown in Fig. 2. Area under the curve (AUC) values were calculated as 0.810 (95% CI: 0.671–0.949), 0.857 (95% CI: 0.745–0.969) and 0.881 (95% CI: 0.784–0.978), respectively. As a result, 1.05 (82% sensitivity, 74% specificity) for LHR, 22.5 (78.6% sensitivity, 73.9% specifity) for o/e LHR and 23.5 (85.7% sensitivity, 74.2% specificity) for o/e TFLV were determined to be cut-offs for neonatal survival, respectively, with highest sensitivity and specificity.

ROC curves for assessing the performance of LHR, o/e LHR and o/e TFLV values in predicting neonatal survival (LHR: Fetal lung area to head circumference ratio, o/e LHR: Observed/expected LHR and o/e TFLV: Observed/expected total fetal lung volume).
ROC curve analysis for assessing the performance of LHR, o/e LHR and o/e TFLV in predicting neonatal survival
ROC: Receiver operating characteristic, CI: Confidence interval LHR: The lung area to head circumference ratio, o/e LHR: Observed/expected lung-to-head ratio, o/e TFLV: Observed/expected total fetal lung volüme, AUC: Area under the curve, Std. error: Standard error.
The non-survival group had a lower median gestational week at diagnosis, LHR, o/e LHR, o/e TFLV, 5thminute Apgar score and neonatal operation rate compared to the survival group in this study. Furthermore, the non-survival group had higher rates of polyhydramniosis, right-sided CDH, mid-to-posteriror or retrocardiac stomach position and liver herniation. Although the postpartum ECMO application rate was lower in the non-survival group (14.3% vs 37.5%), this difference did not reach statistical significance. These findings indicated that postnatal prognosis was closely related to prenatal risk factors, as reported in previous studies [3–6]. Additionally, cut-off values of 1.05, 22.5 and 23.5 were found for LHR, o/e LHR and o/e TFLV measurements with highest sensitivity and specificity using ROC curve analysis. These cut-off values were also consistent with the current literature [3–6].
Gestational age at diagnosis has been debated as a prognostic factor for neonatal survival in the literature [3]. While some studies reported higher rates of neonatal mortality in cases diagnosed before the 25th gestational week, others found no association with postnatal prognosis [3, 24]. The non-survival group had a median value of 20 and the survival group had a median value of 27 for gestational week at diagnosis in this study. This finding was most probably due to the earlier ultrasonographic detection of larger defects at earlier gestational weeks.
Polyhydroamnios is usually associated with diminished fetal swallowing of amniotic fluid with increased herniation of the fetal visceral organs into a larger defect [18]. However, a statistically significant correlation could not be shown in most of the previous studies [18, 26]. The polyhydroamnios rate was 28.6% in the non-survival group and 6.25% in the survival group in this study.
Right sided CDH was found to be associated with worse prognosis [27, 28]. Rates of neonatal mortality, morbidity, requirement for ECMO and patch repair surgery were higher in cases with right sided CDH [27, 28]. There were 13 cases (46.4%) with right sided CDH in the non-survival group and only one case was observed (6.25%) with right sided CDH in the survival group. Our findings were consistent with the literature [27, 28].
Using stomach position for the prognosis of CDH is considered an easy and objective method [4, 29]. Neonatal morbidity, mortality, necessity for ECMO and prolonged mechanical ventilation in cases with isolated left CDH may be assessed by the position of the fetal stomach according to some studies [4, 29]. While intraabdominal stomach position was associated with the most favorable outcomes, retrocardiac stomach position resulted in the worst outcomes [4, 29]. Stomach position may also be used to indirectly determine the liver position. Furthermore, similar predictability in outcomes as liver position and LHR was reported in the literature [22]. However, fetal stomach position is not yet considered as a standard predictor of outcome due to high rates of interobserver disagreement [30].
Liver herniation was reported to be one of the most reliable prenatal predictors of postnatal survival [31]. Significantly higher rates of neonatal mortality were reported in cases with fetal liver herniation [31]. Either ultrasonography or fetal MRI can be used in order to assess the position of the liver [31]. In particular, ultrafast fetal MRI using rapid HASTE technique is reported to be the most powerful tool to accurately demonstrate liver herniation [32]. Although the sensitivity of ultrasound may be increased using color flow doppler, small sized lesions can be missed. Thus, fetal MRI may be preferred in complicated cases [31]. The rate of liver herniation was 46.4% in the non-survival group while this rate was only 6.25% in the survival group. Our findings were consistent with the literature [3–6].
