
Abstract
OBJECTIVE:
To study whether there is an association between nutritional intake during the first week of life and severity of bronchopulmonary dysplasia (BPD) in extremely low birth weight (ELBW) infants.
METHODS:
In a retrospective cohort study, medical records of all ELBW infants admitted to our Neonatal Intensive Care Unit (2010–2017) were reviewed for infants’ demographics, clinical characteristics, nutritional intake during their first week of life, and BPD risk factors.
RESULTS:
During the study period 226 infants were identified of whom 67% (151/226) had moderate-severe BPD and the rest served as controls. Overall infants with moderate-severe BPD were younger, smaller, and spent more time on mechanical ventilation than their controls [(mean±standard deviation) 24.7±1.7 vs. 26.8±2.0 weeks gestational age (p < 0.001); 678±154 vs. 837±129 grams (p < 0.001); and 37.9±23.6 vs. 13.7±15.3 days (p < 0.001) respectively]. During the first week of life, the average caloric, carbohydrate, protein and lipid intakes were significantly lower, and the average fluid intake was significantly higher in the moderate-severe BPD than the control group. After adjustment for confounders, fluid intake, and days on mechanical ventilation were significantly associated with moderate-severe BPD with an odds ratio [OR (95% confidence interval)] of 1.03 (1.01–1.04), and 1.05 (1.03–1.07) respectively. Daily caloric intake was associated with an increased risk for moderate-severe BPD [OR: 0.94 (0.91–0.97)].
CONCLUSION:
Low caloric intake, and high fluid intake during the first week of life are associated with the severity of BPD in ELBW infants.
Introduction
Bronchopulmonary dysplasia (BPD) is common in extremely low birth weight (ELBW) infants. It is estimated that more than two-thirds of all ELBW infants are diagnosed with BPD at 36 weeks corrected gestational age (GA) [1]. The pathogenesis of BPD is multifactorial [2]. There are several genetic, antenatal and postnatal factors that are known to modulate lung’s maturation and its response to local and systemic inflammation, which are frequently associated with the diagnosis of BPD [3, 4]. Several risk factors associated with BPD have been well studied, whereas the role of others have not been well elucidated. For instance, the role of nutrition as a risk factor for the development of BPD has not been well investigated. Few nutritional elements have been proven to have a causative role in the prevention or treatment of BPD [5]; especially since the metabolism of glucose and fatty acids is important for essential cellular functions such as cellular differentiation, apoptosis and control of inflammation [6].
Nutrition plays a very important role in infants with BPD, since sick infants have high energy expenditures in order to compensate for their high metabolic demand and increased work of breathing [7]. Also, malnutrition affects lung’s growth, and early poor caloric intake is associated with the development of BPD [8]. It has been recently shown, that overall poor caloric intake during the first week of life is associated with poor growth in extremely preterm infants, until the age of two years [9]. Therefore, several attempts have been made to improve neonatal growth by improving caloric intake, mainly by improving amino acid intake to improve protein accretion. However, a recent meta-analysis has shown no difference in growth between infants who received early high protein supplementation (>3 g/kg in ≤24 hours of age) versus low and late protein supplementation (<3 g/kg in > 24 of age). It is believed that there is a threshold for protein supplementation, and when that threshold is attained, excessive protein intake does not translate into protein accretion [10]. In this study we sought to investigate whether there is an association between early caloric, individual macronutrients and fluid intake, and the development of BPD in ELBW infants.
Methods
In a retrospective cohort study, medical records of all infants who were admitted to our neonatal intensive care unit (NICU) at MetroHealth Medical Center, Cleveland, OH between 2010 and 2017, were reviewed. Our inclusion criteria consisted of all ELBW infants (<1000 grams) who were admitted to our NICU and exclusion criteria consisted of all ELBW who died during their first week of life and the ones who had congenital anomalies or suffered from moderate to severe hypoxic-ischemic encephalopathy.
