
Abstract
BACKGROUND AND OBJECTIVES:
Early onset sepsis (EOS) is an important cause of neonatal morbidity and mortality. Timely administration of antibiotics is crucial in management. We initiated a quality improvement project to improve timely administration of antibiotics.
METHODS:
Primary drivers of change identified by the team were improving delivery of antibiotics from pharmacy and improving time to admit in the electronic medical record (EMR) in order to improve overall timeliness of antibiotics administration. Timings of antibiotics administration was tracked by using a control chart. Timings of antibiotics and outcomes of pre-intervention (December 2016) were compared with post intervention of PDSA cycles (January 2017–November 2018).
RESULTS:
There was statistically significant improvement in time to admission in electronic medical records over the time periods of pre-intervention, PDSA I and PDSA II (p-value < 0.05) (Table 1). Also, time to delivery of antibiotics from pharmacy was significantly reduced between PDSA cycles from 21 minutes to 9 minutes with improvement in overall workflow. An average time to infusion of antibiotics decreased from 70 minutes to 48 minutes. There was also overall improvement in number of neonates receiving antibiotics under 1 hour of decision making from 37% to 77%.
CONCLUSIONS:
In our study we were able to successfully implement our “antibiotics under one hour” goal. The ability to achieve this objective can be met across multi-institutions rendering care to newborns if the approach is multidisciplinary. Deleting obstructions in the process that involve admission, registration and entry into the EMR effectively reduced time.
Abbreviations
Early onset sepsis National institute for Health and Care Excellence Electronic medical record Neonatal intensive care unit Plan-do-study-act El Paso Children’s Hospital
Introduction
Neonatal sepsis is an important cause of neonatal mortality and morbidity. Early onset sepsis is defined as a blood or cerebrospinal fluid (CSF) culture obtained within 72 hours after birth growing pathogenic bacterial species [1]. Infants with EOS typically present with symptoms soon after their birth. EOS is usually due to vertical transmission by ascending contaminated amniotic fluid or during vaginal delivery [2]. There are multiple risk factors associated with increased likelihood of neonatal infection but most common are maternal chorioamnionitis and maternal GBS colonization [3, 4]. Overall incidence of EOS in term neonates defined as positive growth of bacteria is 0.57 to 0.98 per 1000 live births per different prospective population studies [5]. National institute for Health and Care Excellence (NICE) suggests infusion of antibiotics within one hour of decision, also known as “the golden hour” [6]. Management of early sepsis involves supportive care and more importantly timely administration of antibiotics [2]. While administration of antibiotics as quickly as possible makes sense, administration of antibiotics within one hour is often hard to achieve due to various barriers [7, 8]. The 2008 international guidelines also recommend administration of antibiotics within 1 hour of suspicion of sepsis [9]. Most neonatologists agree that antibiotics should be administrated promptly to neonates with suspected EOS. Literature in neonates is lacking, however adult studies do show that patients with sepsis are at high risk of progression and delay in antibiotics administration is linked with poor survival [8, 10].
Golden hour initiative at our facility was kick started to standardize admission process and as part of the project we formulated a prospective quality improvement project to investigate and improve timing of antibiotic infusion in neonates admitted with Suspected EOS. We identified barriers and designed interventions to improve timeliness of antibiotics administration. Our primary objective was to decrease antibiotics administration to under one hour from decision time in 75% of neonates admitted with suspected EOS within a 6 months period. Our secondary objective was to assess the effect of timing of antibiotics administration on short term health related outcomes of neonates admitted with Suspected EOS.
