
Abstract
BACKGROUND:
Glycerin suppositories are often used to facilitate meconium evacuation in premature infants. The evidence for this practice is inconclusive. The purpose of this study was to assess the feasibility of a multicenter randomized controlled trial on the effectiveness of this treatment strategy.
STUDY DESIGN:
We conducted an external pilot study for a multicenter randomized controlled trial of premature infants randomized to glycerin suppositories or placebo procedure. Participants were included if they were gestational age of 24 weeks 0 days to 31 weeks 6 days and/or birthweight of 500 to 1500 grams. We excluded infants with life-threatening congenital anomalies, contraindications to receiving suppositories, or signs of clinical instability. Outcomes included cost, recruitment, and treatment-related adverse events.
RESULT:
A total of 109 were screened, 79 were initially eligible, and 34 consented to participate. Four of these infants were excluded prior to randomization due to thrombocytopenia, 30 were randomized, and 26 reached full enteral feeds. Three infants (10%) experienced rectal bleeding 5 to 43 days after completing study treatments. An anal fissure was noted in two of these patients. There were no cases of rectal perforation but one infant assigned to active treatment developed necrotizing enterocolitis.
CONCLUSIONS:
Conducting a multicenter randomized controlled trial on the use of glycerin suppositories in premature infants is feasible. Minor modifications to the study protocol are needed to increase participant recruitment and simplify the administration of study treatments.
Abbreviations
Necrotizing enterocolitis Neonatal intensive care unit Standard deviation
Introduction
Adequate nutrition is a significant challenge for premature infants in the Neonatal Intensive Care Unit (NICU) [1 –6]. These patients have immature digestive tracts and may take several days to pass meconium and develop a normal stooling pattern. Infants who take longer to achieve complete meconium evacuation also appear to experience delays in the transition to enteral feeding. As a result, many of these patients are given glycerin enemas or suppositories to stimulate the passage of meconium and improve feeding tolerance [7 –9]. One center reported that almost half of premature infants were treated with glycerin suppositories at least once during their NICU admission [9].
A systematic review and meta-analysis from 2015 assessed the evidence for the use of glycerin enemas and suppositories in premature infants identified. The authors identified a total of 185 participants from three single-center, randomized controlled trials [8]. These studies focused on the prophylactic use of glycerin enemas (one trial) or suppositories (two trials) [10 –12]. There were no differences between the intervention group (daily glycerin enemas or suppositories) and control groups (no intervention or placebo procedure) in terms of meconium evacuation, transition to full enteral feeding, or mortality. There were also no reports of rectal bleeding or perforation. The meta-analysis, however, revealed a trend towards increased risk of necrotizing enterocolitis (NEC) with active treatment. This trend was observed in all three trials but did not cross the threshold of statistical significance (risk ratio = 2.72, 95% confidence interval 0.76–9.81, I2 = 0%, p = 0.13).
The systematic review was complicated by the fact that all three trials were underpowered and affected by one or more methodological issues. For each outcome, the quality of evidence was therefore low to very low. The authors concluded that the evidence for the use of glycerin suppositories or enemas in premature infants is inconclusive and that further research is required. Similar findings and conclusions were reported by a Cochrane Review based on the results of the same three trials [13]. The authors concluded that the available evidence, ‘ ... does not support the routine use of prophylactic glycerin laxatives in clinical practice. Additional studies are needed to confirm or refute the effectiveness and safety of glycerin laxatives for prevention or treatment of feeding intolerance in [very low birthweight] infants.’ Two other single-center, randomized controlled trials have been published since then [14, 15]. These studies are also small and the authors were unable to make definitive conclusions because of insufficient statistical power.
We designed an external pilot study to assess the feasibility of a multicenter randomized controlled trial on the prophylactic administration of glycerin suppositories in premature infants [16, 17]. Outcomes for the pilot included recruitment rate, treatment-related adverse events, and cost. We also reported protocol violations, post-randomization exclusions, and other methodological challenges.
Methods
Study protocol
The Glycerin Suppositories Used Prophylactically in Premature infants (SUPP) Trial is an external pilot study for a placebo-controlled, parallel-design, multicenter randomized controlled trial. The study protocol was registered on clinicaltrials.gov (NCT02153606) and a complete description has been published previously [16, 17].