Medical records were reviewed for infants’ demographics including their birth weight (BW), gestational age (GA), gender, ethnicity, mode of delivery, and Apgar scores at 1 and 5 minutes of life. Also, medical records were reviewed for infants’ clinical characteristics and risk factors associated with BPD including days of mechanical ventilation, postnatal steroids use, treatment of patent ductus arteriosus (PDA), air leak, sepsis, history of maternal chorioamnionitis and use of caffeine.
During the first week of life, medical records were reviewed for daily fluid intake (ml/kg/day), and caloric intake (kcal/kg/day). Also, medical records were reviewed for daily macronutrients intake including carbohydrate (grams/kg/day), protein (grams/kg/day), and lipid (grams/kg/day) intakes. When available, daily urine output (ml/kg/day), serum glucose (mg/dl), serum sodium (mEq/l), blood urea nitrogen (BUN, in mg/dl), and serum creatinine (mg/dl) levels were collected.
Mortality and morbidities of all infants were reviewed including death prior to discharge from the NICU, hospital length of stay, and average daily weight gain (grams). Infants’ anthropometric measurements at discharge were recorded including discharge weights (in grams), discharge lengths (in cm) and discharge head circumferences (in cm). Also, all anthropometric measurements were expressed in Z scores.
During the study period, and according to our NICU guidelines, all infants were nil per mouth (NPO) and on parenteral nutrition during their first week of life. BPD was defined according to the National Institute of Child Health and Human Development (NICHD) definition at 36 weeks corrected GA. Patients were classified according to the severity of their BPD; the study group consisted of infants with moderate and severe BPD and the rest (no BPD and mild BPD) served as controls. The study was approved by MetroHealth Medical Center institutional review board (IRB).
Statistical analysis
Data were expressed as means±standard deviations, and percentages, and continuous data were analyzed by independent samples t-tests and Mann Whitney U tests as appropriate. Categorical data were analyzed by Chi square test or Fisher exact test as appropriate. Odds ratio with 95% confidence interval were calculated. A general linear model (GLM) analysis was conducted to compare daily fluid, caloric and macronutrients intakes between the groups. Also, a GLM analysis was conducted to compare daily urine output, serum glucose, serum sodium, BUN and creatinine between the two groups. A backward logistic regression model was developed to adjust for potential confounders, with moderate to severe BPD as the dependent variable, and risk factors associated with BPD (and found to be statistically significantly different in a bivariate analysis) as independent variables. A p value of <0.05 was considered statistically significant.
Results
During the study period (2010 and 2017) 24,090 infants were born at MetroHealth Medical Center of whom 264 ELBW were admitted to the NICU and 226 infants met our inclusion criteria.
Patients’ demographics are summarized in Table 1. Sixty-seven percent (151/226) of infants developed moderate to severe BPD. Infants with moderate to severe BPD were smaller, and younger than their controls. Also, they had lower Apgar scores at 1 and 5 min of life than their counterparts. Also, patients’ clinical characteristics and risk factors for BPD are summarized in Table 1. There were significant differences between the two groups. Infants with moderate to severe BPD had more days of mechanical ventilation, and postnatal steroids. Also, they had more surgical ligation of their PDA and a higher rate of pneumothoraces than their controls. Patients with moderate to severe BPD had a higher rate of sepsis than their controls.
Patients’ demographics, clinical characteristics and risk factors for BPD
Patients’ demographics, clinical characteristics and risk factors for BPD
The daily fluid intake and caloric intake during the first week of life are summarized in Fig. 1 A&B. There was a significant difference in fluid intake between the two groups. Infants with moderate to severe BPD had a larger amount of daily fluid intake than their controls as shown in Fig. 1A (General linear model, p < 0.001). Also, there was a significant difference in caloric intake between the groups. Infants with moderate to severe BPD received a smaller amount of daily caloric intake than their controls as shown in Fig. 1B (General linear model: P < 0.001).
