
Abstract
The information regarding fetal effects of acetazolamide use during pregnancy and lactation is sparse. We report the clinical and pharmacodynamic characteristics of maternal acetazolamide use and the timing of its effects on acid-base balance in three cases who presented with metabolic acidosis in the newborn period. We found that the infants’ clinical status soon after birth was inconsistently correlated with maternal drug dose and concentrations of medication in maternal serum. However, there was low transfer of the drug in breast milk and its use did not affect clinical symptomatology. We also present a review of literature on this subject to help consolidate our current knowledge on this topic.
Abbreviations
Continuous positive air pressure
Neonatal intensive care unit
Introduction
The current medical literature is abundant with data on the fetal effects of drugs taken by the mothers during pregnancy and lactation. Acetazolamide is a non-competitive inhibitor of carbonic anhydrase, the enzyme responsible for forming hydrogen and bicarbonate ions from carbon dioxide and water. Its use in pregnant and parturient women is commonly for indications of glaucoma, or benign intracranial hypertension or pseudo tumor cerebri. Acetazolamide has many effects that determine its clinical use, including the effects on – electrolyte and acid-base balance, CSF production, cardiac and brain electrical activity. The use of this drug in older children and adults is well tolerated with physiological adaptations that occur gradually over time during its chronic use. However, its effect on serum electrolytes and hypochloremic-non-anion gap metabolic acidosis may have important implications in newborn infants transitioning from the fetal to the extra-uterine environment where normal renal and respiratory adaptive mechanisms may not be fully effective [1]. Maternal use of acetazolamide is suspected to have an effect on the fetus and newborn infant, based on case reports of clinical effects correlated with infant serum concentrations documented after birth [1–3]. However, the pharmacokinetic link between maternal dose, maternal serum concentration, placental transfer, infant serum concentration and infant clinical status have not been adequately characterized.
This report was based on a retrospective compilation of data from patients treated by one of the authors. Therefore, patient consent was not obtained as recommended by the Institutional Review Board at Connecticut Children’s Medical Center.
Case 1
A 28-year old G1P0 mother delivered a male infant vaginally at 32 weeks gestational age. There were no perinatal problems except for preterm labor and spontaneous rupture of membranes at <12 hours prior to delivery. Her past history was significant for a non-active herpes simplex-2 infection and her current pregnancy was complicated by hyperprolactinemia, and pseudo tumor cerebri. She was on treatment for pseudo tumor cerebri with acetazolamide at a dose of 1500 mg/day in three divided doses. There was no report of fetal distress except for brief tachycardia to 170 beats/min noted just prior to delivery.
The infant presented at birth cyanotic and limp with a weak cry. Apgar score at one, five and ten minutes were 2, 5 and 8 respectively. Birth weight was 1610 g. He was dried, stimulated and bulb suctioned with poor response. He was provided respiratory support with bag and mask positive pressure ventilation following which he improved. He was admitted to the NICU on nasal CPAP with 6 cm of H20 pressure and 40% of supplemental oxygen. In the NICU, he continued to have tachypnea, moderate subcostal retractions, decreased neurological tone and activity and was therefore electively intubated. His initial blood gases showed pH 7.27; PaO2 105 mm Hg; PaCO2 34 mm Hg; and base deficit – 10 Mmol/L, suggestive of metabolic acidosis. Initial CXR showed well expanded lungs with very mild haziness. Surfactant (Curosurf® 2.5 ml/kg intra-tracheal) was given at 1 hour of life and infant was extubated soon afterwards. Infant was supported on nasal CPAP with 6 cm of H20 pressure without supplemental oxygen. Subsequent blood gas showed continuing metabolic acidosis with base deficit of – 10 for which a single bolus (10 ml/kg IV) of 0.9 % normal saline was given followed by a 2 mEq/k/dose of sodium bicarbonate that was administered by slow intravenousinfusion.