Participants
Premature infants were recruited from the Level 3 NICU at the McMaster Children’s Hospital. This unit has 42 beds and admits approximately 1100 infants per year of all gestational ages. Approximately 150 of these patients would be eligible for our study.
Parents or guardians were approached for consent postnatally within the first 48 hours of life. Inclusion criteria were gestational age of 24 weeks 0 days to 31 weeks 6 days and/or birth weight of 500 to 1500 grams. We excluded infants who had life-threatening congenital anomalies, were clinically unwell, or had contraindications to receiving a glycerin suppository (i.e., coagulopathy or neutropenia) [18 –20]. We also excluded those who had already achieved complete meconium evacuation, since most sources attribute the theoretical benefit of glycerin suppositories in premature infants to their ability to expedite meconium evacuation [7–9 , 13]. There may be a role to extend the duration of treatment but this has not yet been clearly established. Inclusion and exclusion criteria are listed in full in Table 1.
Inclusion and exclusion criteria
Inclusion and exclusion criteria
Active treatment consisted of 250 mg glycerin suppositories administered once daily starting between 48 and 72 hours of life (i.e., day 3). This smaller suppository was created by cutting the tip off a 1440 mg glycerin suppository. In order to maintain consistent dosing, we designed a plastic measurement guide that creates a glycerin ‘tip’ weighing approximately 250 mg [17]. In keeping with the usual practice in our unit, this medication was covered with a water-based lubricant and placed in the infant’s rectum.
Participants in the control group received 250 mg glycerin suppositories placed in the diaper once daily. In usual practice, partially dissolved suppositories are often ejected from the rectum either with or without stool. Leaving a suppository in the diaper (but not in the rectum) makes it ambiguous as to whether it was placed in the rectum and ejected, or simply placed in the diaper. Furthermore, ensuring that the charge nurses administered study treatments to all participants helped maintain blinding.
All participants received study treatments once daily until they passed two bowel movements free of meconium staining. This treatment duration was also used in a randomized controlled trial of glycerin enemas [10]. In the SUPP trial, the maximum treatment duration was set at 12 days, such that all treatments stopped on day 14 of life, regardless of stooling pattern. All infants were made nil per rectum while receiving study treatments and bedside nurses were advised not to reinsert suppositories found in the diaper.
Randomization
Infants were allocated to treatment groups via web-based, stratified blocked randomization. Previous studies have shown that the size of the infant is highly predictive of the time to full enteral feeds [21]. In order to maintain prognostic balance between groups, we stratified participants by gestational age: (1) 24 weeks 0 days to 27 weeks 6 days; or (2) 28 weeks 0 days to 31 weeks 6 days. This strategy has been used in other randomized controlled trials of feeding intolerance in premature infants [10, 11]. Further details regarding sequence generation, treatment codes, and block size are described in the study protocol [17].
On day 3 of life, one of the co-investigators discussed the infant’s status with the bedside nurse and reviewed recent bloodwork. If there were any relevant changes (e.g., need for vasopressors or development of thrombocytopenia), the infant was not randomized. If the infant continued to meet all inclusion and exclusion criteria, he or she was randomized to active treatment or placebo. This typically occurred before noon, which left ample time for the charge nurse on duty to administer study treatments during routine handling between noon and 6 : 00 pm.
Outcomes
Outcomes for the pilot study included recruitment rate (percentage of eligible infants randomized), completion rate (percentage of infants reaching the primary endpoint of full enteral feeds), treatment-related adverse events, and cost. We also assessed frequency and type of protocol violations and post-randomization exclusions.
The primary outcome for the proposed multicenter trial will be days to full enteral feeding (defined as 150 mL/kg/day). Advancing the rate of enteral feeds is typically based on a standardized NICU feeding protocol [22 –26]. Deviations from this protocol occur when infants become unwell, develop signs of feeding intolerance, or if there are other clinical concerns. Secondary outcomes for the multicenter trial will include feeding volume on day 14 of life (in mL/kg), days to complete meconium evacuation, days of parenteral nutrition, incidence of NEC, incidence of line sepsis, compliance with treatment regimen, and mortality.