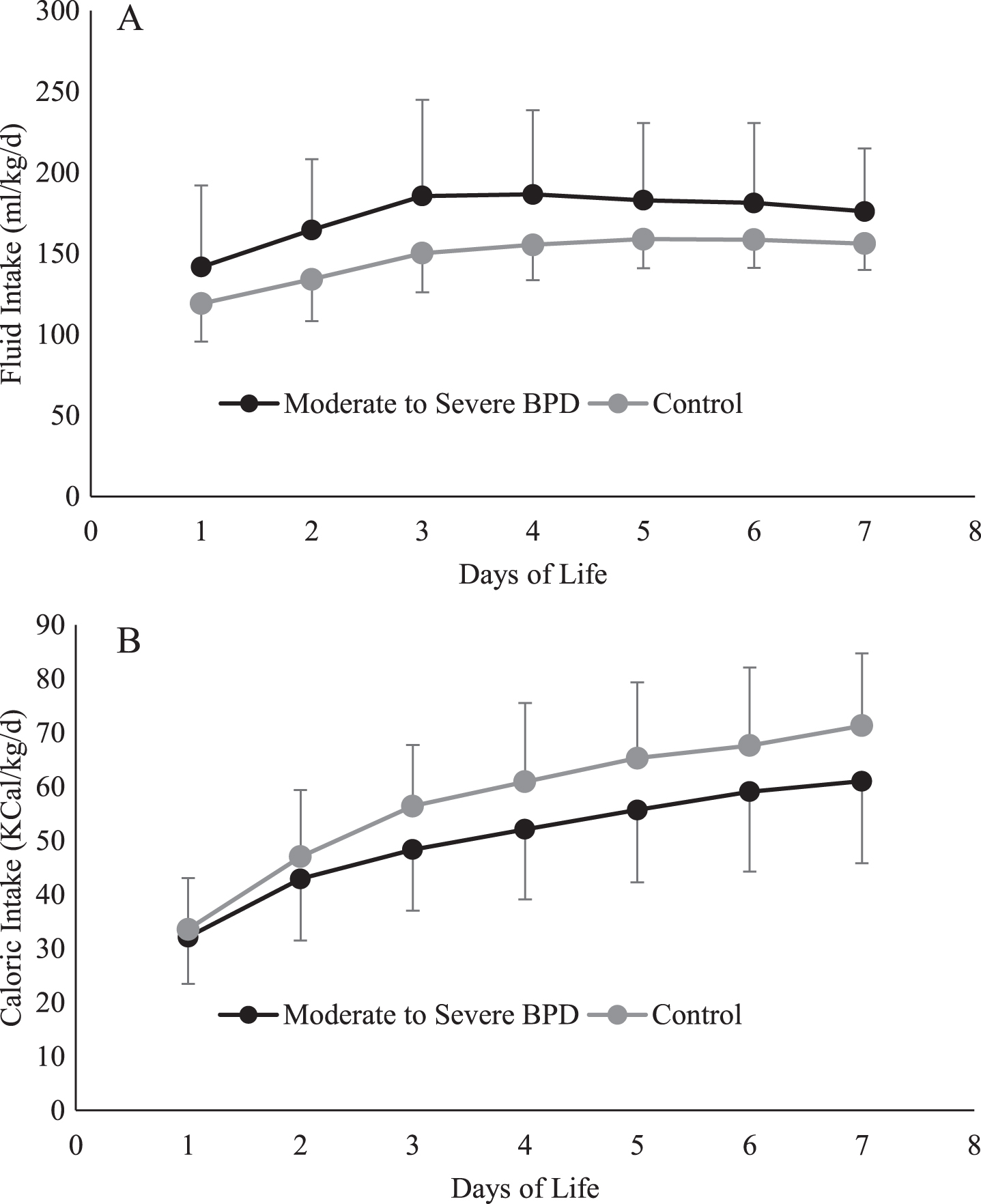
The daily fluid intake (1A) and daily caloric intake (1B) during the first week of life. Infants with moderate to severe BPD had a larger amount of daily fluid intake than their controls (p < 0.001). Infants with moderate to severe BPD received a smaller amount of daily caloric intake than their controls (P < 0.001).