Soon after birth the CBC and differential counts were within normal range. After obtaining blood cultures, the infant was started on ampicillin and gentamicin 100 mg/k/dose IV every 12 hours and 4.5 mg/k/dose IV every 36 hours respectively for the suspicion of sepsis. Antibiotics were discontinued at 48 hours of age when the suspicion of sepsis was cleared. Serum electrolytes at 12 hours of age showed hypochloremia and a non-anion gap metabolic acidosis (Na 138 mEq/L; Chloride 99 mEq/L; and K 4.6 mEq/L) which resolved over the next 2 days. Baby remained euglycemic and laboratory values for serum calcium, serum magnesium, blood urea nitrogen and creatinine remained within normal range for age. Acetazolamide serum concentration was found to be 10 mcg/ml in the cord blood collected soon after delivery and at that time, the maternal serum concentration was 30 mcg/ml. Subsequently when there was sufficient maternal breast milk production on day 1-2 after birth, acetazolamide concentration in the breast milk was found to be 4.2 mcg/ml (test reporting limit – 0.5mcg/ml). Within the first 24 hours after birth, the infant serum concentration of acetazolamide was 10 mcg/ml.
The metabolic acidosis resolved within 6 hours of birth without any additional treatment; and hypochloremia resolved within 24 hours of birth. Infant recovered from respiratory symptoms within 2 days and remained well for another 6 days. Incidentally, he was subsequently diagnosed with a left upper lobe congenital lobar emphysema that needed surgical resection prior to discharge home.
Case 2
A 29-year old G3P1 delivered a 39-week gestational age, male infant after a cesarean section for maternal ocular myasthenia gravis. There was artificial rupture of membranes at time of delivery. During pregnancy, the mother was treated for depression and pseudo tumor cerebri. She had intermittently taken Fioricet® throughout her pregnancy. She was also on regular treatment for pseudo tumor cerebri with acetazolamide at a dose of 1000 mg/day divided twice a day. There was no fetal distress before delivery. A vigorous male infant was delivered with good tone and spontaneous cry. Birth weight was 3325 gm and the Apgar scores at 1 and 5 minutes were 8 and 9 respectively. He received routine newborn care, and was admitted to the NICU without any medical intervention except to be monitored for cardiorespiratory stability secondary to maternal myasthenia gravis and the risk that maternal antibody may cause respiratory depression in the infant. The infant had a normal physical exam at admission but soon developed mild grunting, tachypnea and intermittent oxygen desaturations with poor respiratory effort. After evaluation with blood gases and chest radiograph supplemental oxygen therapy was started. Initial chest radiograph showed clear lung fields and good lung expansion. Blood gas done 4 hours after birth showed metabolic acidosis with pH 7.21; PaO2 42 mmHg; PaCO2 53 mmHg; and base deficit – 8 mMol/L. Blood gases continued to improve for metabolic acidosis and the base deficit cleared by the 2nd day of life. Serum electrolytes, calcium and magnesium concentrations remained within normal range. The need for supplemental oxygen was confirmed to be due to hypoventilation secondary to transient effect of maternal antibodies for myasthenia. This problem resolved completely by the 13th day of life when he was weaned to room air without need for respiratory support. Infant was discharged home on 17th day after birth with no active medical issues. However, on later follow-up this infant developed neurological signs consistent with autism spectrum disorder at 3 years of age. In this case, acetazolamide concentration in the cord blood at birth was 10 mcg/ml while the maternal serum concentration was 3.7 mcg/ml soon after birth. No other drug levels were available. The baby was electively given formula feeds and no measurements were made of the breast milk for drug concentrations.