Blinding
Parents and guardians, investigators, physicians, bedside nurses, allied health professionals (e.g., dieticians), research assistants, outcome assessors, and statistical analysts were blinded to treatment allocation. The only individuals who were not blinded were the charge nurses who administered study treatments. These individuals are experienced neonatal nurses who are not routinely involved in the bedside care of infants in the NICU.
Data safety and monitoring board
Members of the Data Safety and Monitoring Board (DSMB) included one pediatric surgeon and two neonatologists. This group met after the first five participants were enrolled and every three months thereafter to discuss treatment-related adverse events. There were no a priori rules regarding stopping the pilot study. The members of the DSMB were able to reveal the assigned treatment to determine if adverse events were related to treatment. Unblinding of participants was facilitated by a second research assistant who was not otherwise involved in the trial.
Statistical analysis
All data were analyzed in the Statistical Package for the Social Sciences (SPSS) version 22 (Chicago, IL, USA). Counts of days were reported using median and standard deviation (SD). Missing data were not imputed. Participants were analyzed on the basis of intention-to-treat (i.e., analyzed as randomized).
We chose a sample of size of 30 participants because previous methodological reviews of pilot studies recommend using at least 12 participants per group [27]. Other studies suggest that 30 may be more appropriate, especially if the data will be used to perform a sample size calculation [28 –30].
Results
Recruitment
The SUPP Trial opened to enrollment from January to June 2015, we recruited 22 participants who were 28 weeks 0 days to 31 weeks 6 days gestation. We then recruited 8 participants who were 24 weeks 0 days to 27 weeks 6 days gestation over another six-month period from September 2016 to February 2017. During these time periods, 109 infants were screened, 79 (72%) were initially eligible and approached for consent, and 34 (43%) consented to participate. Four of the infants who consented were ineligible at the time of randomization (i.e., day 3 of life) because their platelet counts had dropped below 100×109/liter. As a result, 30 of 75 (40%) were randomized and 26 reached the primary endpoint of full enteral feeds (Fig. 1).
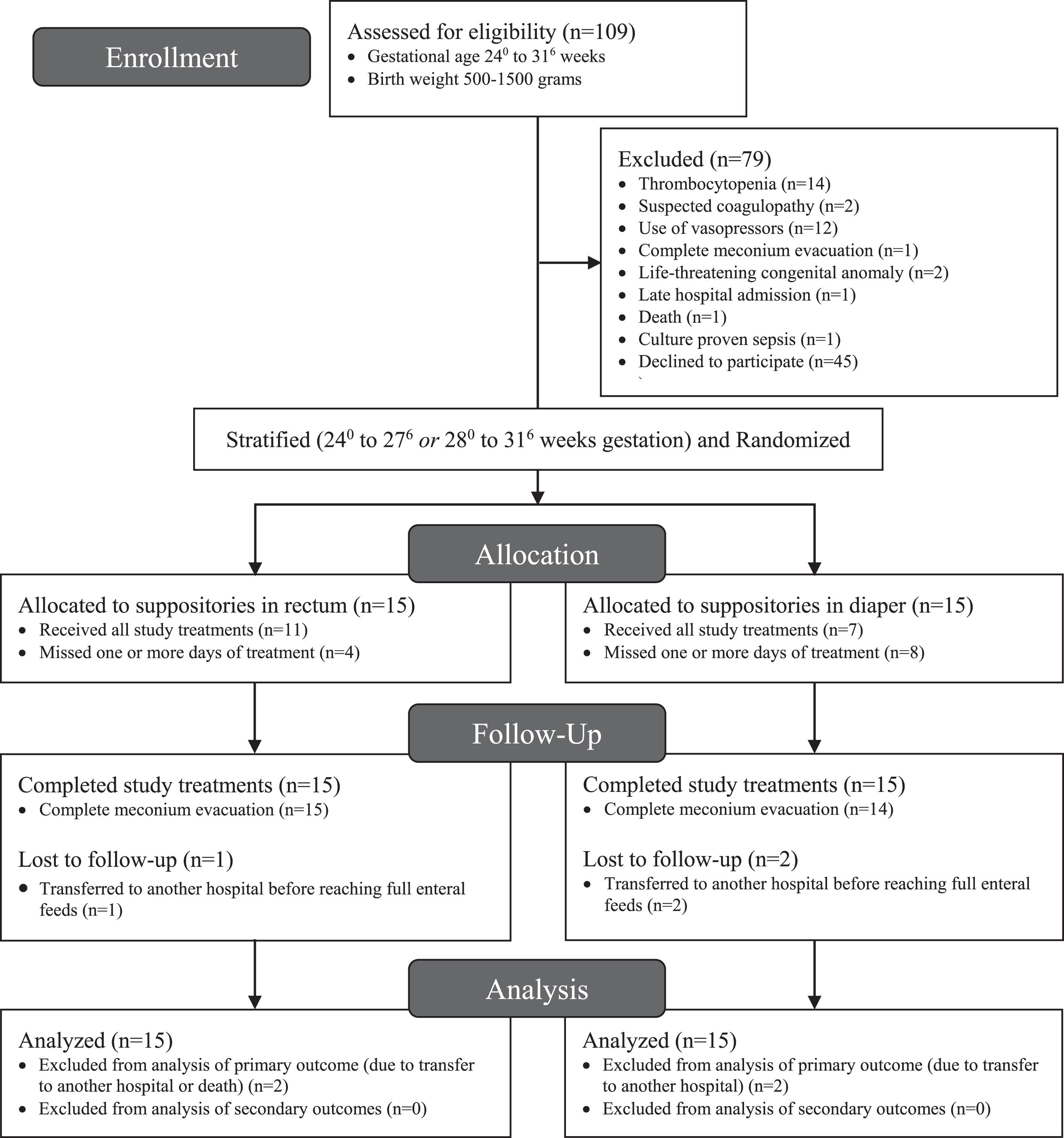
Recruitment of participants using the Consolidated Standards of Reporting Trials (CONSORT) flow diagram [34].