The daily carbohydrate, protein, and lipid intakes during the first week of life are summarized in Fig. 2. There was a significant difference in the amount of daily carbohydrate, protein and lipid intakes between the groups. Infants with moderate to severe BPD had a smaller amount of daily macronutrient intakes than their controls over the span of their first week of life (Fig. 2A, 2B, and 2 C; General linear model with p values < 0.001 for all macronutrients).
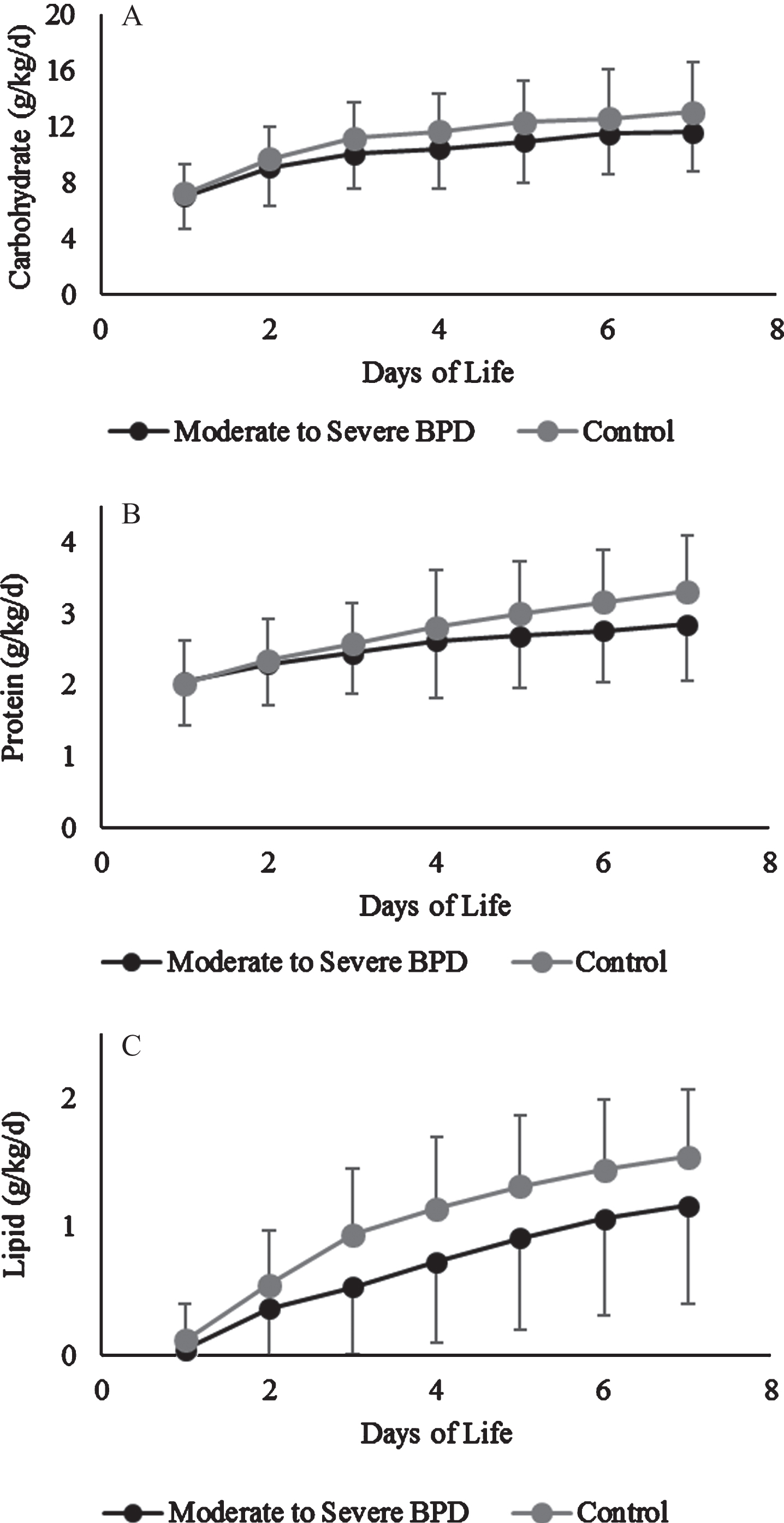
The daily carbohydrate (2A), protein (2B), and lipid (2C) intakes during the first week of life. Infants with moderate to severe BPD had a smaller amount of daily macronutrient intakes than their controls (p < 0.001 for all macronutrients).