Case 3
A 32-year old G2P0 delivered a 39-week gestational age female infant by primary elective cesarean section for idiopathic intracranial hypertension as straining during labor was contraindicated. There was artificial rupture of membranes at the time of delivery. Pregnancy was complicated by morbid obesity, insulin-dependent diabetes mellitus, asthma, gastroesophageal reflux disease, migraines, depression and severe anxiety. The mother’s chronic medications during pregnancy included – insulin, albuterol, sertraline, quetiapine, hydrocodone, and acetaminophen. She was also on treatment with acetazolamide at a dose 1500 mg/day in 3 divided doses for pseudo tumor cerebri with idiopathic intracranial hypertension. There was no fetal distress before delivery. There was spontaneous rupture of membranes with meconium stained fluid just before delivery. The infant’s birth weight was 3800 gm and she presented with a spontaneous cry and Apgar scores at 1, 5 and 10 minutes of 6, 7 and 8 respectively. She was bulb-suctioned for large amount of meconium from mouth, nose and stomach. She was non-dysmorphic but had increased work of breathing with grunting, nasal flaring and chest retractions. The infant also had decreased neurological tone. The umbilical cord arterial blood pH was 6.98; and base deficit was – 16.7 mMol/L. Infant was given respiratory support with nasal CPAP and 40% supplemental oxygen and transferred to the NICU. An arterial blood gas obtained from the infant at about 4 hours of age had a pH of 7.28, PaCO2 of 46 mm Hg, PaO2 of 67 mm Hg and base deficit of – 5 mMol/L. Initial chest radiograph showed non-specific densities. After obtaining blood cultures, infant was treated with Ampicillin and Gentamicin for 48 hours until the suspicion for sepsis was resolved. The infants’ respiratory status started to improve and she was weaned off nasal CPAP support by the 2nd day of life. The metabolic acidosis also resolved by 2nd day of life. Infant remained euglycemic during hospital stay. Serum electrolytes and calcium concentrations were not measured. Infant resolved all medical issues by 3 days of age when she was discharged home with parents. Infant received breast milk throughout the hospital stay despite maternal use of acetazolamide during this time. Acetazolamide in the maternal serum soon after delivery was 10 mcg/ml. Acetazolamide concentration in infant’s umbilical cord blood was 4.6 mcg/ml. Acetazolamide in the breast milk within 2-3 days of delivery was found to be 4.2 mcg/ml.
Discussion
Acetazolamide is a drug that has many medical uses, including preoperative management of closed-angle glaucoma, adjunct treatment for open-angle glaucoma, management of fluid- induced edema, and congestive cardiac failure. Due to lack of availability of safety data, its use in pregnant women is mostly limited to severe glaucoma, pseudo tumor cerebri or idiopathic intracranial hypertension. In adults a therapeutic acetazolamide concentration in the serum is 3–10 mcg/ml [4] and toxicity is sometimes seen at >20–40 mcg/ml [5] but the bioavailability of this drug is variable especially during pregnancy [6]. Moreover, kinetics of maternal-placental and fetal transmission have not been studied.
It is well known that drug bio-physicochemical properties such as molecular weight, ionization at physiologic pH and protein binding affinity play an important role in transfer of drug across the placenta [7]. Acetazolamide, with a low molecular weight of 222 gm/Mol can easily transfer across placenta but because it is 90% bound to plasma protein the amount of free drug available for transfer may be limited. The rate of transfer may therefore be increased by high maternal serum concentration, low serum protein status and good utero-placental blood flow, while conditions such as preeclampsia may decrease drug transfer [7]. It is unclear if there are any modifying factors in the placenta and if the fetal concentrations are different from maternal concentrations.