Some of the reasons for not providing consent included: belief that the infant was already clearing meconium and did not require a suppository; not wanting to expose their child to risk from suppository administration if it was not necessary; or simply not wanting to be involved in research. Recruitment rate was 30/75 (40%) and completion rate was 26/30 (87%). Baseline characteristics of participants who were randomized are summarized in Table 2.
Baseline characteristics of premature infants randomized to glycerin suppositories or placebo procedure
SD = standard deviation.
Three of 30 infants (10%) experienced a treatment-related adverse event. The first of these was an infant who received the placebo procedure once daily for six days. A ‘rescue’ suppository was administered on day 5 of life, complete meconium evacuation was achieved on day 9, and study treatment was stopped at that point. On day 13, the infant passed a few drops of bright red blood per rectum and was noted to have an anal fissure. The Pediatric Surgery service was consulted but no further investigations or treatment was recommended. Given the amount of time from treatment to the adverse event, the DSMB judged this outcome as ‘possibly’ related to study treatment.
The second infant received active study treatments (i.e., glycerin suppositories per rectum) once daily for five days. Complete meconium evacuation was achieved on day 8 of life. Twenty-eight days after receiving study treatments, the stool was found to be streaked with blood and an ulcerated perianal rash and anal fissure were noted. The anal fissure healed but the infant continued to have excoriated buttocks for a month until the infant was diagnosed with cow’s milk protein allergy. The mother started a dairy-free diet and the skin healed with the assistance of a zinc-based cream.
Finally, the third infant received active study treatments for four days and complete meconium evacuation was achieved on day 7 of life. Forty-three days after completing study treatments, streaks of blood were noted in the stool. This patient was also determined to have cow’s milk protein allergy and the stools cleared after the mother started a dairy-free diet. These last two events were judged to be unlikely related to study treatment.
There were no cases of rectal perforation. One infant in the intervention group died after completing study treatments and another experienced a late mortality after exiting the study. Both participants were born before 28 weeks gestation. The first infant completed study treatments on day 11 of life with no apparent complications. She later developed gram-negative and Staphylococcus aureus sepsis on day 20 of life and died on day 22 due to septic shock. The death was discussed with DSMB members and was determined to be unlikely related to study treatments.