To determine if the supply of macronutrients intake was limited by infants’ intolerance of glucose and protein intake, daily serum glucose, BUN and serum creatinine levels were studied. There was a significant difference between the two groups. Infants with moderate to severe BPD had a higher daily serum glucose and BUN, but there were no differences in daily serum creatinine levels. Infants, with moderate to severe BPD, had a higher serum glucose levels than their controls between day one and seven of life. Serum glucose varied between 133±76 mg/dl on day one and 119±69 mg/dl on day seven of life in infants with moderate to severe BPD vs. 107±54 mg/dl on day one and 107±41 mg/dl on day seven in the control group (GLM; p = 0.06). Also, infants, with moderate to severe BPD, had higher BUN levels than their controls between day one and seven of life. BUN varied between 13.5±4.3 mg/dl on day one and 29.8±15.2 mg/dl on day seven of life in infants with moderate to severe BPD vs. 14.5±6.0 mg/dl on day one and 23.9±11.9 mg/dl on day seven in the control group (GLM; p = 0.04). Between day one and seven of life, infants with moderate to severe BPD, did not have any differences in daily serum creatinine levels than their controls. Serum creatinine levels varied between 0.77±0.17 mg/dl on day one and 0.95±0.26 mg/dl on day seven of life in infants with moderate to severe BPD vs. 0.86±0.25 mg/dl on day one and 0.86±0.28 mg/dl on day seven in the control group (GLM; p = 0.91).
To determine if the fluid intake was affected by infants’ urine output and serum sodium, daily urine output and serum sodium were obtained. Infants with moderate to severe BPD had a higher daily urine output, and serum sodium than their controls. The average daily urine output varied between 3.3±1.6 ml/kg/hour on day one and 4.8±1.9 ml/kg/hour on day seven of life in infants with moderate to severe BPD vs. 3.8±1.8 ml/kg/ hour on day one and 3.6±1.2 ml/kg/hour on day seven in the control group (GLM; p < 0.001). Also, infants, with moderate to severe BPD, had higher serum sodium levels than their controls between day one and seven of life. Serum sodium varied between 140±5 mEq/l on day one and 137±5 mEq/l on day seven of life in infants with moderate to severe BPD vs. 137±3 mEq/l on day one and 137±3 mEq/l on day seven in the control group (GLM; p = 0.03).
The average macronutrients, caloric and fluid intake during the first week of life are summarized in Table 2. Infants with moderate to severe BPD had higher intake of fluids and a lower caloric and macronutrients’ intakes than their controls.
Average macronutrients, caloric and fluid intake during the first week of life
To adjust for potential confounders, a binary, backward logistic regression model was developed with BPD as the dependent variable and GA, days of mechanical ventilation, PDA surgical repair, pneumothorax, sepsis, daily fluid intake, and daily caloric intake as independent variables. After adjustment for the aforementioned risk factors, daily fluid intake, daily caloric intake during the first week of life, and duration of mechanical ventilation were the only independent risk factors that were retained and were associated with the severity of BPD (Table 3).
Adjusted Odds ratio of risk factors associated with bronchopulmonary dysplasia
We have shown that early nutrition and fluid intake, as early as the first week of life, is associated with the severity of BPD in ELBW infants. Early low caloric intake is associated with the severity of lung disease at 36 weeks corrected GA. Also, we have shown that excessive fluid intake as early as the first week of life is associated with the severity of BPD in ELBW infants.