Assessment of fetal lung volume is one of the critical points in the prediction of neonatal survival. However, the optimum technique has not yet been developed [3–6]. Fetal lung volume may be assessed by two-dimensional ultrasonography, three-dimensional ultrasonography or fetal MRI [3–6]. The most commonly used parameters used for the assessment of fetal lung volume are LHR, o/e LHR and o/e TFLV [3–6]. Fetal lung area to head circumference ratio is an estimate of contralateral lung size and mediastinal shift at the level of the atria on transverse scan of the fetal thorax [33]. When LHR is greater than 1.4, the prognosis is generally good. If it is between 1.0 and 1.4, ECMO is often necessitated in the postnatal period. On the other hand, if LHR is 1.0 or less, the prognosis is poor. Furthermore, coexistence of liver herniation is associated with worse outcomes [33]. Additionally, the lower limit of LHR for neonatal survival has been a matter of debate in the last years. The lower limit of LHR for neonatal survival is decreasing with the results of current studies [3–6]. Lower LHR values were reported to be mostly associated with neonatal morbidity and increased rates of fetal interventions [3–6]. Median LHR values were 1.6 and 0.9 in the survival and non-survival groups respectively in this study. Moreover, a cut-off value of 1.05 was found by ROC curve analysis. These findings are consistent with the current literature [3–6]. Fetal lungs grow at a much higher rate than the fetal head circumference throughout gestation [34]. Thus, o/e LHR seems to be a more reliable parameter compared to LHR [3–6]. Values below 15% are associated with the worst outcomes and values above 45% are associated with favorable outcomes [3–6]. The median o/e LHR values were 48.5% and 20% in this study. Additionally, 22.5% was found to be the cut-off value for neonatal survivors according to ROC curve analysis. Observed/expected total fetal lung volume calculated by fetal MRI has high inter-observer agreement and positively correlates with LHR [32]. However, due to cost-effective issues we could not perform fetal MRI in any of the cases. On the other hand, we calculated TFLV using two-dimensional ultrasonography and calculated o/e TFLV according to established normograms [3–6]. Median o/e TFLV values were 50 and 20.5 in the survival and non-survival groups, respectively. Furthermore, a cut-off value of 23.5 was found by ROC curve analysis. These findings are consistent with the current literature [35]. In addition, estimation of fetal lung volume in pregnancies with CDH may also be used to identify fetuses that may benefit from fetal interventional procedures [13]. Fetal tracheal occlusion is the most widely used intrauterine intervention for the time being [13]. Obstruction of the fetal trachea leads to an increased transpulmonic pressure that results in large fluid-filled lungs during fetal lung development. Additionally, accelerated parenchymal lung growth was reported in normal and hypoplastic lungs [36]. However, FETO could not be performed in any of the cases due to the lack of technical devices.
Chromosomal anomalies were reported in 10 to 20 percent of prenatally identified cases; the most common of these were trisomies 18, 13 and 21 [1, 7]. An underlying syndrome is present in approximately 10 percent of CDH cases [1, 7]. Fetal karyotype analysis by amniocentesis was performed in eight cases (15.7%) and all were reported to have a normal karyotype. Additionally, there were two (3.9%) prenatally detected congenital structural abnormalities: one single umbilical artery and one limb-body wall complex. This low rate of chromosomal and structural abnormalities in this study was most probably due to the relatively small number of cases.
Optimal mode and gestational age for delivery is not certain in pregnancies with CDH. Elective induction of labor between 38 and 39 weeks of gestation is recommended so that pediatric surgery and neonatology services may be prepared to care for the neonate. There is no evidence that routine cesarean delivery is beneficial [37]. Survival and non-survival groups were comparable for median gestational week at birth, birth weight and mode of delivery. Median gestational week at birth was 38 for both groups. Median birthweight values were 2990 and 2935, respectively for the survival and non-survival groups. However, cesarean rates were 75% and 82.2%, respectively. These high rates were most probably related to the preference for cesarean sections by physicians in order to provide optimal care for the neonates.
Neonatal survival rate in pregnancies complicated with CDH has improved in the last decades due to advances in antenatal diagnosis and improvement of neonatal care [10]. Mortality rates still range between 30–50% depending on the severity of CDH and clinical characteristics of the patients [10]. The low rate of survival in this study was associated with several factors. First of all, FETO could not be performed in any of the cases. Secondly, most of the cases had poor prognostic factors such as right-sided lesion, liver herniation and low fetal lung volume. As our institution is a referral center, cases with unfavorable prognostic factors were mostly referred to our clinic for further management. Finally, only a small percent of the patients in the non-survival group could be operated. Although the efficacy of ECMO in infants with CDH was not demonstrated in randomized controlled studies, if available, ECMO should be considered for almost all neonates who cannot be managed with maximal conventional medical therapy, since they cannot survive without ECMO [1]. The overall rate of ECMO procedure was 22.7% in this study (37.5% in the survival group and 14.3% in the non-survival group).
The main strengths of this study were the relatively high number of parameters investigated, the single center experience and the homogeneity of cases in terms of obstetric characteristics. However, the main limitations were the retrospective design and the small number of cases, as well as the lack of MRI measurements for TFLV and FETO.
In conclusion, pregnancies with CDH should be managed at tertiary reference centers by a multidisciplinary approach. Earlier gestational week at diagnosis, right sided CDH, presence of liver herniation, supradiaphragmatic stomach position, lower LHR, o/e LHR and o/e TFLV were associated with decreased rates of neonatal survival. Physicians should be more cautious especially in cases with LHR, o/e LHR and o/e TFLV values below 1.05, 22.5 and 23.5, respectively.
Disclosures
The authors state that they have no conflict of interest. No funding was used for this study.
Footnotes
Acknowledgments
Special thanks to all the medical staff who work with devotion in order to provide optimal health-care to the patients in our institution.