The other infant started study treatments on day 3 of life. These were stopped on day 9 after he developed abdominal distension and pneumoperitoneum. The infant underwent urgent laparotomy and was found to have a spontaneous ileal perforation, which was treated with an end ileostomy and mucous fistula. Seventeen days later, on day 25 of life, the infant experienced generalized peritonitis and underwent a second laparotomy. This revealed a perforation in a dilated portion of proximal small bowel. The surgical team created a proximal loop ileostomy and revised the end ileostomy.
The infant continued to have difficulties with recurrent sepsis and ultimately underwent a third laparotomy of day 71 of life to determine if this was due to an intra-abdominal source. He was found to have patchy areas of small bowel necrosis and pneumatosis intestinalis consistent NEC. The infant underwent small bowel resection, revision of the mucus fistula, and temporary abdominal closure with placement of a silo. The infant’s course was also complicated by severe bronchopulmonary dysplasia, recurrent sepsis, cholestasis from parenteral nutrition, patent ductus arteriosus, intraventricular hemorrhage, and retinopathy of prematurity. He continued to have recurrent sepsis and died on day 127 of life at a corrected gestational age of 43 weeks and 2 days. These events were reviewed by the DSMB and judged to be unlikely due to study treatments. Complete safety and feasibility data are summarized in Table 3.
Safety and feasibility outcomes of premature infants randomized to glycerin suppositories or placebo procedure
Safety and feasibility outcomes of premature infants randomized to glycerin suppositories or placebo procedure
SD = standard deviation.
Fifteen of the 30 participants experienced at least one protocol violation. One participant received the first study treatment after 72 hours of life, which was six hours later than indicated in the study protocol. This occurred because the charge nurse was unavailable to administer the study treatment at the usual time because of a contamination issue in the NICU unrelated to the study.
Twelve participants (40%) missed one or two days of treatment with a total of 21 out of 197 (11%) missed study treatments. With the exception of one day, where a charge nurse mistakenly believed study treatment should have been stopped for two patients, these instances were attributed to exceptionally busy days in the NICU. In most instances, the charge nurse was working alone with no other personnel available to assist with administering study treatments.
Four participants (13%) received treatments one or two days longer than required. The first case occurred over the first weekend of the study. The infant passed two normal stools (free of meconium staining) on two separate days and this was not recognized prior to the infant receiving an additional day of treatment. The second and third cases occurred several months into the study on very busy days. The charge nurse was managing a heavy workload and forgot to confirm meconium evacuation prior to giving an extra study treatment. One infant also received two extra days of treatment. This patient had already received 12 days of treatment without meconium evacuation, and study treatment should have stopped as per protocol.
Cost
The costs of conducting the pilot study were documented in Canadian dollars. These included: (1) salary for the part-time research assistant responsible for obtaining consent and collecting outcome data ($22.60/hour×15 hours/week×36 weeks=$12,204); (2) honorariums to compensate charge nurses to administer study treatments ($100 per nurse×26 nurses = $2,600); and (3) administrative costs for printed materials (approximately $1,000) and server space (approximately $500). As a result, the cost for each participant randomized was approximately $530.
Other methodological issues
Three infants (10%) were transferred to a Level 2 NICU at a community hospital prior to reaching full enteral feeds and one infant died before reaching 40 weeks corrected gestational age. Seven infants (23%) received a rescue suppository prior to completing study treatments (2/15 in the active treatment group and 5/15 among those randomized to placebo procedure). Two of these (7%) received rescue suppositories prior to starting study treatments because they were judged to have signs of feeding intolerance by the medical and nursing team. One received a rescue suppository on day 2 of life (prior to randomization) and the other on day 3 (six hours before the first study treatment was administered). The most common reason given for the other five infants was that no significant stooling had occurred for at least 48 hours.
Discussion
This external pilot study assessed the feasibility of a multicenter randomized controlled trial of glycerin suppositories among premature infants. One of the issues that surprised us was the number of infants who initially met the inclusion criteria but had to be excluded prior to randomization on day 3 of life. Fortunately, we set up our study protocol with two inclusion and exclusion criteria ‘checkpoints’: one at the time of consent (usually within the first 48 hours of life) and one immediately prior to randomization (before noon on day 3 of life). If we had randomized participants at the time of consent, then 4 of 34 infants (12%) would have stopped treatment early due to post-randomization exclusions.