The pathogenesis of BPD is multifactorial, which makes it challenging to come up with a simplified approach to its management. Several studies have shown that smaller, younger, growth-restricted infants are at risk for BPD, as well as infants with low Apgar scores are at risk for death or BPD [1, 12]. Our findings, in ELBW infants, are consistent with the literature. In our study, infants with moderate to severe BPD were smaller, younger and had low Apgar scores at birth than controls. Likewise, mechanical ventilation, oxygen toxicity and sepsis are well known risk factors associated with BPD [13, 14]. In our study, patients with moderate to severe BPD spent more times on mechanical ventilation and had a higher rate of sepsis than controls. Surgical ligation of PDA and presence of pneumothoraces are two risk factors associated with BPD [15, 16], and our study infants with moderate to severe BPD had a higher rate of PDA surgical ligation and a higher rate of air leaks than their controls. The association between chorioamnionitis and BPD remains inconclusive [17, 18], and in our study we did not find a statistically significant difference in chorioamnionitis between infants with moderate to severe BPD and their controls. Our results could be due to the smaller size of our cohort (our study might have been underpowered to show any differences), or because the rate of chorioamnionitis is elevated at baseline among ELBW infants.
It has been previously shown that increased fluid intake is associated with BPD [19, 20] and in our study, infants with moderate to severe BPD had a higher fluid intake than their counterparts. To determine if the higher fluid intake in our patients with moderate to severe BPD was related to a decrease in urinary output, and as a result the increase in fluid intake was necessary to avoid acute kidney injury, we measured daily urinary output and serum creatinine during the first week of life. We found that infants with higher fluid intake had a higher urinary output and we did not find any statistically significant differences in daily serum creatinine between the two groups. Our findings suggest that infants with moderate to severe BPD did not require an increase in fluid intake to compensate for a low urinary output or impaired renal function. This may be related to lower expression of mineralocorticoid receptors in ELBW neonates leading to excessive renal fluid loss besides excessive trans-epidermal losses [21] or lower expression of Aquaporin 1 and 9 at lower gestational ages [22, 23].
Adequate nutrition is essential to promote lung and somatic growth. In premature infants, critical illness during the first week of life is associated with significant morbidity, which is mediated by their early caloric intake. In a study of 1,366 extremely premature infants, more critically ill infants (requiring mechanical ventilation for seven days at birth), had a lower caloric intake, and more moderate to severe BPD then the less critically ill infants [24]. In another study of 296 infants who were less than 27 weeks GA, an early increase in energy and protein intake was associated with a lower risk of BPD in infants who were mechanically ventilated for more than 10 days [25] but a recent meta-analysis to investigate this association found 12 studies which addressed this issue but no randomized controlled trials were found that examined the effects of increased versus standard energy intake for preterm infants with (or developing) chronic lung disease (CLD)/BPD [26]. In our study, patients with moderate to severe BPD had a lower caloric and protein intake during their first week of life than their controls, thus there is a need to conduct randomized trials to answer this important question and provide guidance for management of these infants.
To determine if any of the macronutrients are responsible for the poor caloric intake in infants with moderate to severe BPD, we analyzed the daily intake of each of the macronutrients during infants’ first week of life. We found that infants with moderate to severe BPD had a lower daily glucose, protein and lipid intake than their controls. Therefore, to determine if the intake of each macronutrient was associated with the infants’ intolerance to the supplementation of the macronutrient in question, we monitored daily serum glucose and BUN. We found a significant difference between the two groups. Infants with moderate to severe BPD had a higher daily serum glucose and BUN. Our findings suggest that the lack of supplementation of glucose and protein might have been limited by the infants’ intolerance to a higher amount of glucose and protein supplementation. For instance, the body composition of a one kg preterm infant is 1% fat and 8.5% protein, and the non-protein caloric reserve is only 110 kcal/kg [27]. Since fatty acid oxidation is generally impaired in ELBW infants, in case of energy failure, protein catabolism is necessary for gluconeogenesis and energy production, which is largely mediated by several factors including cytokines, glucocorticoids and catecholamine release [28]. Also, ELBW infants often grow in a suboptimal environment, in a noisy NICU where stress, pain, and altered sleep pattern may negatively impact their growth and development. Chronic inflammation which is frequently observed in ELBW infants developing BPD affects growth through suppression of insulin like growth factor IGF-1 [29]. Hyperglycemia is mostly explained by poor endogenous insulin production or poor IGF-1 function [22, 31]. Therefore, multiple stressors and metabolic derangements of ELBW infants might have been responsible for the inability to provide adequate caloric and macronutrients intake to these critically ill infants.
