
Abstract
BACKGROUND:
Extremely preterm infants are peculiar in regard to their risk of retinopathy of prematurity (ROP). In this study, we aim to study insults that may affect extremely preterm infants, including prenatal, at birth, and postnatal insults and their effect on the development of ROP.
METHODS:
This study used the data from Prematurity and Respiratory Outcomes Program (PROP). All included infants with a gestational age of 23 0/7 to 28 6/7 weeks using best obstetrical estimate. We included stressful events and/or modifiable variables that may affect the normal development. We used multiple regression analysis in our statistical analysis.
RESULTS:
We included a total of 751 infants in our study. The mean birth weight for the included sample was 915.1 (±232.94) grams. 391 (52.1%) Infants were diagnosed with ROP. We found a significant negative correlation between ROP development and birth weight (p < 0.001), with a correlation coefficient of – 0.374. We found that the need for prophylactic indomethacin (OR 1.67), the occurrence of air leaks (OR: 2.35), ventilator-associated pneumonia (OR: 2.01), isolated bowel perforations (OR: 3.7), blood culture-proven sepsis (OR: 1.5), other infections (OR: 1.44), and receiving ventricular shunt (OR: 2.9) are significantly associated with the development of ROP.
CONCLUSIONS:
We believe this study included the largest number of factors studied in the largest sample of extremely premature infants. We recommend a screening program for extremely preterm infants that takes into account a scoring system with higher scores for complicated condition.
Introduction
Retinopathy of prematurity (ROP) is defined as a biological developmental process of the retina in premature infants, and is considered among the foremost serious and most dangerous complications in premature infants [1]. Embryonic retinal arteries begin to grow at the end of first trimester of gestation and their development is complete at term. Therefore, the phases of evolution of the eye are underdeveloped in premature infants, and the growth of the vessels is either ceased or unusual, and ultimately, the vessels become very frangible, which might result in visual impairment in severe cases [2]. The earliest incidences of ROP were noticed within the forties and fifties of the past century, primarily as a result of the use of supplemental oxygen without control (1st epidemic). Although the survival of premature infants improved in the following decades, and despite improved monitoring methods for oxygen supplements, ROP emerged with an increasing incidence (2nd epidemic) [3]. ROP has variable risk factors, but the two major well-known risk factors are the gestational age (GA) and birth weight (BW). The multicenter study of cryotherapy for ROP (CRYO-ROP) followed 4,099 infants with BW≤1251 g and reported that lower BW and younger GA were strongly associated with developing ROP [4]. Several other risk factors emerged afterwards with variable contribution to the development of ROP [5]. Extremely preterm infants, born before 28 6/7 weeks of gestational age, tend to have some peculiarities that are not common in older, more mature infants. These include the exposure to stressful events that are not common in mature infants, including cardiorespiratory events [6]. Moreover, previous studies also confirmed that the course of ROP in extremely preterm infants also differs, with ROP beginning in the nasal retina more commonly than in mature infants [7]. It is now proposed that any insult from preterm, to birth, till complete maturation will pre-dispose to ROP [8]. As a result, the lower gestational age increases the duration of infants’ exposure to adverse postnatal insults, contributing to an increased risk of ROP [5]. In this study, we aim to study insults that may occur to extremely preterm infants, including prenatal, at birth, and postnatal insults and their effect on the development of ROP.
Subjects and methods
This study used the data of Prematurity and Respiratory Outcomes Program (PROP), which was a prospective cohort multicenter study of respiratory outcomes of preterm infants in the United States. The PROP was performed by a consortium of six clinical centers (incorporating tertiary neonatal intensive care units [NICU] at 13 sites) and a data-coordinating center working in collaboration with the National Heart Lung Blood Institute (NHLBI). Each clinical center contributed subjects to the study, enrolling infants with gestational ages 23 0/7 to 28 6/7 weeks. The study was waived from institutional review board (IRB) approval as it used open-access data. Inclusion criteria include: gestation age of 23 0/7 to 28 6/7 using best obstetrical estimate, 7 days of age or less at enrollment, and ROP examination done before discharge. Exclusion criteria include: concern for viability, structural abnormality or congenital malformation that might adversely affect life expectancy, and unavailability for long term follow up.
