
Abstract
BACKGROUND:
Dengue fever is a mosquito-borne viral illness with 100 million new cases occurring worldwide. The vectors involved are mainly Aedes aegypti and Aedes albopictus. Dengue infection is associated with maternal as well as fetal morbidities, like stillbirth, preterm birth, and low birth weight.
THE CASE:
We report a case of dengue fever occurring during early pregnancy and subsequent congenital neurologic malformation in the neonate as a result of vertical transmission. To our knowledge, this is the first case of confirmed congenital dengue in Saudi Arabia.
DISCUSSION:
Dengue infection is not commonly associated with congenital anomalies and no biologic mechanism has yet been established for its teratogenicity. Congenital dengue in neonates can be confirmed by identification of the dengue virus in cord blood samples. The positive dengue serology within the first week of life, together with the confirmed maternal dengue infection during pregnancy, supports the diagnosis of vertical transmission in the presence of clinical manifestations. A high index of suspicion, early diagnosis, and close monitoring is needed in these cases.
Background
Dengue fever is a mosquito-borne viral illness with 100 million new cases occurring worldwide. The vectors involved are mainly Aedes aegypti and Aedes albopictus [1]. Dengue fever was first detected in the city of Jeddah in 1994, and A. aegypti was implicated as the cause. After a large outbreak of dengue in the city of Mecca in 2009, the disease became endemic in that city [2]. The case fatality rate reported by the Ministry of Health in 2009 was 4.6% [2]. Dengue infection is associated with maternal as well as fetal morbidities, like stillbirth, preterm birth, and low birth weight [3].
We report a case of dengue fever occurring during early pregnancy and subsequent congenital neurologic malformation in the neonate as a result of vertical transmission. To our knowledge, this is the first case of confirmed congenital dengue in Saudi Arabia.
The case
A 33-year-old Saudi female, gravida 3, para 2, with 2 healthy living children, presented at our hospital emergency room at 13 + 2 weeks of gestation with a history of fever, headache, body pain, and nausea. She had no petechiae or history of bleeding. Her blood smear showed mild thrombocytopenia, and her dengue serology was positive for both the NS 1 antigen and dengue IgM, although the IgG was negative. She improved with conservative management provided as outpatient care. Her initial antenatal ultrasound at 22 weeks was normal (Fig. 1), but a follow-up scan at 29 + 3 weeks of gestation showed fetal brain anomalies in the form of microcephaly, with the fetal head circumference below 1% for its gestational age (Fig. 2). Magnetic resonance imaging (MRI) of the fetus conducted at 29 weeks demonstrated extensive loss of cerebral parenchyma volume and loss of the normal architecture of the cerebral hemispheres; these were replaced by large cysts. The proposed differential diagnoses at that time were congenital infections or fetal cerebral ischemic insults (Fig. 3). The patient went into labor at 37 + 3 weeks and delivered a vigorous baby girl with a good Apgar score. The infant’s birth weight was 2.47 kg (10th centile), her height was 47 cm (50th centile), and her head circumference was 27 cm (<3rd centile for her age) (Fig. 4). She showed no dysmorphic features. The infant was admitted to the neonatal intensive care unit for further care and workup, where she remained hemodynamically stable, euglycemic, and was feeding well orally. Her routine laboratory investigations were normal. Serology for dengue was positive (both IgM and IgG) and the Zika virus PCR was negative. A skeletal survey showed apparent microcephaly with a fusion segmentation anomaly of the lumbar vertebrae. Her abdominal ultrasound was normal. A brain MRI scan showed a significant reduction in the brain volume, ventriculomegaly with marked cystic changes, and a small dystrophic calcification at the junction of the cortical and subcortical areas at the periventricular regions, together with diffuse cerebellar hypoplasia (Fig. 5).

Ultrasound scan shows no normal head at gestational age 22 weeks + 3days.