Previously reported cases along with details of the three cases reported in this series are shown in Table 1. The earliest reports of acetazolamide use in pregnant women were for the treatment of pre-eclampsia and fluid retention, but no details of fetal or infant effects were reported [8]. A letter to JAMA in the year 1957, described an infant with dehydration at 48 hours after birth, born to a mother who was taking 250 mg/day of acetazolamide for the last 3 weeks of her pregnancy [9]. In a report of birth defects and drugs in pregnancy, based on 50,282 mother-infant pairs, Heinonen et al. reported only 12 instances of acetazolamide use, but did not report any effects on the infant [10]. The first detailed report of effects of maternal acetazolamide on newborn infant, were described in a 2 day old, 36 week gestational age, 2400 gm birth-weight infant with metabolic acidosis that lasted for 2 days and recovered spontaneously despite breast feeding by the mother [2]. In this instance the mother had taken acetazolamide 500 mg/day divided twice a day, throughout pregnancy for treatment of glaucoma. Infant also showed transient hypocalcemia and hypomagnesemia on day 1-2 after birth [2]. No drug concentrations were reported and correlation with clinical symptoms was not possible [2]. A case of a preterm infant with transient renal tubular acidosis was reported after maternal use of acetazolamide (750 mg/day for 3 days) for glaucoma during pregnancy. Acetazolamide concentrations were measured in the baby’s serum (2.9 mcg/ml at 5 hours after birth) demonstrating trans-placental passage [3]. The teratogenic potential of acetazolamide is established in rats, hamsters and mice, but not in monkeys [11]. In humans, Heinonen et al. [10] did not find any congenital malformations among offspring of their 12 patients who had used carbonic anhydrase inhibitors during pregnancy. Only one case of multiple congenital malformations (glaucoma, microphthalmia and patent ductus arteriosus was related to acetazolamide use based on a letter from Lederle laboratories in 1975, as cited by Worsham et al. [12], in their case-report. In this report, one women on 750 mg per day of acetazolamide for glaucoma during the 1st and 2nd trimester had a baby with sacrococcygeal teratoma; but no causal link could be made. Teratogenicity tests in rats and mice showed the absence of fourth and fifth digits from the right forelimb in the offspring of rats and mice [13–15]. In the three cases that we report, it may or may not be a coincidence that one infant had left sided congenital lobar emphysema and another who was born to mother with ocular myasthenia gravis developed signs of autism-spectrum disorder by 3 years of age. In a longitudinal observational study of 6 women treated for glaucoma during pregnancy, where acetazolamide was used mostly in the third trimester (except in 2 women where it was used from the first trimester) the only adverse effect reported was low birth weight in exposed infants [16]. Metabolic acidosis and electrolyte effects were not reported, but these infants were found to be well in the newborn period and continued to do well at their 2-year follow-up [16]. In a study reporting the results of a questionnaire survey of 101 women (158 pregnancies) who were treated for idiopathic intracranial hypertension during pregnancy with acetazolamide starting before 13 weeks of gestation, there were no reports of congenital defects or neonatal problems [17]. Another case series of 12 women treated during pregnancy with acetazolamide for idiopathic intracranial hypertension reported the lack of adverse effects on the fetus or the newborn infant [18]. Even though these reports are reassuring, none of them were focused on evaluation of the physiology and metabolism of newborn infants.
Acetazolamide use during pregnancy and effects on newborn – review of literature and our 3 cases
BW – Birth Weight; GA – Gestational age at birth in completed weeks.
In our present case series we highlight the finding of metabolic acidosis after birth. The finding of metabolic acidosis correlated with respiratory symptoms and was confirmed by obtaining a blood gas. In all instances, there was a need for medical management of metabolic acidosis. The inconsistent correlation of infant’s symptoms and acidosis to serum concentrations of acetazolamide may depend on a complex interaction between maternal-placental and fetal pharmacokinetics and needs further elucidation. Very little is known about the transfer of this drug in breast milk and all of the information available is from a single case report [19]. However, it is reassuring that our findings of breast milk concentration of 4.2 mg/ml was very similar to that concentrations reported by Soderman et al. [19]. Therefore we were able to confirm that the amount of breast milk ingested by the baby per day from a women who is taking therapeutic doses of acetazolamide, would not result in a significant serum concentration in the infant. This was reaffirmed with our finding that the two infants in our case series resolved their metabolic acidosis despite getting the majority of their nourishment from breast milk.