Early nutrition provided to ELBW infants has been compromised often by several factors such as the severity of illness, the fear of NEC or intolerance to certain macronutrients such as glucose and protein. Despite implementing of nutritional protocols in most NICUs, most infants continue to receive suboptimal nutrition. In a prospective study of 353 VLBW infants, 34% of all infants did not meet their protein intake goals (3.5 g/kg/day), and 71% of all infants did not meet their caloric intake goals (90 kcal/kg/d) by the end of their first week of life [32]. In another large multicenter study of 1,187 ELBW infants, most infants did not receive their recommended amounts of glucose and caloric intake during their first week of life [33].
Infants with moderate to severe BPD had a lower fat intake than their controls. Unfortunately, we did not have triglyceride levels available to review the tolerance to lipid intake, and to determine if the limitation of lipid supplementation was limited by hypertriglyceridemia and fat intolerance.
It has been shown that the combination of high amino acid and energy intake increases the proportion of phenylalanine used for protein accretion through phenylalanine hydroxylation [34]; and BUN levels reflect other factors than protein intake, such as renal function, acuity of illness, liver function and hydration status. High BUN and serum creatinine are mostly secondary to kidneys’ dysfunction of prematurity rather than protein intolerance [35]. Balakrishnan et al in a study evaluating the effect of protein intake on BUN in VLBW infants has shown that BUN increases by 8.9 mg/dl/day independently from the amount of protein intake, and that BUN increases by 1.2 mg/dl for each g/kg of protein intake [36]. The findings of several studies support the fact that preterm infants have high protein turnover rate secondary to active catabolism. Protein breakdown needs to be combined with high protein synthesis rate to support the demand and replace the deficit. Protein synthesis is an active energy consuming process, thus sufficient amino acids and energy should be available to optimize the process [34]. Protein is an important energy source in the fetus consequently an elevated BUN levels after premature birth may reflect an acceptable generation of a byproduct material rather than protein intolerance. Thureen el al found no correlation between the amount of protein intake and the level of BUN [30]. In our study, infants with moderate to severe BPD received less amount of protein then their controls, and they had higher serum BUN levels than their controls. Since our study is a retrospective study, it is difficult to determine if the level of BUN was the deterrent for increasing the amount of protein intake.
To adjust for potential confounders seen in our study, a logistic regression analysis was conducted with moderate to severe BPD as the dependent variable and GA, days of mechanical ventilation, PDA surgical repair, pneumothorax, sepsis, daily fluid intake, and daily caloric intake as independent variables. After adjustment for other risk factors, daily fluid and caloric intake during the first week of life and duration of mechanical ventilation were the only independent risk factors that were associated with the severity of BPD.
Our study has limitations; it is a single center retrospective study and it was difficult to determine the deterrents that prevented treating physicians from increasing the total amount of caloric intake, and individual macronutrients intake. Also, it was difficult to determine the deterrents that prevented the treating physicians from restricting the amount of total fluid intake. Future randomized controlled studies are needed to determine the optimal fluid, caloric and macronutrient intakes to improve the short and long-term morbidity of surviving extremely preterm infants.
The main strength of our study, is that all patients were exclusively parenterally fed during their first week of life. Therefore, it was possible to accurately calculate the amount of total fluids, total caloric, and macronutrients’ intakes. If infants were to be enterally and parenterally fed, the calculations of different intakes would have been affected by gastro-intestinal absorption, and our calculations would have been an estimate at best. Also, our findings emphasize the importance of nutrition, as early as the first week of life, to prevent the development of severe BPD.
In conclusion, we have shown that early low caloric and high fluid intakes are associated with the severity of BPD at 36 weeks corrected GA.
Funding and conflict of interests
None.