Variables
We included all variables that may be considered as a “stressful” event and are modifiable or may affect the normal development, including: maternal and infant demographics, clinical data and co-morbidities, and infants’ respiratory, nutritional, and medication data throughout the NICU stay. Clinical data were available from birth throughout NICU stay with at least a weekly follow up and at discharge. We used the following variables in the current study.
Prenatal and perinatal factors
Maternal diabetes during pregnancy, maternal hypertension during pregnancy, maternal asthma during pregnancy, placental abruption, clinical chorioamnionitis, and receiving antenatal corticosteroids.
At birth factors
Stabilization procedures provided at birth, continuous positive pressure ventilation (CPAP), supplemental oxygen, non-invasive positive pressure ventilation with flow inflating or self-inflating bag, T-piece resuscitator, intubation, chest compression, and cardiac drugs (epinephrine).
Post-natal pre-discharge factors
Surfactant administration, prophylactic indome-thacin given within the first 24-hours of life, air leaks (i.e. pulmonary interstitial emphysema, pneumothorax, pneumomediastinum, pneumopericardium, pneumoperitoneum, subcutaneous emphysema, and systemic air embolism), pulmonary hemorrhages, clinical diagnosis of patent ductus arteriosus (PDA), ventilator-associated pneumonia (VAP), necrotizing enterocolitis (NEC) Bell’s stage 2 or 3, isolated bowel perforations not considered to be associated with NEC, blood culture-proven sepsis, culture-proven meningitis, upper respiratory tract infection, urinary tract infection, cellulitis, other infections, and receiving a ventricular shunt.
Statistical analysis
We used SPSS version 21.0 (Chicago, USA) in our analysis. We used mean (±standard deviation) to describe continuous variables (i.e., age and measurements). We used count (frequency) to describe other nominal variables (e.g., gender). We used Kendall Tau test to analyze the association of ROP development and birth weight, and we used Spearman test to analyze the correlation between worst ROP stage in each eye with birth weight. We adopted a model-building strategy to analyze the factors associated with the development of ROP, where we performed Chi-square test to analyze the association between ROP and any prenatal and postnatal events that may occur to very preterm infants. Events with significant association with ROP were further included in a logistic regression model with diagnosis of ROP being the dependent variable, and we presented the results in Odds Ratio (OR) and their 95% confidence intervals (CI). We didn’t include BW in the regression analysis, as BW is likely to be a proxy for gestational age and not an independent risk factor [9]. All assumptions were tested and met, and a p value of < 0.05 was taken as significant.
Results
Of the total 835 infants originally included in the PROP study, 751 had an ROP examination prior to discharge and were included in our study. They were 387 (51.5%) males and 364 (48.5%) females. The mean BW for the included sample was 915.1(±232.94) grams, and the mean head circumference was 24.7 cm (±10.21). 391 (52.1%) infants were diagnosed with ROP (Table 1 details the characteristics of ROP in these infants). We found a significant negative correlation between ROP development and BW (p < 0.001), with a correlation coefficient of – 0.374. We also found a negative significant correlation between worst ROP stage in right and left eyes with BW (p < 0.001 for both eyes), with a correlation coefficient of – 0.477 and – 0.485, respectively. All perinatal events that were significantly associated with ROP were inputted into the regression analysis, including CPAP (p < 0.001), indomethacin (p < 0.001), air leak (p = 0.003), PDA (p < 0.001), pulmonary hypertension (p < 0.001), VAP (p = 0.003), bowel perforation (p < 0.001), sepsis (p < 0.001), other infections (p < 0.001) and ventricular shunt (p = 0.006). The regression analysis yielded the significant independent variables associated with ROP (independent predictors of ROP), which are detailed in Figure 1. The model was robust as found by Hosmer and Lemeshow test (p = 0.111) with Nagelkerke R square of 0.134 and the overall model accuracy was 64.2%.