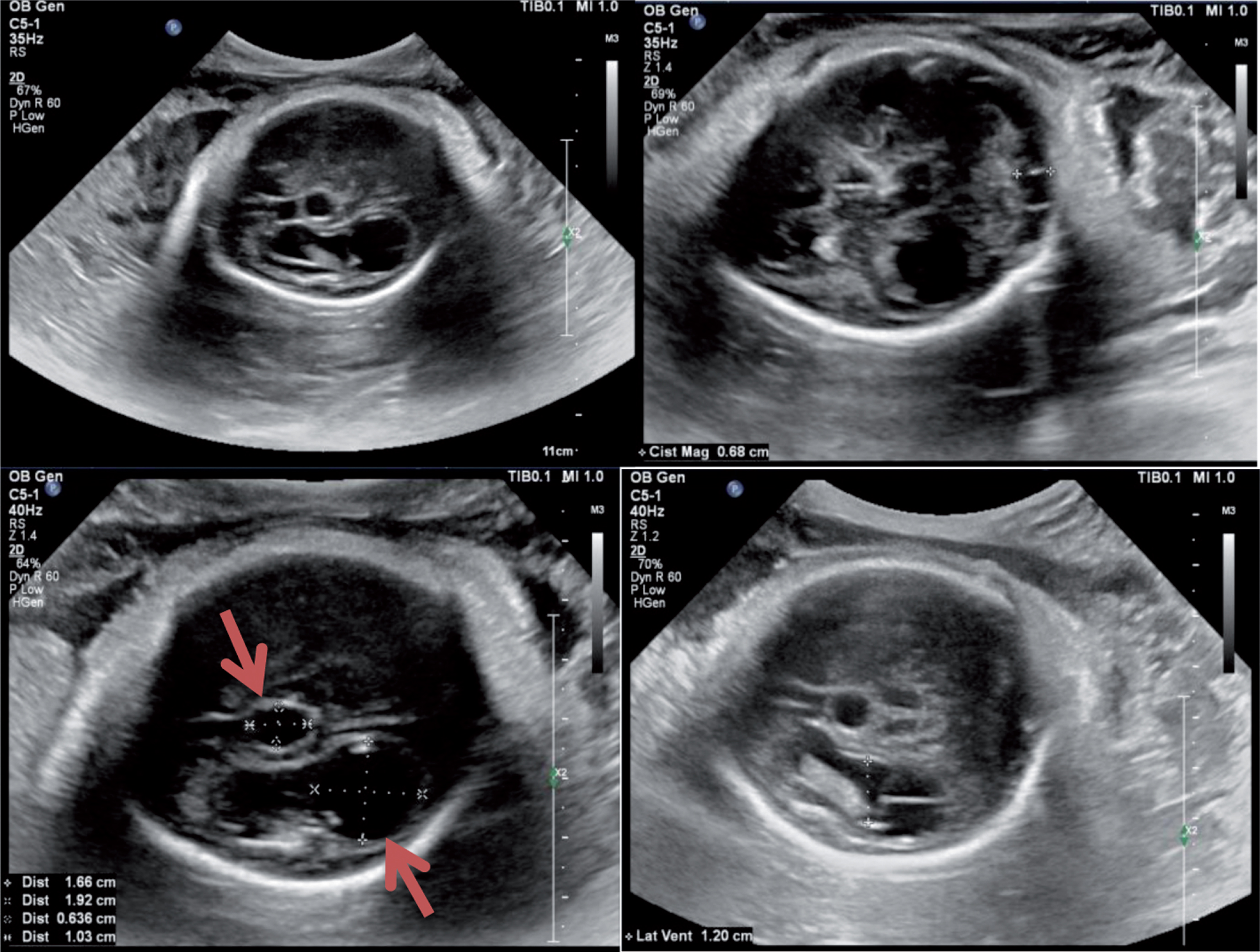
Follow-up ultrasound scan at gestational age 29 weeks + 3days shows fetal brain anomalies in the form of microcephaly, with the biparietal diameter (BPD) and head circumference (HC) below 1% for gestational age, a lemon-shaped skull, and a midline cyst and right cerebral cyst (arrows) posterior to the lateral ventricle.