Methods
Site and duration of study
This study was conducted at El Paso Children’s Hospital(EPCH) affiliated with Paul L. Foster School of Medicine, Texas Tech University Health Sciences Center El Paso, Texas. EPCH is a free-standing children hospital in El Paso, Texas. However, it does share one floor with a sister adult hospital facility named University Medical Center (UMC) which harbors labor and delivery (L&D) unit. UMC is a health system with over 6000 deliveries per year. The neonatal intensive care unit (NICU) at EPCH is a state designated level IV NICU unit with over 700 admissions per year. However, as a likely result of falling birth rates nationwide and other factors, we experienced declining number of admissions during the study period as shown in results section. Care of neonates is undertaken by two teams, which include an attending neonatologist, resident physicians, neonatal nurse practitioners (NNPs) and advance care registered nurses. This study was conducted between December 2016 and November 2018.
Primary drivers of change identified by the team were improving delivery of antibiotics from pharmacy and improving time to admit in the electronic medical record (EMR) in order to improve overall timeliness of antibiotics administration (Fig. 2).
Subjects
All neonates admitted to the NICU qualified for study. There was a total of 469 neonates admitted to NICU with a diagnosis of suspected EOS and received antibiotics during the study cycle. For the purpose of this study EOS was defined as an infection occurring within 72 hours of birth. Decision to start antibiotics was based newborn’s clinical condition supplemented by prenatal events and maternal risk factors.
QI activities: Pre-intervention and plan-do-study-act activity I (December 2016-September 2017)