The possible mechanism of maternal acetazolamide effect on the newborn infant can be explained by integrating the various observations from our cases and a review of literature. We have shown that there is variation in bioavailability of the drug. In two of our three cases, there seems to be a good correlation between maternal drug dose and serum concentrations in the mother around the time of delivery; and our findings confirm this observation in pregnant women [4, 20]. It has previously been shown that a maximal dose of 1000 mg/day results in a therapeutic serum concentration of 10 mcg/ml in non-pregnant individuals [20]. We found that maternal serum concentrations could however vary from 3.7 mcg/ml to 30 mcg/ml with doses between 1000 to 1500 gm/d. This may be due to the effect of maternal serum protein and placental blood flow or the interaction with other drugs. It is also clear that acetazolamide transfers from the mother to the fetus across the placenta as evidenced by the cord blood concentrations that we and others have measured [3]. We have shown that the fetal or umbilical cord blood concentrations may be higher or lower than the maternal concentrations and therefore maternal serum concentrations alone may not predict the newborn’s symptoms. Extrapolating from the information that following an oral dose of acetazolamide, there is a predictable rise and fall in serum concentrations (peak in 1-2 hours.; elimination half-life 10–12 hours) [6], it can be estimated that umbilical cord blood concentrations may be a good guide to the newborn’s symptoms and effects, therefore, repeated measurements from the infant’s blood may not be necessary. The effect of the drug on fetal and infant metabolic status has been shown in experiments with pregnant sheep [21]. The pathogenic effects of acetazolamide relating to tissue injury and metabolic acidosis may not only be due to the effect on renal carbonic anhydrase but may also be from an acquired enzymatic injury resulting from the inhibition of mitochondrial carbonic anhydrase V that provides bicarbonate to pyruvate carboxylase and can produce tricarboxylic acid cycle damage resulting even in lactic acidosis. Therefore, acidosis in some instances may be due to both bicarbonate loss and increase in lactic acid. There are no clinical reports of lactic acid measurement except in the one case reported by Filippi et al. where the use of citrated products help in treating the lactic acidosis [22]. We have no measurements of lactate in our cases but have evidence of non-anion gap acidosis in one of the cases, which may have been due to lactic acid.
Another point highlighted by our case series is the potential effect of gestational age. Maturational differences have been demonstrated in the effect of acetazolamide in laboratory animals [23]. It is possible that the effects of placental transfer or infant metabolism are more profound in the premature infant, as most of the cases reported with infant symptoms were preterm infants. Term infants do not appear to be as affected both in our experience and in earlier reports [16, 24]. From our cases and the reported literature, we have developed a putative model of maternal-infant acetazolamide related interactions (Fig. 1). Maternal use of acetazolamide during pregnancy results in trans-placental passage of the drug that may vary based on maternal serum concentration, maternal plasma protein status and placental blood flow. It is unclear if the placenta has an active or passive role in the transfer of drug to the fetus. The cord blood concentrations of the drug do not always correlate with maternal therapeutic concentrations or the infants’ effects of metabolic acidosis. Non-anion gap metabolic acidosis is the common form of acidosis with acetazolamide but there may be some contribution of lactic acid abnormalities especially if the drug influences the mitochondrial carbonic anhydrase V [22]. The effects on the newborn may manifest as tachypnea and respiratory abnormalities that usually bring this problem to medical attention. However, it is reassuring that the effects of the drug are transient and the newborn infant adapts very quickly; and despite continuing maternal use of the drug and breastfeeding there were no lasting effects on the newborn infant both in the immediate newborn period and on their 2 year follow-up. However, the teratogenic risk of acetazolamide is still in question as one of our cases had an otherwise unexplained congenital anomaly. We, therefore, recommend cautious use of acetazolamide in pregnant women or those planning to get pregnant and close observation of newborn infants born to women on chronic acetazolamide therapy.