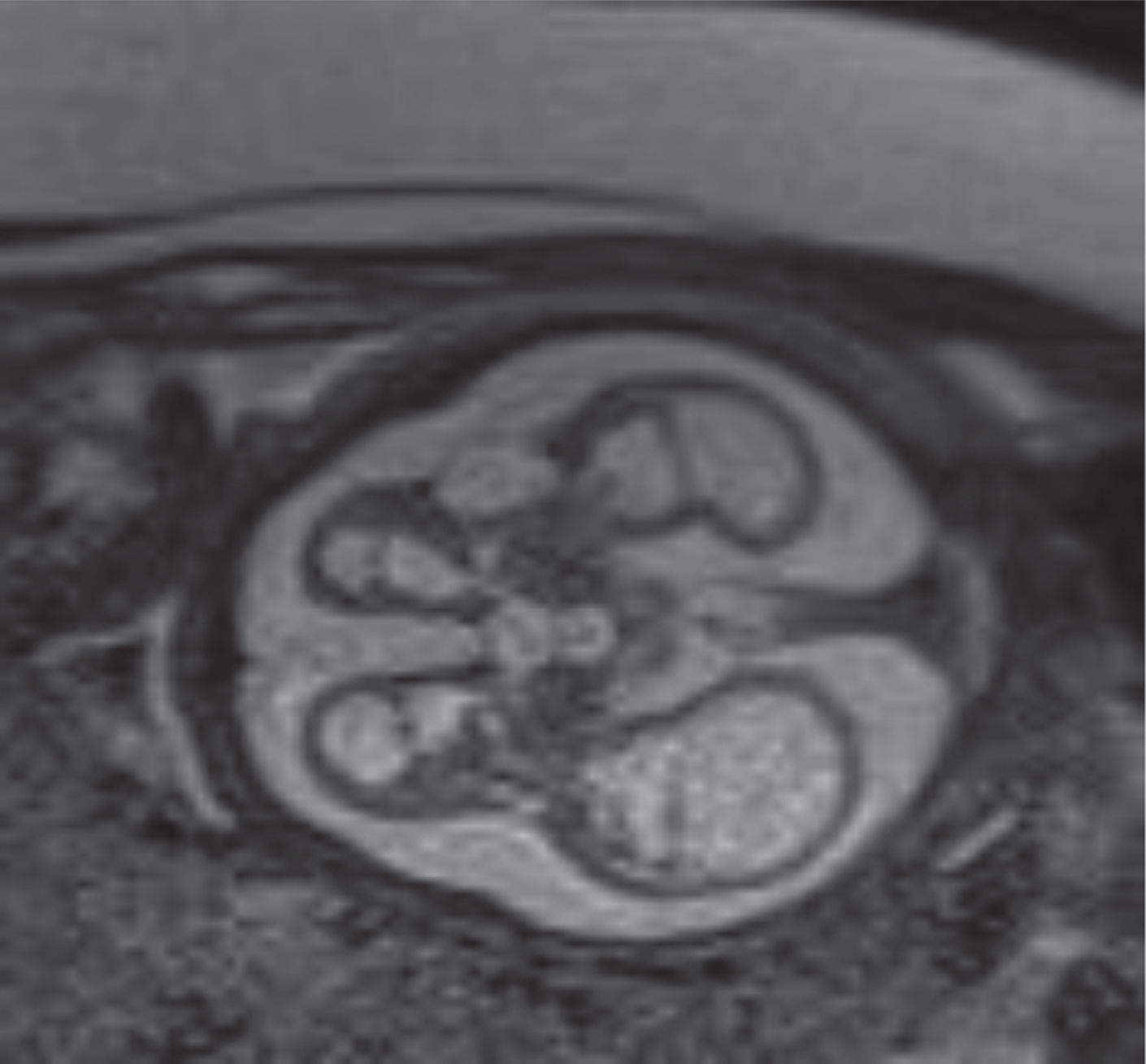
Magnetic resonance imaging performed at gestational age 29 weeks + 6 days. A selected T2 weighted image in the axial plane of the fetal head demonstrates an extensive loss of cerebral parenchyma volume and a loss of the normal architecture of the cerebral hemispheres, which are replaced by large cysts as well as by the formation of subcortical cysts. Marked ventricular dilatation is identified by the large extra-axial spaces.