In the first phase of the study, an audit of antibiotics administration timing was done which included reviewing charts of 29 neonates admitted to the neonatal intensive care unit (NICU) in the month of December 2016. We found only 37% of the neonates admitted with EOS were receiving antibiotics under one hour after decision to treat was made. This data was presented and an interdisciplinary team was formed which included medical director, nursing supervisor, pharmacist manager and hospital administration liaisons. This interdisciplinary team investigated perceived barriers to timely antibiotics administration (Fig. 1). After identification of area of improvement and initial data analysis was completed, the team proposed that antibiotics administration could be improved. The primary objective was to decrease the time to administer antibiotics to less than 1 hour over a period of 6 months. Initial interventions also included thorough record keeping at each step, policy changes, and staff education was provided with in-services, staff meetings and emails. Multiple lectures and presentations were done to bring to the attention of as many staff as possible. All NICU pediatric residents received a small presentation before each month’s orientation.
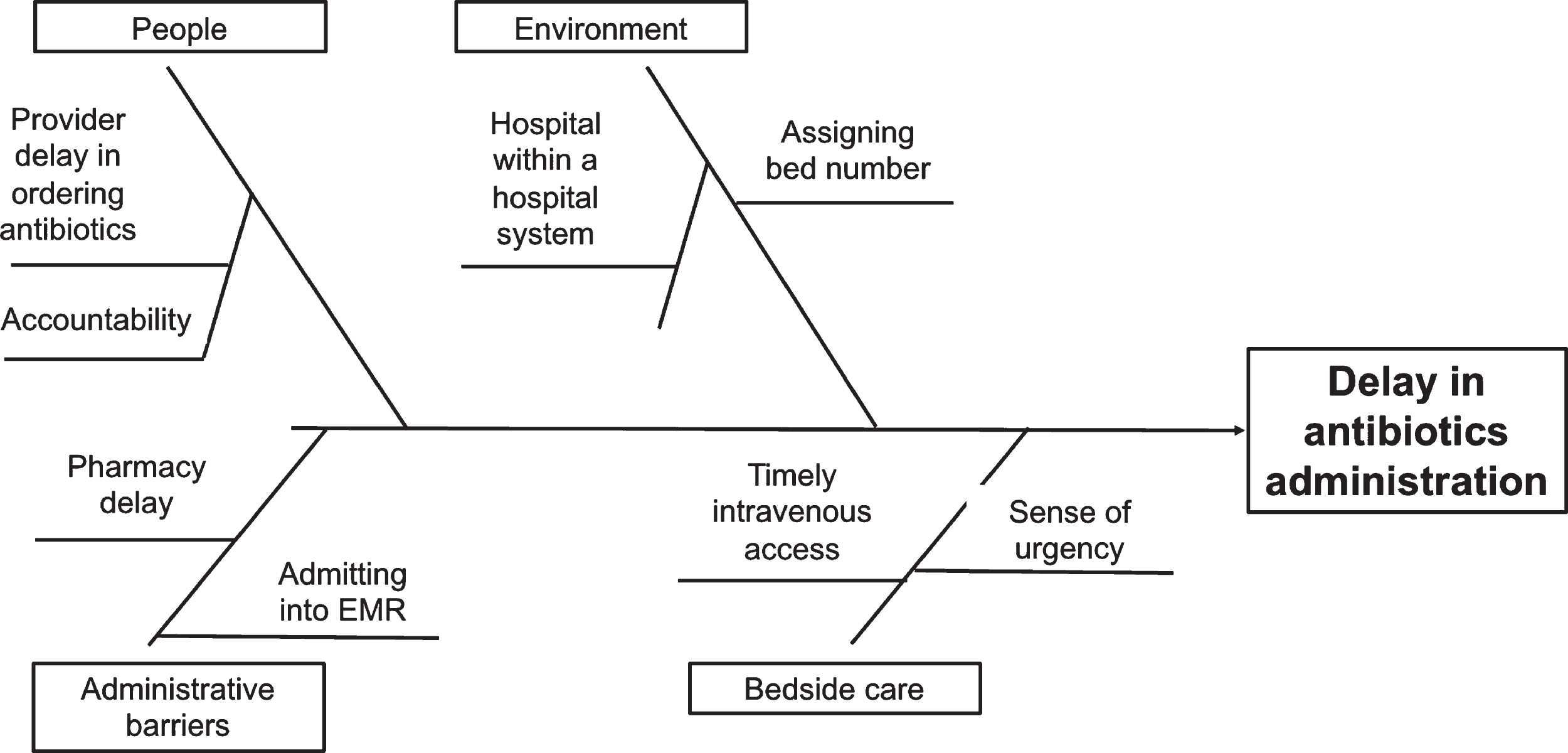
Fishbone diagram for causes in delay in antibiotics administration.
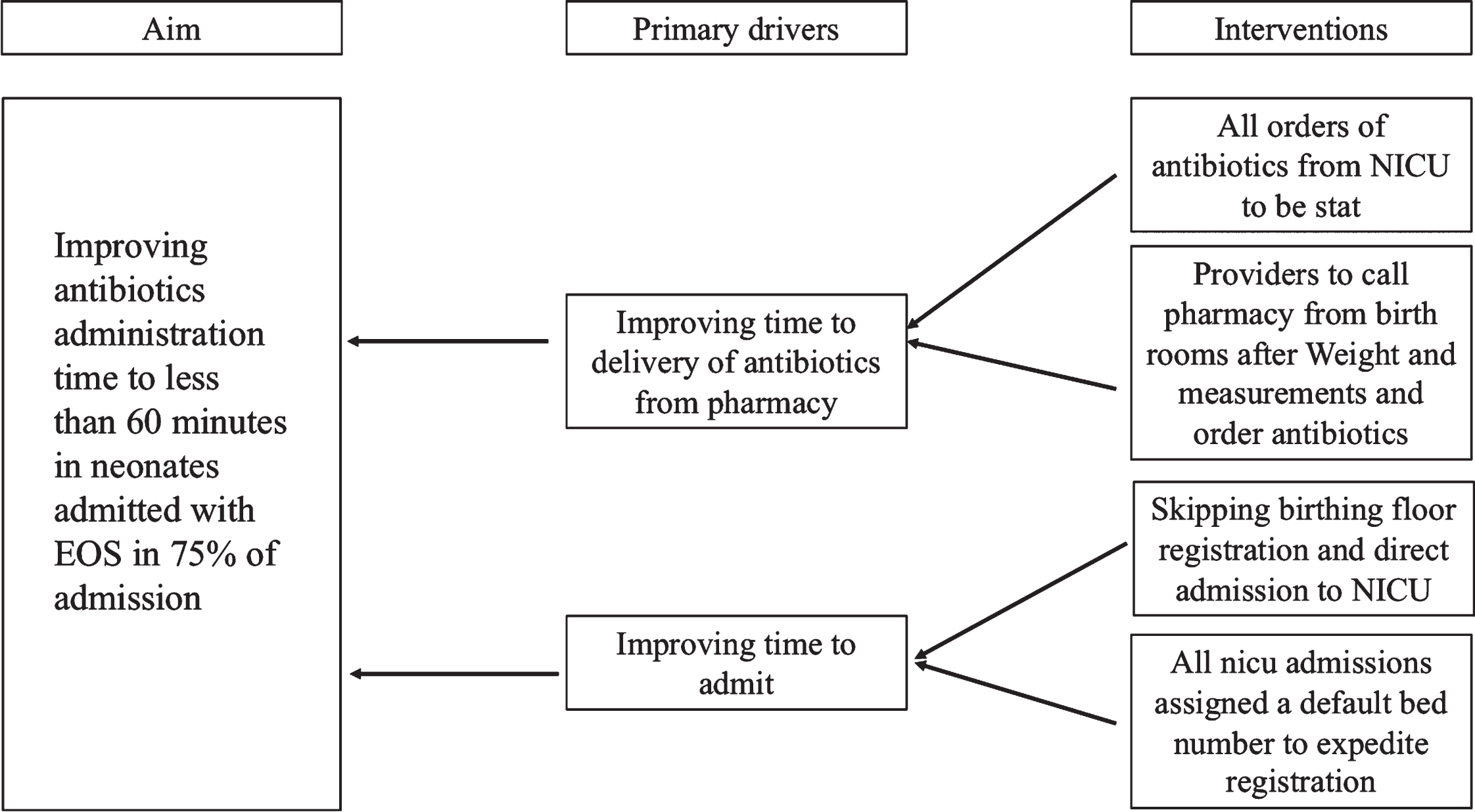
Drivers of change.
Our hospital is like many other children’s hospitals in that it is a hospital within a hospital type of system. The birthing unit, while in the same building, technically belongs to a different hospital which can lead to a whole host of problematic situations. Prior to initiation of this project birthing unit nurses used to notify the birthing unit registration staff who would in turn notify NICU registration staff for an admission and needed to wait for a bed number allocation. To simplify this process, we instituted a policy which created the provision for birthing unit nurses to call NICU registration staff to admit the incoming newborn to a default NICU bed number.
Plan-do-study-act activity II (October 2017-May 2018)