The most common reason for an infant being ineligible was thrombocytopenia. Ten of 109 screened participants (9%) were not approached for consent and four others (4%) were not randomized for this reason (13% total). The mean platelet count for these infants was 79×109/liter (range 67 to 90×109/liter), which was only slightly below our cut-off of less than 100×109/liter. If the exclusion criterion had been set at 50×109/liter, then none of these infants would have been excluded.
Randomizing participants on day 3 of life meant that all potentially eligible participants could be approached for consent on a weekday. For example, an infant born on a Monday could be approached for consent on Tuesday and randomized on Wednesday. An infant born on a Saturday could be approached for consent on Monday morning and randomized at noon that same day. The other benefit of randomizing infants on day 3 of life was that it selected out infants who were likely to be excluded for clinical reasons once they started treatment. Infants in both strata had plenty of time to declare themselves as clinically unwell (e.g., needing vasopressors or developing culture-positive sepsis) before being randomized. From a clinical perspective, the infants who were ultimately randomized in this study tended to be the ‘feeders and growers’ who were most likely to benefit from routine glycerin suppositories because they were: (1) not initially unwell and; (2) did not achieve complete meconium evacuation until at least day 4 of life.
A significant challenge from a feasibility standpoint was the need to assess participants each day and decide whether study treatments should continue or be stopped. When we designed the study protocol, we believed that the only potential benefit of administering glycerin suppositories prophylactically was to facilitate meconium evacuation. Thus, giving glycerin suppositories beyond the point of complete meconium evacuation would likely have no benefit and only expose participants to the small but non-zero risk of rectal perforation, rectal bleeding, or anal fissure.
On a practical level, however, stopping study treatments after complete meconium evacuation meant that our research assistant had to spend considerable time each day reviewing bedside charts and discussing with the clinical team if infants should continue to receive study treatments as per the study protocol. This involved carefully reviewing the nursing record of each participant and deciding whether they had passed two normal bowel movements free of meconium staining. This close monitoring was time-intensive and may not have been necessary. In fact, two previous randomized controlled trials of glycerin suppositories in premature infants used fixed duration of treatment: (1) 10 days starting at 24 hours of age [12]; or (2) 13 days starting at 48 hours of age [11]. None of the infants in these trials (n = 104) experienced a treatment-related adverse event and determining the length of treatment duration was greatly simplified.
An even better option might be to use predefined duration of treatment for each age group (i.e., stratum) based on the median treatment duration in the pilot study (e.g., 5 days total for infants 28 weeks 0 days to 31 weeks 6 days gestation). This would minimize the need for a long course of treatment in the older age group and ensure that infants in the younger group received sufficient therapy to clear meconium in most cases. Using this approach in a multicenter trial would be far more feasible than using a variable duration of treatment as we did in this pilot. This approach would also likely decrease the rate of protocol violations. Furthermore, stooling pattern would not have to be assessed on a daily basis.
Another challenge was the number of participants transferred to a Level 2 NICU in a community hospital prior to reaching full enteral feeds. In the study protocol, we anticipated that some infants would be transferred prior to reaching term (i.e., 37 weeks gestation) but not likely before reaching full enteral feeds [17]. In practice, however, this turned out not to be the case and some participants were lost to follow-up.
We were concerned to see that ‘rescue’ suppositories were used more frequently in the control group (5/15 infants) compared to those randomized to active treatment (2/15 infants). This may have been a consequence of these infants not receiving glycerin suppositories and not having regular stools. The other possibility is that some element of unblinding and bias played a factor in the decision to administer rescue suppositories. For example, some of the bedside nurses or medical personnel may have become unblinded (by secretly observing which study treatments were administered, overhearing treatment assignments being discussed by the charge nurses, opening the infant’s diaper immediately after study treatments were administered, etc.). If these clinicians realized that certain infants were assigned to receive the placebo procedure only, then they might have been more likely to advocate for the use of rescue suppositories with the medical team.