At birth: Severe microcephaly (head circumference 29 cm) with no other dysmorphic features.
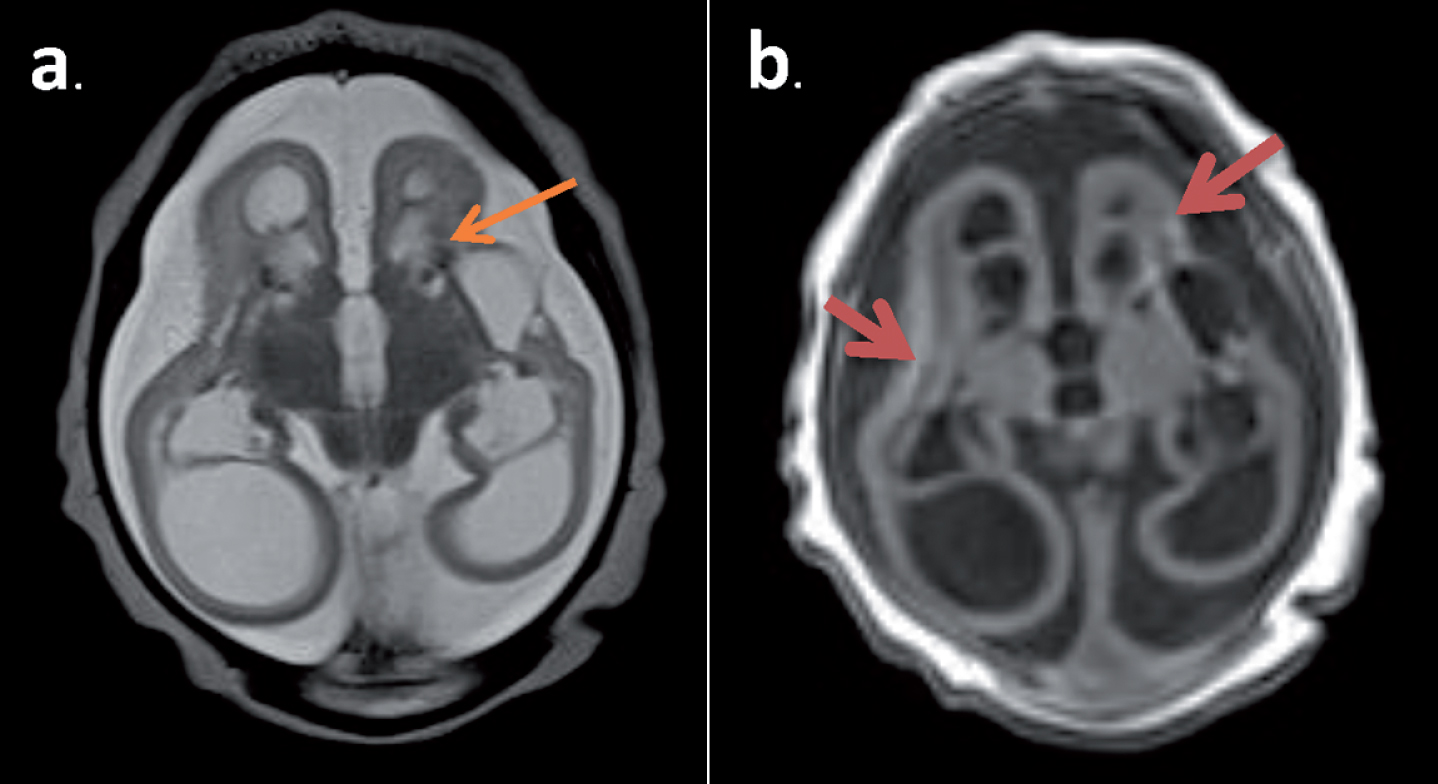
Magnetic resonance imaging performed on the neonate’s brain on the 8th day of life. Two selected images in the axial planes are shown: a. T2 weighted and b. T1 weighted image. The imaging demonstrates the marked reduction in the volume of the supratentorial brain. Significant thinning of the cortex and loss of the normal architecture with marked cystic changes are seen at the bilateral cerebral hemispheres. Also identified is the loss of normal architecture with the presence of small dystrophic calcification at the junction of the cortical and subcortical areas of the frontal lobes and periventricular regions (arrows). Associated ventriculomegaly is identified, with enlargement of the subarachnoid spaces.