Workflow process and policy changes: A clinical pharmacist is present during rounds during the day time. Since our NICU does not have satellite pharmacy, all antibiotics are delivered from the pharmacy in pre-mixed syringes and verified by bedside nurses and bedside nurses do not have to mix antibiotics themselves. One of the prime obstacles causing a delay in antibiotics administration was a pharmacy requirement of having exact weight measurements prior to dispensing antibiotics, which led to delays in physician ordering. To speed up ordering of antibiotics, physicians and NNP were educated to call pharmacy to place verbal order for antibiotics after taking appropriate weight measurements in delivery units. To minimize medical errors the clinical pharmacist accepting the verbal order, verified mother’s last name, medical record number (MRN) and infant’s weight with ordering medical provider. The medication was again verified and crosschecked by bedside nurses before administering the antibiotics. All verbally placed orders were required to be placed in EMR via a computerized physician order entry (CPOE) immediately after admission of infant in EMR. All clinical pharmacists were requested to take verbal neonatal orders for antibiotics as STAT with target to deliver antibiotics within 20 minutes of the order placement. Next, for timely administration of antibiotics, in consultation with pharmacy and after reviewing literature, it was decided that ampicillin could be given over 5 minutes as slow bolus and gentamicin to be put on pump to complete infusion in 15 minutes. To standardize the process and to define start time, we followed two decision trees: A) if MD or NNP decided to admit a baby from delivery room for any reason and started antibiotics for suspected EOS, then onset of time was taken from time of initiation of transfer from delivery unit to the NICU, which was recorded by L&D nurses; b) If MD or NNP decided to start antibiotics for suspected EOS after admission to the NICU then onset time was taken from decision time and was recorded by bedside nurses. We decided to define target as time to initiation of infusion of antibiotics: ampicillin or gentamicin which ever came first from the pharmacy.