The characteristics of retinopathy of premature in our included sample of extremely preterm infants
The characteristics of retinopathy of premature in our included sample of extremely preterm infants
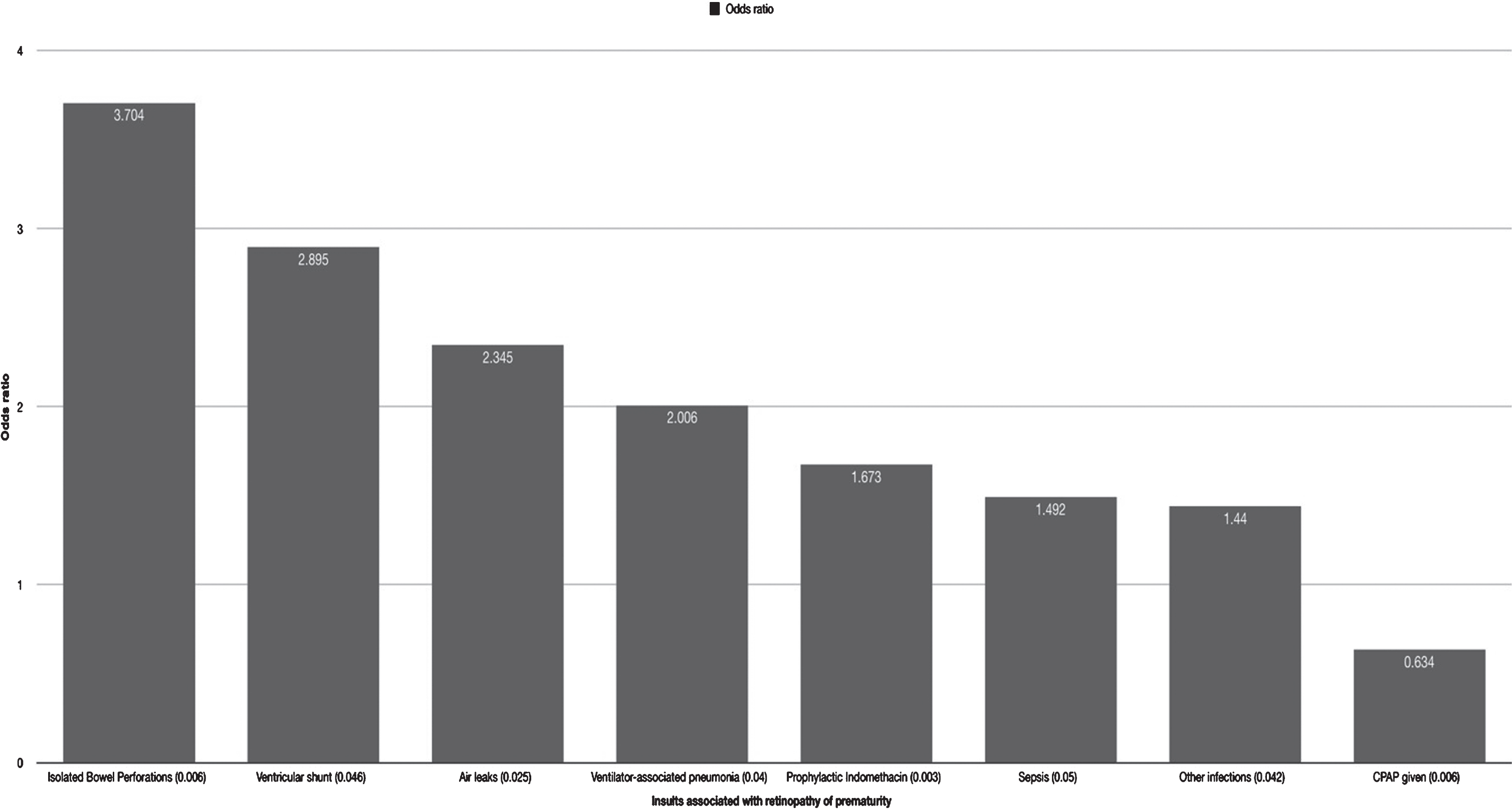
Details of the significant variables as found in the regression model with their respective odds ratio.