The baby was discharged home in stable condition in the second week of life on regular breast feeding and cholecalciferol drops. At her outpatient follow up at one month of age, she was thriving well except for the microcephaly (head circumference of 29 cm). She had mild hypertonia of her limbs and a history of abnormal movement on and off, lasting for a few seconds and then self-aborted. She was therefore referred to the neurology and physiotherapy team and was given follow-up appointments.
Dengue fever is an acute febrile illness caused by dengue viruses (DENV-1, DENV-2, DENV-3, DENV-4) belonging to the Flaviviridae family. The virus is transmitted to humans through the bites of infected mosquitoes. The incubation period in the human body is 4–10 days. Dengue fever shares the same vectors as Zika, namely A. aegypti and A. albopictus. The incidence of dengue has increased 30-fold over the last 50 years. As many as 50–100 million infections are now estimated to occur annually in over 100 endemic countries [1]. In Saudi Arabia, dengue is mainly found in the Mecca, Madinah, and Jizan regions [2]. Our patient came from the Mecca region.
Dengue infection is not commonly associated with congenital anomalies and no biologic mechanism has yet been established for its teratogenicity. However, it causes increased production of pro-inflammatory cytokines, including interleukins 6 and 8, and tumor necrosis factor-α. These cytokines affect the uterus, causing its stimulation and the activation of proteins that lead to preterm labor. Thrombocytopenia, plasma leakage, or bleeding tendency could result in damage to the placental circulation, with subsequent fetal consequences like stillbirth and vertical infection [3]. A systematic review published in 2016, which included observational studies and case reports, evaluated the association between dengue infection during pregnancy and the risk of adverse fetal outcomes in 6,071 pregnant women. Analysis of four studies showed an association between dengue infection and an increased risk of preterm birth (OR 2.5, 95% CI 1.44–4.34), while analysis of three studies showed an increased risk of low birth weight or intrauterine growth restriction (OR 1.84, 95% CI 1.04–3.25) [4]. Another review published in 2018 showed that symptomatic dengue fever during pregnancy could lead to congenital neurological manifestations, including microcephaly, anencephaly, and hydrocephalus, in the newborn [5]. Congenital dengue in neonates can be confirmed by identification of the dengue virus in cord blood samples. Although this identification was not performed in our case, the positive dengue serology within the first week of life, together with the confirmed maternal dengue infection during pregnancy, supports the diagnosis of vertical transmission in the presence of clinical manifestations [6].
In summary, the association between symptomatic dengue during pregnancy and congenital anomalies of the brain in the infant, while not having as high a frequency as the linkage observed for Zika virus, opens up the possibility that other flaviviruses can cause congenital malformations and raises questions about policy implications. A high index of suspicion, early diagnosis, and close monitoring is needed in these cases. The health authority needs to collaborate in the design and monitoring of control and prevention strategies for this infection in the susceptible population.
Disclosure statements
Funding Source: No funding was secured for this study.
Financial Disclosure: The authors have no financial relationships relevant to this article to disclose.
Conflict of interest
The authors have no conflicts of interest to disclose.