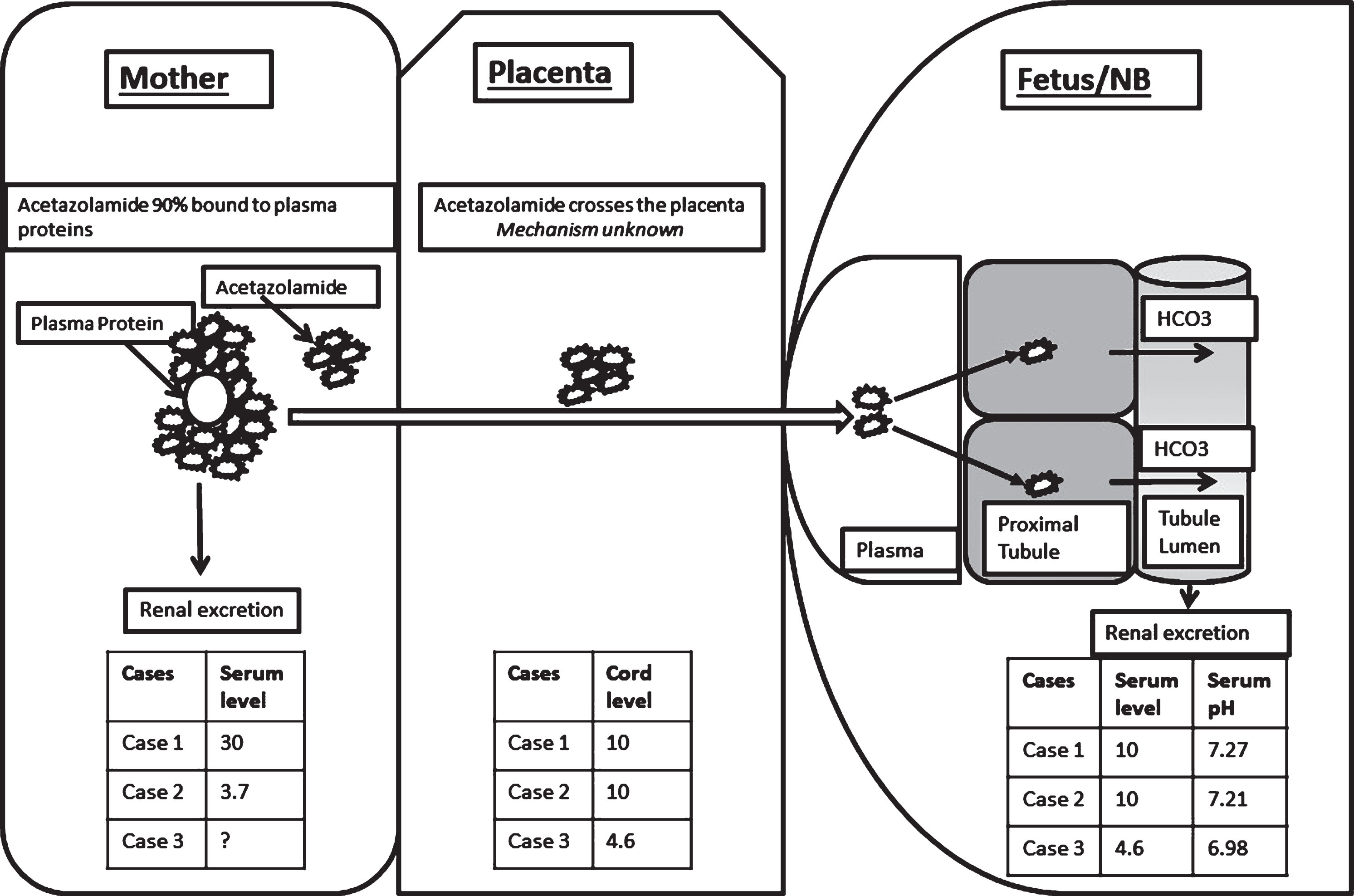
Distribution of acetazolamide in maternal-placental-fetal compartments: Serum concentrations of acetazolamide in mother’s blood, placental or umbilical cord blood and fetal or neonatal blood are correlated with data from three mother-infant dyads. Potential pharmacodynamic mechanisms involved in drug distribution between maternal and infant blood and effects of the drug on renal excretion of bicarbonate are illustrated.
A major limitation of this report is that it is based on observational data from a limited set of patients. There was no systematic collection of information on a cohort of mothers using acetazolamide during pregnancy. Hence, the inferences drawn from our study are limited and highlight the need for a systematic review from a larger dataset.
Disclosures
Financial disclosure statement: The authors have no potential or actual financial interests related to this work.
Conflict of Interest statement: The authors have no conflict of interests to declare.