During their stay in the NICU, extremely preterm infants born before 28 6/7 weeks of gestational age may encounter several insults that might predispose them to ROP. We found that the need for prophylactic indomethacin (OR 1.67), the occurrence of air leaks (OR: 2.35), VAP (OR: 2.01), isolated bowel perforations (OR: 3.7), blood culture-proven sepsis (OR: 1.5), other infections (OR: 1.44), and receiving ventricular shunt (OR: 2.9) are significantly and independently associated with the development of ROP. On the other hand, receiving CPAP at birth is significantly (p = 0.006) protective against the development of ROP (OR: 0.63). Multiple ROP-predicting tools have been developed, almost all of which depend on BW and GA [10–13]. Recent studies showed that ROP-predicting tools have lower accuracy in extremely preterm infants, which can drop by 50% in this group compared to infants with gestational age above 30 weeks [14]. Considering that all predictive tools include GA and BW during risk calculation, there is a need to examine other risk factors in extremely preterm infants that may further increase the risk of ROP. Moreover, predicting tools that consider postnatal weight gain have better accuracy [12], this points to the importance of the NICU events in predisposing to ROP. One study included stressful events in infants with gestational age below 32 weeks [15]. Although they only retrospectively assessed few events, namely; respiratory distress syndrome, bronchopulmonary dysplasia, sepsis, intraventricular hemorrhage (IVH), and NEC, they found that assessing these risk factors and including them in infants’ assessment for ROP would reduce the infant eligibility for screening by 29%. In our study, we included infants who are extremely preterm, with a prospective weekly follow up, and with assessment of more than 30 variables that may predispose to ROP. Our findings are consistent with most studies which proved that ROP has a great association with lower BW and GA [16–19]. Infants with extremely low BW and/or GA age are at risk of worse ROP outcomes [20, 21], and are at higher need for treatment than other preterm infants [22]. Moreover, some studies compared small-for-gestational age with appropriate-for-age preterm infants, and found higher risk of ROP in the former group [23]. Reynolds et al. explained ROP as a cause of poor tissue oxygenation due to underdeveloped pulmonary function which consequently leads to abnormal retinal vasculature and cellular damage [24]. Previous studies found that NEC, sepsis, and IVH are predisposing factors for ROP [4, 15], although these and other factors were either retrospectively reviewed, or were not followed in a regular fashion as in our analysis. In this study, we also found that sepsis is an important risk factor, but instead of NEC and IVH, we found that bowel perforation and the need for intraventricular shunt, regardless of the indication, are more important risk factors to consider. While isolated perforated bowel has never been assessed one-to-one with ROP, our study revealed that ROP can be a potential outcome of isolated bowel perforation more than other gastroenterology-related factors. NEC is believed to cause ROP via increasing amount of inflammatory and angiogenic factors in the blood stream [25, 26]. Our finding of isolated bowel perforation may have a comparable underlying pathogenesis to develop ROP. Though, the literature lacks assessment of ROP and ventricular shunt, IVH was found to have great association with ROP [17]. Our study found that infants who received ventricular shunts had one of the significant risk factors for ROP. Indomethacin is an independent risk factor for ROP [27, 28], and Fortes Filho et al. found that PDA has a lower risk for ROP than indomethacin [21]. Although some studies found males to be at higher risk for ROP and for worse clinical progression than females [17], this study showed no gender or eye-side preference, in consistence with other landmark studies [17]. The effect of CPAP on the development of ROP is controversial, where some studies, including ours, found the use of CPAP to be protective against the development of ROP, mainly due to a reduced need for mechanical ventilation and lowering oxygen saturation goals [29–31], other studies found the use of CPAP to be a predisposing factor to ROP [17, 33]. In a previous study done on infants below 30 weeks gestational age, they found that the only two factors associated with the development of ROP were exposure to any surgery or maternal exposure to magnesium [34]. Another study, that enrolled infants born before 34 weeks gestational age, found that having IVH and formula feeding are the only factors significantly increasing the risk of ROP [11].
Although the data used in this study have several strength points, including its prospective design with weekly follow up and a large sample of accurately-recruited extremely preterm infants, it didn’t assess the studied variables in very preterm infants, restricting the generalizability of our findings. Moreover, we didn’t assess the severity of ROP in terms of its stages and the involved parts of the retina.
In conclusion, we identified several events that may occur to extremely preterm infants during their NICU stay and might compromise vascular tissue perfusion after birth and thus lead to ROP. These factors should be considered in future ROP-predicting tools, especially among extremely. We recommend a screening program for extremely preterm infants that takes into account a scoring system with higher scores for complicated conditions.
Disclosure statements
Conflict of interest
None
Data availability
Data used in this study are available at BioLINCC: https://biolincc.nhlbi.nih.gov/studies/prop/?q=prop
Footnotes
Acknowledgments
The authors wish to thank the original investigators of the PROP study and the National Heart, Lung, Blood Institute for providing the data free of charge for research purposes.