One possible solution would be to set up more stringent criteria for the use of rescue suppositories (e.g., only if infants have not stooled in 48 hours and there is ongoing clinical concern). We intentionally did not do this in the pilot study because we wanted this study to be pragmatic. We also wanted clinicians to feel free to use their best judgement and not give the impression that infants in our trial were ‘not allowed’ to receive non-study glycerin suppositories. Setting up specific rules for initiating rescue treatment makes the study less pragmatic and may make the multicenter trial less feasible.
Another option would be to modify the blinding strategy. Some clinicians suggested that infants randomized to the placebo procedure should have suppositories discarded rather than placed in the diaper. This approach was used in the trial by Shinde et al., where the intervention in the control group was simply opening and closing the diaper [11]. Another advantage of using this placebo procedure is that infants assigned to active treatment could have suppositories that were ejected re-inserted into the rectum rather than left in the diaper. This may increase the effect of the study intervention (if one actually exists). While this approach may have some advantages in theory, we were concerned that in practice, this might result in some charge nurses not performing the placebo procedure at all. Leaving suppositories in the diaper acts as a reminder for the charge nurses to go to the bedside and participate in the treatment ritual on a daily basis. This likely helped maintain blinding and compliance.
In the study protocol, we planned to recruit participants in both strata (24 weeks 0 days to 27 weeks 6 days; and 28 weeks 0 days to 31 weeks 6 days) at the same time. When the study was conducted, however, there were concerns about treatment safety in the younger age group. Thus, we decided to enroll infants in series, with the older age group participating first. Once we had safely demonstrated the study procedures, we were able to proceed with recruiting infants in the younger and more vulnerable stratum. We selected the distribution of 22 and 8 participants in each age group, respectively, to reflect the overall distribution of premature infants in our unit. The disadvantage of this approach, of course, was that infants in each stratum were enrolled during different time periods. In the larger, multicenter study, it will be essential to recruit all participants concurrently. Particularly, to ensure that date does not become a significant covariant.
Finally, a philosophical issue that came up during the course of the pilot study was whether the term ‘placebo’ was appropriate to use in reference to glycerin suppositories left in the diaper. Some clinicians felt that this intervention was a form of ‘sham’ therapy. A Cochrane Review from 2010 reported that there is no formal definition of placebo that clinicians and researchers agree upon [31]. They noted that: “It is generally assumed that any effect of a placebo intervention is unrelated to its essential component ... but caused by the special interaction between patient and healthcare provider associated with the treatment ritual.” Similarly, a systematic review of sham interventions noted that these procedures are “ ... characterized by physical change of bodily tissue through manual or robotic operation and thereby inherently imply physical harm and/or risks” [32]. Thus, we believe the term ‘sham’ implies a level of risk that does apply to the control intervention in this trial (i.e., leaving a glycerin suppository in the diaper).
Conclusion
The evidence for the use of glycerin suppositories in premature infants remains inconclusive. Despite the ‘absence of evidence’ [33] for the use of glycerin suppositories in premature infants, this treatment strategy remains pervasive in many neonatal intensive care units. The results from our study suggest that conducting a multicenter randomized controlled trial is feasible. The protocol will need minor modifications but this should not deter us from conducting a definitive study on this common clinical practice.
Funding source
The SUPP trial was funded by a McMaster Surgical Associates Innovation Grant. Dr. Michael Livingston is supported by the Regional Medical Associates Scholarship Award and the Clinician Investigator Program at McMaster University (funded by the Ontario Ministry of Health and Long-term Care). These organizations had no role in developing the content of this manuscript.
Conflict of interest
The authors declare no conflict of interest.
Footnotes
Acknowledgments
We would like to thank Henrietta Blinder, Christina Sguazzin, Julia Pemberton, Bethany Easterbrook, and Adriana Dekirmendjian for their administrative and technical assistance. We would also like to acknowledge Stephanie Becker and the neonatal nursing team at McMaster Children’s Hospital for their enthusiasm and support. The members of the Data Safety and Monitoring Board include Drs. Salhab el Helou, Sandesh Shivananda, and Karen Bailey. Finally, we would like to thank Drs. Luis Braga and Lehana Thabane for reviewing the manuscript and providing feedback.