Accountability and problems with compliance
The biggest challenge that our interdisciplinary team expected for this project to succeed was the importance of exact time record keeping during each step of antibiotics administration. Issues that were identified were addressed with individual physicians, residents, nurse practitioners, nurses and pharmacists. Multiple sessions to improve sense of urgency for placing correct orders from birthing unit, improving delivery of antibiotics from the pharmacy, bedside intravenous access and administration of antibiotics to the patients were conducted. For time keeping, a prospective audit tool was developed and kept at the bedside to track time of birth, decision to admit time and initiate management of EOS with antibiotics, time to admit in the EMR, time to delivery of antibiotics from pharmacy from the time of order, time to infusion of antibiotics after delivery from pharmacy, time to insertion of intravenous lines and a comment section if time to infusion time went over 60 minutes to explain reasons for delay.
Statistical analysis
This study was approved by the Institutional Review Board of Texas Tech University Health Sciences Center at El Paso with exemption of consent. Analysis of variance was used to analyze the difference between the pre-intervention, PDSA cycle I and PDSA cycle II.
Normally distributed continuous data were analyzed by unpaired t-test. Categorical data was evaluated by Fisher’s exact test or Mann-Whitney test as appropriate. To show our data analysis we created a control chart which is used to determine whether process variation is in control and predictable. Control chart has a central line for the average, an upper line for the upper control limit, and a lower line for the lower control limit. These lines were determined from the data collected overtime.
Results
During this study period 1045 newborns were admitted to NICU. A total of 469 neonates were admitted with suspected EOS and received antibiotics. After excluding 56 neonates who either received comfort care or had insufficient data collected, a total of 413 neonates were included in the final analysis. Of those 29 were born during pre-intervention phase, 231 neonates were born during PDSA I and 153 neonates were born during PDSA II (Table 1).
Timeliness of administration of antibiotics
Timeliness of administration of antibiotics
a – Analysis of variance, P-value < 0.001. b- Analysis of variance, P-value < 0.05. c- Chi-square test, P-value of < 0.05.
The control chart for time to start of infusion, shown in Fig. 3, depicts no special cause variation over the period of this study between December 2016 and November 2018. The process remained stable as no data points were outside the control limits. Also, a steady and consistent decline in number of minutes to infusion of antibiotics was observed from PDSA I cycle to PDSA cycle II. There was statistically significant improvement in time to admission in electronic medical records over the time periods of pre-intervention, PDSA I and PDSA II (p-value < 0.05) (Table 1). Time to delivery of antibiotics from pharmacy was significantly reduced between PDSA cycles (p-value < 0.001) (Table 1). With improvement in overall workflow, average time to infusion of antibiotics decreased from 70 minutes to 48 minutes (p-value < 0.001) (Table 1). In addition, there was overall improvement in number of neonates receiving antibiotics under 1 hour of decision making (p-value < 0.05) (Table 1). Over the period of this project, a total number of 297 and 116 neonates received antibiotics under one hour and over one hour respectively. There was no difference in basic maternal and neonatal characteristics except for more mothers of Hispanic ethnicity in under one-hour group (Table 2). There was no difference in neonatal morbidities between two groups as well (Table 3).

Control chart.
Maternal and neonatal characteristics
Un-Paired t-test used for values with mean (SD). Fisher exact used for rest of the parameters.
Neonatal outcome
Un-paired t-test used for values with mean (SD). Fisher exact used for rest of the parameters.
This quality improvement project showed that timing of administration of antibiotics can be decreased in neonates admitted with suspected EOS by implementing a systematic quality improvement initiative. Average time to antibiotics administration decreased to 48 minutes, which was made possible by decreasing time to ordering antibiotics and delivery of antibiotics to pharmacy to 9 minutes. Verbal orders are discouraged in general, and as part of this quality improvement project the EMR systems in both hospitals are in process of complete integration and soon will negate the need of placement of verbal orders. All verbal orders were verified by the accepting clinical pharmacist as well as by bedside NICU nurses. Placing of verbal orders from delivery units did not lead to increase in errors which were tracked by pharmacy department. There was modest but significant improvement in time to admission to electronic medical record down to 22 minutes. All of the above interventions improved total number of neonates receiving antibiotics under one hour from 37% to 77% during the course of this quality improvement project. As we continue to work on our goal for antibiotics under one-hour, timely insertion of intravenous line, ordering of antibiotics and timely admission to EMR are still the areas where improvement is needed.
Our study has several strengths. First this is the only study to the best of our knowledge which describes antibiotics administration under one hour in neonates admitted with suspected early onset sepsis [11]. Workflow changes played a central role in achieving the goal of our QI initiative. We were able to overcome hurdles of a hospital within a hospital system with collaborative effort between the two institutions. Our study also demonstrates how detailed documentation can help improve process. Second, although unrecognized secular trends during the course of this project may have confounded the result, this study was performed over a relatively shorter period of time without obvious changes in NICU practices during this time period.
Although we were able to improve the timing of administration of antibiotics, our study analysis did not show statistically significant improvement in neonatal outcomes in neonates who receive antibiotics under one hour. Neonatology literature describing nursery practices or guidelines regarding the timing of antibiotics for suspected early onset sepsis is sparse [11, 12]. Although definitive data in neonates is lacking, it makes perfect sense that a shorter time to antibiotics administration may facilitate earlier killing of invading organisms and reduce likelihood of disease progression [13–15].
There are several limitations of our study. The unavailability of progression of inflammatory markers used routinely in critical care and the number of neonates who actually received a prolonged course of antibiotics. However, neonates in both groups of earlier vs delayed antibiotics were equally sick on admission as there was no difference in basic clinical characteristics and had similar outcomes during their stay in neonatal intensive care unit as depicted by morbidity data. Although, equal in basic clinical characteristics and admitted with suspected early onset sepsis, factually majority of neonates in the NICU do not actually have a culture proven or clinical infection [16, 17]. Analysis of neonates who receive prolong course of antibiotics can add more validity to the argument of early administration of antibiotics. Small sample size of our study is a limitation as well. Further prospective larger studies are needed to confirm our findings. Nevertheless, this was not a primary objective of this study. But, one can safely infer that timely administration of antibiotics in conjunction with supportive care plays an equally important role. Focus of our future PDSA cycles will be to identify further barriers and exploring possibility of keeping antibiotics in portable medicine system (Pyxis) in hope to increase number of neonates receiving antibiotics within one hour of decision making. We are currently in process of defining roles of nurses in this regard and putting in necessary safe guards to minimize medication errors.
Conclusion
In our study we were able to successfully implement our “antibiotics under one hour” goal. The ability to achieve this objective can be met across multi-institutions rendering care to newborns if the approach is multidisciplinary. Deleting obstructions in the process that involve admission, registration and order entry into the EMR effectively reduced time. Larger studies involving multiple centers are needed to further validate the results of this study.
Conflict of interest
All authors have indicated they have no potential conflicts of interest to disclose.
Funding source
No external Funding for this manuscript
Financial disclosure
All authors have indicated they have no financial relationships relevant to this article to disclose.
Footnotes
Acknowledgments
We thank Dr. Garrett Levin for his continued guidance during this quality improvement initiative, Hospital administration of both El Paso Children Hospital and University Medical Center for their support.